Find out Blood Group of your own Bloof Find out abnormal Constituments quring Sample
Checking Date & Time
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Loading Image
Here is a comprehensive answer to both practical questions — blood grouping and abnormal constituents of urine — drawn from authoritative medical textbooks.
🩸 Part 1: Finding Your Blood Group (ABO & Rh Typing)
What Is Blood Grouping?
Blood groups are determined by antigens (carbohydrate or protein molecules) on the surface of red blood cells. The two most clinically important systems are:
- ABO system — based on A and B antigens
- Rhesus (Rh) system — based on the RhD protein
ABO Blood Group System
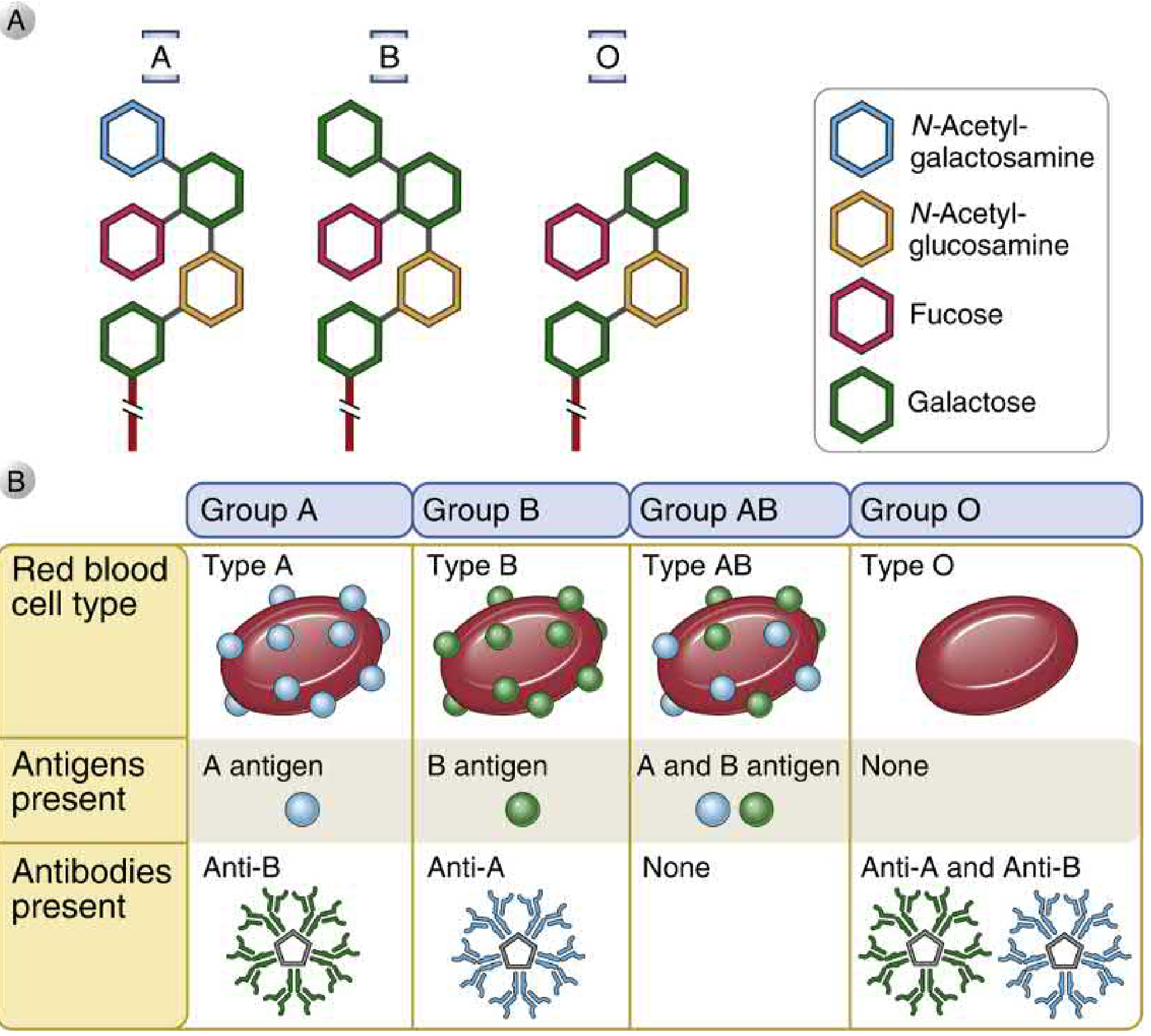
Figure: ABO blood group antigen structures (top) and the corresponding antigens/antibodies present in each blood type (bottom). — Cellular and Molecular Immunology
The Molecular Basis
| Blood Type | Genotype(s) | Antigen on RBC | Natural Antibody in Serum |
|---|---|---|---|
| A | AA or AO | A antigen | Anti-B (IgM) |
| B | BB or BO | B antigen | Anti-A (IgM) |
| AB | AB | A and B antigens | None (universal recipient) |
| O | OO | None (H antigen only) | Anti-A and Anti-B (universal donor) |
The ABO gene on chromosome 9 encodes a glycosyltransferase enzyme:
- A allele → adds N-acetylgalactosamine to the H antigen → creates A antigen
- B allele → adds galactose → creates B antigen
- O allele → encodes a non-functional enzyme; only the H antigen remains
Bombay phenotype (Oh): A rare condition where the fucosyltransferase that makes the H antigen is absent. These individuals cannot produce H, A, or B antigens and make antibodies against all three.
Rhesus (Rh) Blood Group System
The RhD protein is the main antigen tested clinically. It is a non-glycosylated, hydrophobic cell surface protein found in RBC membranes.
- Rh-positive: expresses RhD antigen (~85% of population)
- Rh-negative: has a deletion/alteration of the RhD allele (~15% of population); will make anti-RhD antibodies if exposed to Rh+ blood
Clinical Significance of Rh:
- Transfusion reactions if Rh− patient receives Rh+ blood
- Hemolytic disease of the fetus and newborn (erythroblastosis fetalis): occurs when an Rh− mother carries an Rh+ fetus; maternal IgG anti-RhD crosses the placenta in subsequent pregnancies
- Prevention: Anti-RhD immunoglobulin (Rhogam) is given to the Rh− mother within 72 hours of the first Rh+ delivery to prevent sensitization
How to Determine Your Blood Group (Lab Procedure)
Forward Typing (Cell Grouping)
Patient RBCs are mixed with:
- Anti-A serum → agglutination = A antigen present
- Anti-B serum → agglutination = B antigen present
- Anti-D serum → agglutination = Rh positive
Reverse Typing (Serum Grouping)
Patient serum is mixed with:
- Known A cells → agglutination = anti-A present
- Known B cells → agglutination = anti-B present
| Forward Typing | Reverse Typing | Blood Group |
|---|---|---|
| Agglutination with Anti-A only | Agglutination with B cells | A |
| Agglutination with Anti-B only | Agglutination with A cells | B |
| Agglutination with both | No agglutination | AB |
| No agglutination | Agglutination with both A and B cells | O |
Forward and reverse results must match. A discrepancy indicates an error or a rare variant.
🧪 Part 2: Abnormal Constituents Found During Urine Examination (Urinalysis)
Normal urine contains water, urea, creatinine, electrolytes, and trace amounts of other substances. The following are abnormal findings:
A. Abnormal Chemical Constituents (Dipstick Test)
| Abnormal Constituent | Normal | What It Indicates |
|---|---|---|
| Protein (Proteinuria) | Absent | Glomerulonephritis, nephrotic syndrome, UTI, preeclampsia |
| Glucose (Glucosuria) | Absent | Diabetes mellitus (blood glucose >180 mg/dL), renal tubular disease |
| Ketones (Ketonuria) | Absent | Diabetic ketoacidosis, starvation, prolonged vomiting |
| Blood/Hemoglobin (Hematuria) | Absent | UTI, kidney stones, bladder cancer, trauma, glomerulonephritis |
| Bilirubin | Absent | Obstructive jaundice, hepatocellular disease |
| Urobilinogen (excess) | Trace | Hemolytic anemia, hepatic disease |
| Nitrites | Absent | Bacterial UTI (gram-negative organisms like E. coli) |
| Leukocyte esterase (Pyuria) | Absent | UTI, interstitial nephritis |
Dipstick findings of pyuria + positive nitrites = likely UTI. Gross hematuria should always prompt evaluation to exclude bladder cancer. — Campbell Walsh Wein Urology
B. Abnormal Microscopic Findings (Urine Microscopy)
| Finding | Significance |
|---|---|
| RBCs (>3/HPF) | UTI, stones, cancer, glomerulonephritis |
| WBCs (>5/HPF) | Infection, sterile pyuria (TB, interstitial nephritis) |
| Casts | |
| — Hyaline casts | Non-specific, dehydration |
| — RBC casts | Glomerulonephritis (pathognomonic) |
| — WBC casts | Pyelonephritis, interstitial nephritis |
| — Granular/waxy casts | Chronic renal disease |
| Bacteria | UTI (>100,000 CFU/mL significant) |
| Crystals | Kidney stones (uric acid, oxalate, cystine, struvite) |
| Epithelial cells (renal tubular) | Tubular injury, acute tubular necrosis |
C. Abnormal Physical Properties
| Property | Abnormal Finding | Cause |
|---|---|---|
| Color | Dark brown/tea-colored | Hemoglobinuria, bilirubinuria |
| Cloudy/turbid | Pyuria, phosphaturia, bacteriuria | |
| Red/pink | Hematuria, myoglobinuria | |
| Smell | Ammonia-like | UTI, urease-producing bacteria |
| Fruity/sweet | Ketonuria (DKA) | |
| pH | <4.5 or >8.0 | Metabolic acidosis, UTI with urease bacteria |
| Specific gravity | >1.030 or <1.001 | Dehydration, diabetes insipidus, SIADH |
| Foam | Persistent foam | Proteinuria |
Key Summary
- Blood group is determined by ABO and Rh antigens on red blood cells, established by forward (cell) and reverse (serum) typing
- AB is the universal recipient; O negative is the universal donor
- Abnormal urine may contain protein, glucose, ketones, blood, bilirubin, and abnormal cells/casts — each pointing to specific disease states
- A simple dipstick + microscopy together give maximum diagnostic information from a urine sample
Sources: Cellular and Molecular Immunology, Campbell Walsh Wein Urology, Tietz Textbook of Laboratory Medicine, Henry's Clinical Diagnosis and Management by Laboratory Methods
This is a shared conversation. Sign in to Orris to start your own chat.