I am intern doctor , please show me all dermatology problem along with pictures their classification, diagnosis, laboratory analysis and treatment.
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Searching Images
psoriasis plaque skin lesion
Reading File
Searching Images
atopic dermatitis eczema rash
Searching Images
acne vulgaris comedones papules pustules face
Searching Images
urticaria hives wheals skin
Searching Images
melanoma skin cancer ABCDE features
Searching Images
tinea fungal ringworm skin infection
Searching Images
scabies mite burrow pruritic rash
Searching Images
herpes zoster shingles vesicular rash dermatomal
Searching Images
vitiligo depigmentation white patches skin
Searching Images
rosacea facial erythema telangiectasia
Here is a comprehensive dermatology reference for intern doctors, covering the major skin conditions with classification, clinical features, diagnosis, laboratory workup, treatment, and clinical photographs.
🩺 Dermatology Reference Guide for Intern Doctors
Sources: Fitzpatrick's Dermatology (Vol. 1 & 2), Andrews' Diseases of the Skin, Dermatology 2-Volume Set 5e
📐 SKIN LESION MORPHOLOGY — The Alphabet of Dermatology
Before diagnosing any skin disease, you must recognize primary lesions:
| Primary Lesion | Size | Topography | Contents |
|---|---|---|---|
| Macule | <1 cm | Flat | Color change only |
| Patch | ≥1 cm | Flat | Color change only |
| Papule | <1 cm | Raised/depressed | Solid |
| Plaque | ≥1 cm | Raised/depressed | Solid |
| Nodule | ≥1 cm | Raised | Solid or fluid |
| Vesicle | <1 cm | Raised | Clear fluid |
| Bulla | ≥1 cm | Raised | Clear fluid |
| Pustule | <1 cm | Raised | Pus |
| Erosion | Variable | Depressed | Loss of epidermis |
| Ulcer | Variable | Depressed | Full-thickness loss |
Reaction Patterns (diagnostic categories):
- Papulosquamous — papules/plaques + scale (psoriasis, lichen planus, tinea)
- Eczematous — vesicles, weeping, lichenification (atopic dermatitis, contact dermatitis)
- Vesiculobullous — blisters (pemphigus, herpes)
- Urticarial — wheals + flare (urticaria)
- Pustular — sterile or infectious pustules (acne, folliculitis)
1. 🔴 PSORIASIS


Classification
| Type | Features |
|---|---|
| Plaque (Chronic) | Most common (80%); well-demarcated erythematous plaques with silvery scale; elbows, knees, scalp, sacrum |
| Guttate | Small drop-like lesions; triggered by streptococcal infection; children & young adults |
| Pustular | Sterile pustules; von Zumbusch (generalized, life-threatening) or palmoplantar |
| Erythrodermic | >90% BSA involved; medical emergency; risk of high-output cardiac failure |
| Inverse (Flexural) | Smooth red plaques in folds (axilla, groin, sub-mammary); no scale |
Epidemiology & Triggers
- Affects 2–3% of the population; onset peaks at 15–30 years (Type I, HLA-Cw6+) and >40 years (Type II)
- Triggers: stress, trauma (Köbner phenomenon), infection (strep), drugs (lithium, beta-blockers, antimalarials), alcohol
Diagnosis
- Clinical: Auspitz sign (pinpoint bleeding on scale removal); Köbner phenomenon
- Biopsy (histology): Acanthosis, uniform elongation of rete ridges, thinning of suprapapillary plate, Munro's microabscesses (neutrophil collections in stratum corneum), parakeratosis
- PASI score: quantifies disease severity (0–72 scale)
Laboratory Analysis
| Test | Purpose |
|---|---|
| Skin biopsy (H&E) | Confirms diagnosis; shows parakeratosis, Munro microabscesses |
| Throat swab/ASO titer | Exclude streptococcal trigger in guttate psoriasis |
| Rheumatoid factor, CCP | Negative (helps differentiate from RA in psoriatic arthritis) |
| HLA-B27 | Positive in ~25% with psoriatic arthritis |
| Metabolic panel/lipids | Psoriasis associated with metabolic syndrome; baseline before biologics |
| Hepatitis B/C, TB screening | Mandatory before starting biologics |
Treatment
| Severity | Treatment |
|---|---|
| Mild (localized) | Topical corticosteroids (1st line); vitamin D analogues (calcipotriol); topical retinoids; coal tar |
| Moderate–Severe | Narrowband UVB phototherapy; PUVA; methotrexate; ciclosporin; acitretin |
| Severe/Biologic era | TNF-α inhibitors (adalimumab, etanercept); IL-17 inhibitors (secukinumab, ixekizumab); IL-23 inhibitors (guselkumab, risankizumab) |
| Scalp | Tar shampoo; topical steroid solutions; calcipotriol/betamethasone foam |
| Nail | Potent topical steroids; intralesional steroids; biologics for resistant cases |
2. 🌿 ATOPIC DERMATITIS (ECZEMA)


Classification
| Phase | Age | Distribution | Features |
|---|---|---|---|
| Infantile | 0–2 years | Face (cheeks), scalp, extensor surfaces | Weeping, crusting, erythematous plaques |
| Childhood | 2–12 years | Flexural creases (antecubital, popliteal fossa) | Lichenification, dry skin, intense pruritus |
| Adult | >12 years | Flexural, hands, face, neck | Thick lichenified plaques, chronic course |
Diagnostic Criteria (Hanifin & Rajka)
Must have ≥3 major + ≥3 minor criteria
Major criteria:
- Pruritus
- Typical morphology and distribution (flexural, facial in infants)
- Chronic or chronically relapsing dermatitis
- Personal or family history of atopy (asthma, allergic rhinitis, atopic dermatitis)
Minor criteria include: xerosis, early age of onset, elevated IgE, food hypersensitivity, ichthyosis, keratosis pilaris, Dennie–Morgan fold (infraorbital fold), white dermographism, facial pallor, perifollicular accentuation, etc.
Laboratory Analysis
| Test | Significance |
|---|---|
| Serum total IgE | Elevated in ~80% of patients |
| Specific IgE (RAST) | Identify allergens: house dust mite, pollens, food (egg, milk, peanut) |
| Skin prick tests | Identify relevant allergens in IgE-mediated sensitization |
| Eosinophil count (CBC) | Often elevated |
| Skin swab (MC&S) | Exclude Staphylococcus aureus superinfection (common flare trigger) |
| Patch testing | Exclude contact allergic dermatitis (especially in adult-onset) |
| Serum TARC (CCL17) | Biomarker for disease activity |
Treatment
| Step | Treatment |
|---|---|
| 1 — Emollients | Cornerstone of all AD therapy; apply liberally throughout day |
| 2 — Mild topical steroids | Hydrocortisone 1% for face; mild-moderate potency for body |
| 3 — Moderate/potent steroids | Used in acute flares; step down quickly to avoid atrophy |
| 4 — Topical calcineurin inhibitors | Tacrolimus (0.03–0.1%) and pimecrolimus for sensitive areas; steroid-sparing |
| 5 — Systemic (moderate-severe) | Cyclosporine (rapid response); methotrexate; azathioprine; mycophenolate |
| 6 — Biologic | Dupilumab (IL-4Rα blocker, FDA-approved); tralokinumab |
| 7 — JAK inhibitors | Upadacitinib; abrocitinib (oral, for moderate-severe) |
| Infections | Topical mupirocin or systemic antibiotics for Staph superinfection; oral acyclovir for eczema herpeticum |
| Antipruritic | Sedating antihistamines (chlorphenamine) at night |
3. 🔴 ACNE VULGARIS


Classification (Global Acne Grading System / Leeds Scale)
| Grade | Features |
|---|---|
| Comedonal | Open (blackheads) and closed (whiteheads) comedones only; no inflammation |
| Mild-Moderate Papulopustular | <20 papules/pustules; minimal nodules |
| Moderate-Severe | >20 papules/pustules; nodules; may affect trunk |
| Nodulocystic / Acne Conglobata | Large nodules, cysts, abscesses, sinus tracts; significant scarring risk |
| Acne Fulminans | Explosive onset, systemic symptoms, fever; treat as emergency |
Pathogenesis (4 key factors)
- Follicular hyperkeratinization → comedone formation
- Excess sebum production (stimulated by androgens)
- Cutibacterium acnes colonization
- Inflammation (IL-1, TNF-α, IL-17)
Diagnosis
- Clinical: identify lesion types (comedones, papules, pustules, nodules, cysts)
- Always ask about: drug history (lithium, phenytoin, steroids, androgens), menstrual cycle (hormonal acne)
- Investigations usually not needed, but consider:
Laboratory Analysis
| Test | Indication |
|---|---|
| Hormonal panel (LH, FSH, DHEAS, free testosterone) | Female patients with irregular cycles, hirsutism, PCOS |
| ACTH stimulation test | Exclude late-onset congenital adrenal hyperplasia |
| Pregnancy test (urine hCG) | Before isotretinoin; mandatory |
| Fasting lipids + LFTs | Before and during isotretinoin |
| Swab for MC&S | Exclude gram-negative folliculitis (treatment-resistant or post-antibiotics) |
Treatment (Step-Up Approach)
| Grade | Regimen |
|---|---|
| Comedonal | Topical retinoid (tretinoin, adapalene 0.1%) |
| Mild inflammatory | Benzoyl peroxide (BPO) + topical retinoid ± topical antibiotic (clindamycin, erythromycin) |
| Moderate | Above + oral antibiotic (doxycycline 100mg OD x 3 months; avoid tetracyclines <8yrs) |
| Severe/nodulocystic | Isotretinoin 0.5–1 mg/kg/day for 4–6 months (cumulative dose 120–150 mg/kg); teratogenic — iPLEDGE pregnancy prevention required |
| Hormonal acne (females) | Combined OCP (ethinylestradiol + cyproterone); spironolactone 50–200 mg/day |
| Acne fulminans | Oral prednisolone + isotretinoin |
| Post-inflammatory hyperpigmentation | Azelaic acid 20%; hydroquinone; chemical peels |
4. 🔴 URTICARIA (HIVES)


Classification
| Type | Duration | Subtypes |
|---|---|---|
| Acute | <6 weeks | Allergic (IgE), idiopathic |
| Chronic Spontaneous (CSU) | >6 weeks | Autoimmune (anti-FcεRI/anti-IgE antibodies), idiopathic |
| Chronic Inducible | >6 weeks | Dermographism, cold urticaria, pressure urticaria, solar urticaria, aquagenic, cholinergic |
Diagnosis
- Clinical hallmarks: transient wheals (last <24 hours), intense pruritus, no residual skin change
- If wheals persist >24h → consider urticarial vasculitis (requires biopsy)
- Angioedema in ~50%: deeper swelling of lips, tongue, eyelids, genitalia
Laboratory Analysis
| Test | Purpose |
|---|---|
| CBC + differential | Eosinophilia (parasites); exclude blood dyscrasias |
| ESR, CRP | Elevated in urticarial vasculitis or systemic disease |
| Thyroid function + anti-TPO, anti-thyroglobulin | Autoimmune thyroid disease associated with CSU |
| ANA, complement (C3, C4) | Exclude lupus, vasculitis |
| IgE panel / specific allergen RAST | Acute allergic urticaria (food, drug, latex, venom) |
| Autologous serum skin test (ASST) | Screen for autoimmune CSU (IgG anti-IgE antibodies) |
| Skin biopsy | If wheal lasts >24h; exclude urticarial vasculitis |
| Stool O&P, H. pylori serology | Chronic urticaria with parasitic/infectious triggers |
Treatment
| Step | Treatment |
|---|---|
| Identify & remove trigger | Drugs (NSAIDs, ACE inhibitors, antibiotics), foods, infections |
| Step 1 | Non-sedating H1-antihistamine (cetirizine, loratadine, fexofenadine) daily |
| Step 2 | Increase dose up to 4× normal dose (off-label but guideline-supported) |
| Step 3 | Add omalizumab (anti-IgE) 300 mg SC monthly — highly effective in autoimmune CSU |
| Step 4 | Cyclosporine (resistant cases) |
| Acute anaphylaxis | IM epinephrine 0.3–0.5 mg; IV antihistamines; IV corticosteroids |
5. 🟤 TINEA (DERMATOPHYTOSIS)

Classification by Site
| Type | Site | Common Organism |
|---|---|---|
| Tinea corporis | Glabrous (smooth) skin of body | T. rubrum, T. mentagrophytes |
| Tinea pedis | Feet (web spaces, soles, sides) | T. rubrum |
| Tinea unguium (Onychomycosis) | Nails | T. rubrum |
| Tinea capitis | Scalp / hair | T. tonsurans, Microsporum canis |
| Tinea cruris | Groin ("jock itch") | T. rubrum, Epidermophyton floccosum |
| Tinea faciei | Face | T. rubrum |
| Tinea versicolor | Trunk | Malassezia furfur (yeast, not dermatophyte) |
Diagnosis
- Clinical: annular plaque with raised scaly advancing border and central clearing
- Wood's lamp: Microsporum fluoresces green (tinea capitis)
- KOH (potassium hydroxide) preparation: branching hyphae visible under microscopy — gold standard bedside test
- Fungal culture (Sabouraud's dextrose agar): species identification; takes 2–4 weeks
Laboratory Analysis
| Test | Finding |
|---|---|
| KOH prep of skin scraping | Septate branching hyphae |
| Periodic acid–Schiff (PAS) stain on biopsy | Highlights fungal elements in stratum corneum |
| Fungal culture | Species identification; sensitivity testing if resistant |
| Nail clipping histology + culture | DLSO pattern (distal lateral subungual onychomycosis) is most common |
Treatment
| Location | Treatment |
|---|---|
| Tinea corporis / cruris / pedis (limited) | Topical azole (clotrimazole, miconazole) or terbinafine cream 1–4 weeks |
| Extensive / scalp / nail | Oral terbinafine 250 mg/day (nails: 6 weeks fingers, 12 weeks toes); or itraconazole pulse therapy |
| Tinea capitis | Oral terbinafine or griseofulvin 6–8 weeks; selenium sulfide shampoo to reduce shedding |
| Tinea versicolor | Selenium sulfide or ketoconazole shampoo; single-dose oral itraconazole 400 mg for recurrent cases |
6. 🔴 HERPES ZOSTER (SHINGLES)


Classification
| Type | Features |
|---|---|
| Dermatomal (localized) | Classic unilateral band; thoracic most common (T3–L3) |
| Herpes Zoster Ophthalmicus (HZO) | V1 (ophthalmic) division of trigeminal nerve; Hutchinson's sign = tip of nose vesicles → risk of ocular involvement |
| Ramsay Hunt Syndrome | VII (facial) nerve + geniculate ganglion; ear vesicles + ipsilateral facial palsy + hearing loss |
| Disseminated | >2 dermatomes or >20 lesions outside primary dermatome; in immunocompromised patients |
Diagnosis
- Clinical: prodrome of dermatomal pain/burning → grouped vesicles on erythematous base, STRICTLY UNILATERAL, following dermatome
- Tzanck smear: multinucleated giant cells (not specific — VZV vs HSV)
- PCR of vesicle fluid: most sensitive & specific — gold standard
- Direct fluorescent antibody (DFA) test: quick, differentiates VZV from HSV
Laboratory Analysis
| Test | Purpose |
|---|---|
| PCR (vesicle swab) | Confirm VZV, most sensitive |
| DFA staining | Quick bedside differentiation VZV/HSV |
| Tzanck smear | Multinucleated giant cells (quick, non-specific) |
| VZV IgM serology | Acute infection confirmation |
| CBC, HIV test | Young patient or disseminated → exclude immunosuppression |
| Ophthalmology referral + slit lamp | Mandatory in HZO |
Treatment
| Indication | Treatment |
|---|---|
| Start antivirals within 72h of rash | Acyclovir 800 mg 5×/day × 7 days; or Valacyclovir 1g TDS × 7 days (better bioavailability) |
| HZO / Ramsay Hunt / Disseminated | IV acyclovir 10 mg/kg q8h |
| Pain management | NSAIDs; gabapentin/pregabalin; amitriptyline; opioids if severe |
| Post-herpetic neuralgia (PHN) | 1st line: gabapentin/pregabalin; 2nd line: tricyclics; topical lidocaine 5% patches |
| Prevention | Shingrix vaccine (recombinant, adjuvanted) ≥50 years; 97% effective for PHN |
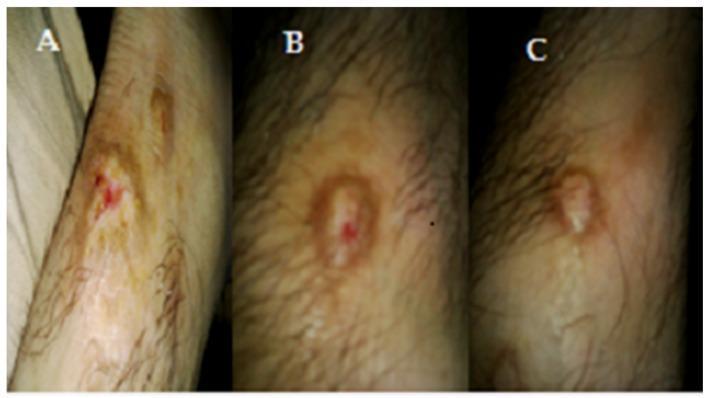
7. 🔵 SCABIES

Classification
| Type | Features |
|---|---|
| Classic Scabies | Intense nocturnal pruritus; burrows in web spaces, wrists, genitalia |
| Crusted (Norwegian) Scabies | Hyperkeratotic crusts; millions of mites; occurs in immunocompromised/elderly; highly contagious |
| Nodular Scabies | Persistent nodules (genital, axillae) after treatment (hypersensitivity reaction) |
| Infant/Elderly | Atypical distribution; may involve face, scalp, palms, soles |
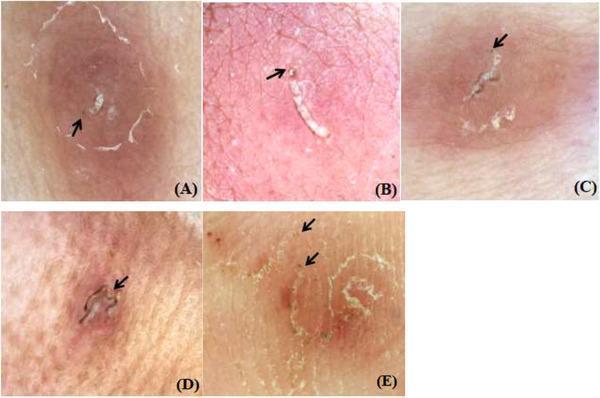
Diagnosis
- Pathognomonic: burrow (serpiginous, thread-like track, 2–15 mm) in finger web spaces
- Dermoscopy: "delta-wing sign" / "jet plane sign" = anterior end of burrow with triangular mite structure
- Skin scraping + microscopy (mineral oil prep): mites, eggs, or fecal pellets (scybala)
Laboratory Analysis
| Test | Finding |
|---|---|
| Skin scraping microscopy | Mite (8-legged), eggs, scybala — confirmatory |
| Dermoscopy | Triangular/delta sign at burrow end |
| Skin biopsy (H&E + PAS) | Mites in stratum corneum tunnel (rarely needed) |
| PCR | Research setting; highly sensitive |
| CBC | Eosinophilia common |
Treatment
| Treatment | |
|---|---|
| First line | Permethrin 5% cream applied neck-to-toe (including under nails); leave overnight; repeat at 7 days |
| Systemic | Oral ivermectin 200 µg/kg; two doses 1–2 weeks apart; preferred for crusted scabies |
| Crusted scabies | Combination: oral ivermectin + topical permethrin + keratolytic (urea cream) |
| Post-scabetic itch | Continues for 2–4 weeks after treatment — does NOT indicate treatment failure |
| Contact management | Treat ALL household contacts simultaneously; wash clothing/bedding at >60°C |
| Symptomatic relief | Oral antihistamines; topical calamine; short course topical steroid for persistent nodules |
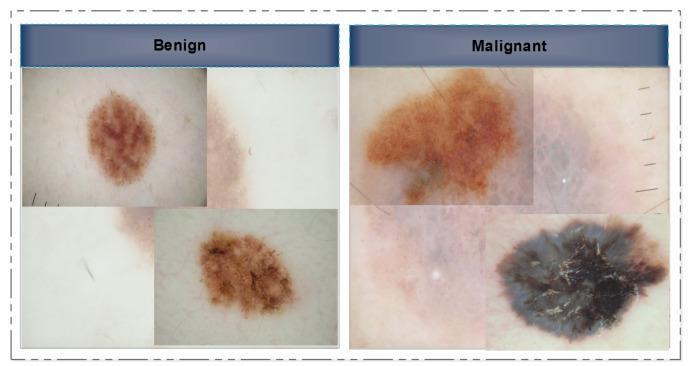
8. ⚫ MELANOMA
Classification (WHO 2022)
| Type | Features | Location |
|---|---|---|
| Superficial Spreading | Most common (70%); grows radially first; irregular pigmentation | Back (M), legs (F) |
| Nodular | Rapid vertical growth; may be amelanotic; worst prognosis | Trunk, head |
| Lentigo Maligna Melanoma | Slow-growing; arises in lentigo maligna; elderly; sun-exposed | Face/head |
| Acral Lentiginous | Palms, soles, subungual; most common in dark skin; aggressive | Acral sites |
| Mucosal | Rare; oral, genital, sinonasal | Mucosae |
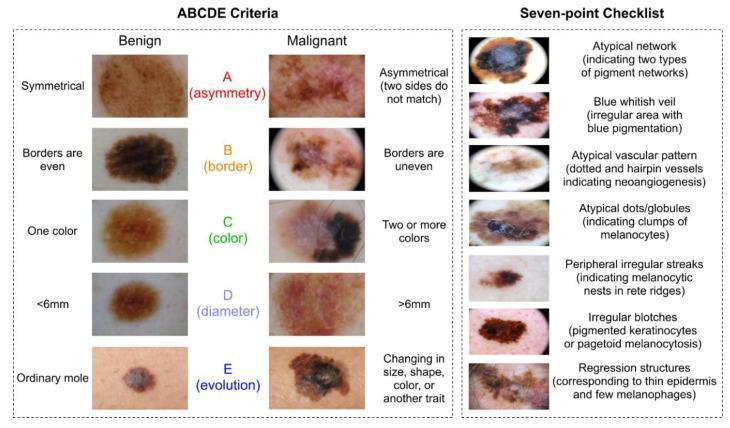
ABCDE Screening Rule
| Letter | Feature |
|---|---|
| A — Asymmetry | One half unlike the other |
| B — Border | Irregular, notched, ragged edges |
| C — Color | Multiple colors (brown, black, red, white, blue) |
| D — Diameter | >6 mm (size of pencil eraser) |
| E — Evolution | Any change in size, shape, color, or new symptoms |
Staging (AJCC 8th ed.)
- T stage based on Breslow thickness (mm depth) and ulceration
- N stage: nodal involvement
- M stage: distant metastasis (M1a skin/LN; M1b lung; M1c visceral; M1d CNS)
Laboratory & Diagnostic Analysis
| Test | Purpose |
|---|---|
| Excision biopsy (full-thickness) | Gold standard — measure Breslow thickness, Clark level, ulceration, mitotic rate |
| Sentinel lymph node biopsy (SLNB) | T1b or thicker; guides staging & prognosis |
| LDH | Elevated in stage IV → poor prognosis |
| CT chest/abdomen/pelvis | Staging for regional/distant metastasis |
| PET-CT | Whole-body staging in advanced disease |
| Brain MRI | Mandatory in stage IV |
| BRAF V600E mutation | In metastatic disease → guides targeted therapy |
| PD-L1 expression | Guides immunotherapy |
Treatment
| Stage | Treatment |
|---|---|
| Stage I–II (localized) | Wide local excision (1–2 cm margins based on Breslow depth) ± SLNB |
| Stage III (nodal) | Surgery + adjuvant immunotherapy (pembrolizumab, nivolumab) or targeted therapy (BRAF+MEK inhibitors if BRAF+) |
| Stage IV (metastatic) | Immunotherapy (ipilimumab + nivolumab); BRAF/MEK inhibitors (vemurafenib + cobimetinib); radiation; clinical trials |
| Lentigo maligna | Mohs surgery or staged excision; imiquimod for non-surgical candidates |
9. ⬜ VITILIGO


Classification
| Type | Features |
|---|---|
| Non-segmental (NSV) | Most common; bilateral, symmetrical; progressive; around eyes, mouth, genitalia, extremities; associated with autoimmune diseases |
| Segmental (SV) | Unilateral; follows dermatomal pattern; early onset; hair depigmentation common; stable after 1–2 years |
| Mixed | Both patterns in same patient |
Diagnosis
- Clinical: well-demarcated chalk-white macules/patches with convex (not concave) borders
- Wood's lamp (365 nm UV): lesions fluoresce bright blue-white (excellent for fair skin)
- Leukotrichia (white hairs within patch) = poor prognosis for repigmentation
Laboratory Analysis
| Test | Purpose |
|---|---|
| Thyroid function tests + anti-TPO | Associated in 20–30%; screen all patients |
| Fasting glucose / HbA1c | Diabetes association |
| ANA | Exclude SLE, other AID |
| CBC | Exclude pernicious anemia (anti-parietal cell antibodies if B12 low) |
| Skin biopsy (melanin stain) | Complete absence of melanocytes (Masson-Fontana stain); rarely needed |
| Ophthalmology review | Uveitis association (especially segmental) |
Treatment
| Category | Treatment |
|---|---|
| Topical (facial/limited) | Potent topical corticosteroids; topical tacrolimus 0.1% (face, flexures) |
| Phototherapy | Narrowband UVB (311 nm) — most effective; 3×/week for 6–12 months; target-NBUVB for localized |
| Systemic | Mini-pulse oral betamethasone (5 mg Saturday + Sunday) to arrest active spreading |
| JAK inhibitors | Ruxolitinib 1.5% cream (FDA-approved 2022 — first approved topical for vitiligo); oral baricitinib |
| Surgical (stable ≥2 yrs) | Split skin grafting; blister grafting; melanocyte-keratinocyte transplant (MKTP); follicular unit extraction |
| Camouflage | Self-tanning creams (DHA); cosmetic camouflage; sunscreen on depigmented skin (high SPF) |
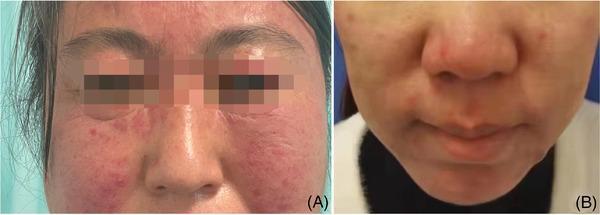
10. 🌹 ROSACEA

Classification (NRS 2017 Subtypes)
| Subtype | Features |
|---|---|
| ETR (Erythematotelangiectatic) | Flushing, persistent central facial erythema, telangiectasias; no papules |
| PPR (Papulopustular) | Erythema + inflammatory papules and pustules; no comedones (differentiates from acne) |
| Phymatous | Skin thickening; rhinophyma (bulbous nose deformity); predominantly in men |
| Ocular | Blepharitis, meibomian gland dysfunction, conjunctivitis, episcleritis; may precede skin rosacea |
Key Features
- Triggers: sunlight, heat, alcohol, spicy food, exercise, emotional stress, Demodex mites
- Central face distribution (cheeks, nose, chin, forehead)
- No comedones (key distinction from acne)
- Flushing (vasomotor instability)
Laboratory Analysis
| Test | Purpose |
|---|---|
| Skin biopsy | Usually not required; shows Demodex mite infestation, perivascular inflammation, sebaceous hyperplasia |
| ANA, dsDNA, complement | Exclude SLE (malar rash looks similar but spares nasolabial folds in lupus) |
| Dermoscopy | Dilated follicles, telangiectasia, Demodex tails |
| Demodex count (surface skin biopsy) | >5 mites/cm² supports Demodex rosacea |
Treatment
| Type | Treatment |
|---|---|
| ETR | Topical brimonidine (vasoconstriction, 3–6 h effect); topical oxymetazoline; laser/IPL for telangiectasia |
| PPR | Topical ivermectin 1% cream (anti-Demodex, anti-inflammatory — 1st line); topical metronidazole 0.75%; topical azelaic acid 15% |
| PPR systemic | Doxycycline 40 mg MR (sub-antimicrobial dose, anti-inflammatory) — 1st line oral |
| Phymatous | CO₂ laser ablation; surgical shave; electrosurgery |
| Ocular | Lid hygiene; topical cyclosporine eye drops; oral doxycycline |
| General | Sun protection (SPF 30+); avoid triggers; gentle skincare |
📊 QUICK DIFFERENTIAL DIAGNOSIS TABLE
| Feature | Psoriasis | Eczema | Tinea | Rosacea | SLE Malar |
|---|---|---|---|---|---|
| Scale | Silvery, thick | Fine, weeping | Peripheral, advancing | None | None/fine |
| Distribution | Extensor | Flexural | Annular spreading | Central face | Malar, spares nasolabial folds |
| Pruritus | Mild | Intense | Mild-moderate | Burning | Mild |
| KOH | Negative | Negative | Positive (hyphae) | Negative | Negative |
| Biopsy hallmark | Munro microabscesses | Spongiosis | Hyphae in corneum | Demodex, dilation | Interface dermatitis, IgG deposits |
| Koebner | Yes | Yes | No | No | No |
🧪 COMMON DERMATOLOGY LAB TESTS AT A GLANCE
| Test | Key Diseases |
|---|---|
| KOH prep | Tinea, candidiasis, tinea versicolor |
| Tzanck smear | HSV, VZV (multinucleated giant cells) |
| Patch test | Allergic contact dermatitis |
| Skin prick test | Urticaria, atopic dermatitis (allergens) |
| Skin biopsy H&E | Most inflammatory and neoplastic disorders |
| DIF (Direct Immunofluorescence) | Pemphigus (IgG fish-net pattern), pemphigoid (IgG linear), dermatitis herpetiformis (IgA granular) |
| Wood's lamp | Vitiligo (blue-white), tinea capitis Microsporum (green), erythrasma (coral-pink) |
| Dermoscopy | Melanoma, scabies, psoriasis, lichen planus |
| RAST / specific IgE | Urticaria, atopic dermatitis allergen profiling |
| ANA, dsDNA, anti-Sm | Lupus erythematosus |
| Anti-desmoglein 1 & 3 | Pemphigus vulgaris/foliaceus |
| Anti-BP180, anti-BP230 | Bullous pemphigoid |
Sources: Fitzpatrick's Dermatology Vols 1 & 2 (9780071837781), Andrews' Diseases of the Skin Clinical Dermatology (9780323547536), Dermatology 2-Volume Set 5e (9780702082252). Clinical photographs from DermNetNZ and PMC Clinical VQA datasets.
Clinical Pearl for Interns: Always describe skin lesions systematically — morphology → distribution → secondary changes → associated symptoms. This approach will generate your reaction pattern and narrow your differential before ordering any test.
This is a shared conversation. Sign in to Orris to start your own chat.