2. Maternal Mortality in India Status, causes, prevention, national program provisions. Help me to write 10 mark answer on topic 2. Maternal Mortality in India Status, causes, prevention, national program provisions. from book k park mbbs 3 rd year Arrange the answer properly Highlight words or sentence Add flow chart where needed neededgive the answer from above paragraph only And answer should me impressive to the examiner who is my hod of community who will cheak my answer sheet as I have to write it in my university exams to score full marks
MATERNAL MORTALITY IN INDIA
Status, Causes, Prevention and National Programme Provisions
DEFINITION
"The death of a woman while pregnant or within 42 days of termination of pregnancy, irrespective of the duration and site of pregnancy, from any cause related to or aggravated by the pregnancy or its management but not from unintentional or incidental causes."
TYPES OF MATERNAL DEATHS
| Type | Definition |
|---|---|
| Direct obstetric deaths | Due to obstetric complications of pregnancy, labour, puerperium (e.g., haemorrhage, eclampsia, sepsis) |
| Indirect obstetric deaths | Pre-existing or newly acquired disease aggravated by pregnancy (e.g., cardiac disease, anaemia) |
| Late maternal deaths | Death from direct/indirect causes after 42 days but within 1 year of termination of pregnancy |
I. STATUS OF MATERNAL MORTALITY IN INDIA
| Category | MMR (per 1,00,000 live births) |
|---|---|
| India (Total) | 113 |
| EAG States + Assam | 161 |
| Assam | 215 (highest) |
| Uttar Pradesh | 197 |
| Madhya Pradesh | 173 |
| Rajasthan | 164 |
| Kerala | 43 (lowest) |
| Southern States | ~65-92 |
- Trend: MMR declined from 167 (2011-13) to 113 (2016-18) per 1,00,000 live births.
- States of Kerala, Maharashtra, Andhra Pradesh, Gujarat and Tamil Nadu have already achieved the SDG goal of MMR < 100 per 1,00,000 live births.
- The lifetime risk of maternal death is 0.3% nationally but 0.5% in EAG + Assam states.
SDG Target 2030: Reduce global MMR to less than 70 per 1,00,000 live births.
II. CAUSES OF MATERNAL MORTALITY
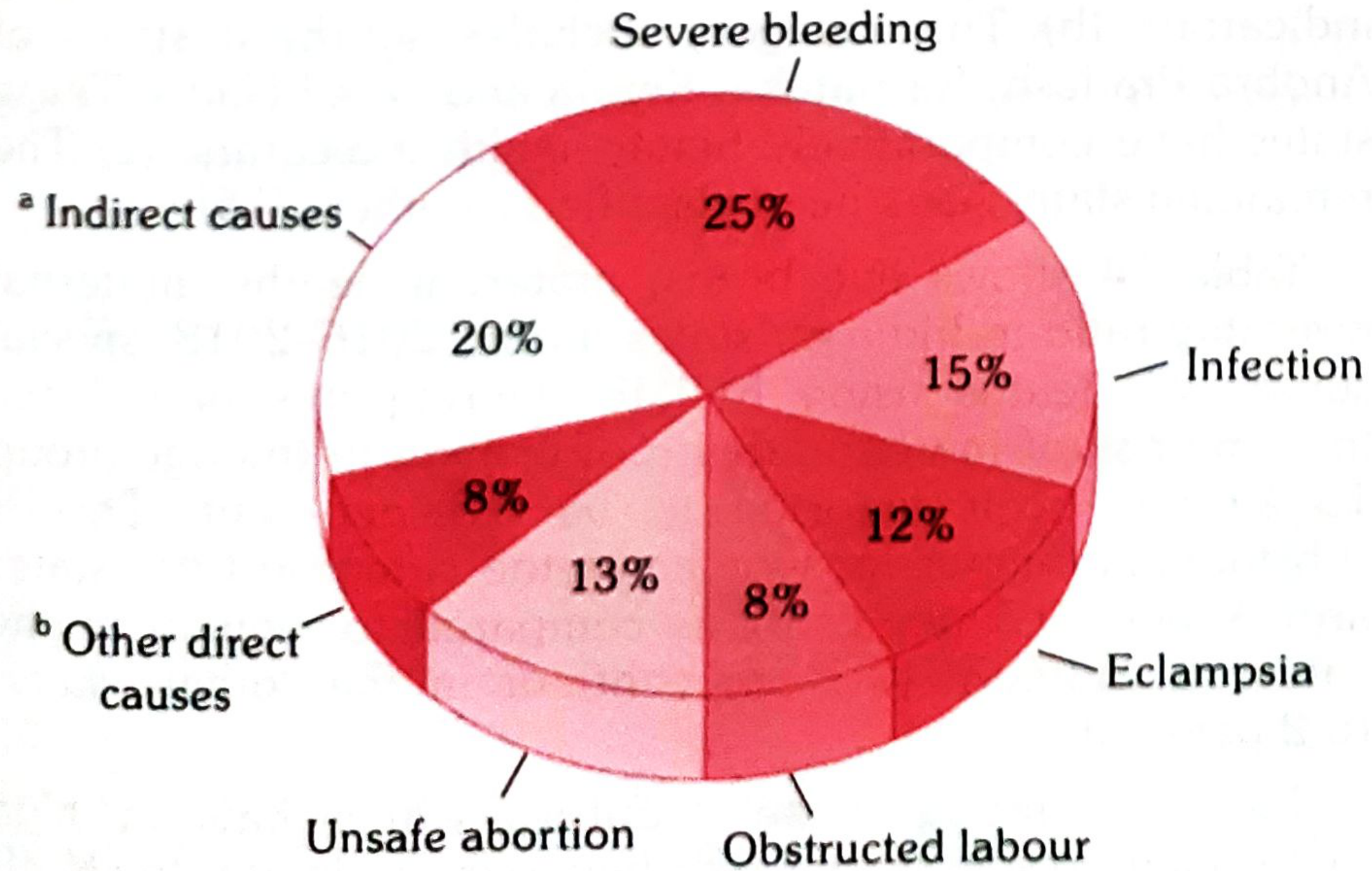
Global Causes (Pie Chart from Park's)
A. MEDICAL CAUSES
| Cause | % of Deaths |
|---|---|
| Haemorrhage (Severe Bleeding) | 25% (most common) |
| Infection / Puerperal sepsis | 15% |
| Eclampsia / Hypertensive disorders | 13% |
| Obstructed labour | 8% |
| Unsafe abortion | 13% |
| Other direct causes | 8% |
| Indirect causes | 20% |
- Anaemia (most significant - affects ~50% of pregnant women)
- Cardiac and renal disease
- Hepatitis, Tuberculosis, Malaria
- Metabolic and endocrine disorders
- Malignancy
B. SOCIAL CAUSES (Determinants of Maternal Mortality in India)
SOCIAL DETERMINANTS
|
|-------- Age: Optimal childbearing age 20-30 years
| (Extremes of age = higher risk)
|
|-------- Parity: High parity → high MMR
|
|-------- Birth Interval: Short intervals → increased risk
|
|-------- Malnutrition, Poverty, Illiteracy
|
|-------- Ignorance, prejudices, cultural beliefs
|
|-------- Delivery by untrained dais
|
|-------- Poor transport and communication facilities
|
└-------- Low level of women's empowerment
III. PREVENTION OF MATERNAL MORTALITY
- Early registration of pregnancy
- At least 4 antenatal check-ups (ANC)
- Dietary supplementation including correction of anaemia
- Prevention of infection and haemorrhage during puerperium
- Prevention of complications - eclampsia, malpresentations, ruptured uterus
- Treatment of medical conditions - hypertension, diabetes, tuberculosis
- Anti-malaria prophylaxis and tetanus toxoid
- Clean delivery practices
- Training and use of village-level health workers (ASHA)
- Institutional deliveries for women with risk factors / bad obstetric history
- Family planning - not more than 2 children, proper spacing of births
- Identification and audit of every maternal death to find its cause
- Provision of safe abortion services
IV. NATIONAL PROGRAMME PROVISIONS
FLOWCHART: National Programmes for Reducing MMR
NATIONAL PROGRAMMES TO REDUCE MATERNAL MORTALITY
|
___________________|___________________
| | | | |
JSY JSSK PMSMA SUMAN LaQshya
(2005) (2011) (2016) (2019) (2017)
| | | | |
Cash Free Free ANC Zero Quality
assist. delivery on 9th of denial labour
for + free every policy room care
inst. transport month
delivery
1. JANANI SURAKSHA YOJANA (JSY) - Launched 12 April 2005
- 100% centrally sponsored scheme under National Rural Health Mission (NRHM)
- Objective: Reduce MMR and neonatal mortality by encouraging institutional deliveries
- Targets BPL women (both rural and urban)
- ASHA works as a link worker between pregnant women and health institutions
- Cash assistance:
| Category | Rural (Mother + ASHA) | Urban (Mother + ASHA) |
|---|---|---|
| LPS (Low Performing States) | Rs. 1400 + 600 = Rs. 2000 | Rs. 1000 + 400 = Rs. 1400 |
| HPS (High Performing States) | Rs. 700 + 600 = Rs. 1300 | Rs. 600 + 400 = Rs. 1000 |
- 10 Low Performing States: UP, Uttarakhand, MP, Jharkhand, Bihar, Rajasthan, Chhattisgarh, Odisha, Assam, J&K
2. JANANI-SHISHU SURAKSHA KARYAKRAM (JSSK) - Launched 1 June 2011
- Free delivery including Caesarean section
- Free drugs and consumables
- Free diet - up to 3 days (normal delivery), up to 7 days (C-section)
- Free diagnostics and free blood
- Free transport - home to institution, inter-facility referral, and drop-back home
- Similar entitlements for sick newborns up to 30 days after birth
- Benefits an estimated 12 million pregnant women per year
3. PRADHAN MANTRI SURAKSHIT MATRITVA ABHIYAN (PMSMA) - Launched June 2016
- Provides fixed-day, free-of-cost, quality ANC to all pregnant women
- ANC services provided on the 9th of every month at government facilities
- Minimum package includes investigations and drugs
- Involves private sector doctors as volunteers
- Over 2.20 crore ANC check-ups conducted
- More than 11.66 lakh high-risk pregnancies identified
4. SUMAN (Surakshit Matritva Aashwasan) - Launched 10 October 2019
- Provides assured, dignified, respectful and quality healthcare at zero cost
- Zero tolerance for denial of services to any woman or newborn at public facilities
- Target: Zero preventable maternal and newborn deaths
5. LaQshya PROGRAMME - Launched 2017
- Improves quality of care in labour rooms and maternity OTs in public facilities
- Evidence-based approach for maternal and newborn care
- Implemented at District Hospitals, Sub-district Hospitals, CHCs, FRUs and Medical Colleges
- 2,445 public health facilities identified under LaQshya
- Ensures respectful maternity care during the most vulnerable periods
6. OTHER STRATEGIES
- Maternal Death Review (MDR): Facility and community-based audit - important strategy to improve quality of obstetric care
- Pregnancy Tracking / Mother and Child Tracking System (MCTS)
- Village Health and Nutrition Day (VHND): Monthly at anganwadi centres for ANC, immunization, family planning
- RMNCH+A Strategy (Reproductive, Maternal, Neonatal, Child and Adolescent Health)
- Anaemia Mukt Bharat Programme - addresses anaemia in pregnant women
- Establishment of First Referral Units (FRUs) for emergency obstetric care
- Safe abortion services under MTP Act 1971 including MVA technique
CONCLUSION
Help me to write 10 mark answer on topic 2. Maternal Mortality in India Status, causes, prevention, national program provisions. from book k park mbbs 3 rd year Arrange the answer properly Highlight words or sentence Add flow chart where needed neededgive the answer And answer should me impressive to the examiner who is my hod of community who will cheak my answer sheet as I have to write it in my university exams to score full marks
MATERNAL MORTALITY IN INDIA
DEFINITION
"The death of a woman while pregnant or within 42 days of termination of pregnancy, irrespective of the duration and site of pregnancy, from any cause related to or aggravated by the pregnancy or its management but not from unintentional or incidental causes."
TYPES OF MATERNAL DEATHS
| Type | Definition |
|---|---|
| Direct Obstetric Deaths | Due to obstetric complications - haemorrhage, eclampsia, sepsis |
| Indirect Obstetric Deaths | Pre-existing disease aggravated by pregnancy - cardiac, renal, anaemia |
| Late Maternal Deaths | Death after 42 days but within 1 year of termination |
1. STATUS OF MATERNAL MORTALITY IN INDIA
"Despite significant improvements, an estimated 44,000 mothers die every year in India" due to pregnancy, childbirth, and post-partum causes.
National MMR Trend:
State-wise MMR (SRS 2016-2018):
| State/Category | MMR |
|---|---|
| India (National Average) | 113 |
| Assam | 215 (Highest) |
| Uttar Pradesh | 197 |
| Madhya Pradesh | 173 |
| Rajasthan | 164 |
| EAG + Assam (combined) | 161 |
| Kerala | 43 (Lowest) |
| Andhra Pradesh | 65 |
- Lifetime risk of maternal death = 0.3% nationally; 0.5% in EAG + Assam states
- States of Kerala, Maharashtra, Andhra Pradesh, Gujarat, Tamil Nadu have already achieved MMR < 100
- SDG 2030 Target: Reduce MMR to < 70 per 1,00,000 live births
2. CAUSES OF MATERNAL MORTALITY
Diagram of Global Causes (Park's Fig. 10):
"About 80% of maternal deaths are due to DIRECT causes and 20% are due to INDIRECT causes"
A. DIRECT (OBSTETRIC) CAUSES
| Cause | % |
|---|---|
| Haemorrhage (Severe Bleeding) | 25% - Single most common cause |
| Infection / Puerperal Sepsis | 15% |
| Eclampsia / Hypertensive Disorders | 13% |
| Unsafe Abortion | 13% |
| Obstructed Labour | 8% |
| Other Direct Causes | 8% |
B. INDIRECT CAUSES (20%)
- Anaemia - most significant indirect cause; affects ~50% of pregnant women
- Cardiac and renal disease
- Hepatitis, Tuberculosis, Malaria, HIV/AIDS
- Metabolic and endocrine disorders
C. DETERMINANTS OF MATERNAL MORTALITY IN INDIA (Table 16, Park's)
┌─────────────────────────────────────────────────────────────────┐
│ DETERMINANTS OF MATERNAL MORTALITY IN INDIA │
├───────────────────────────┬─────────────────────────────────────┤
│ MEDICAL CAUSES │ SOCIAL FACTORS │
├───────────────────────────┼─────────────────────────────────────┤
│ OBSTETRIC: │ • Age at childbirth (< 20 / > 30) │
│ • Toxaemia of pregnancy │ • High parity │
│ • Haemorrhage │ • Too close pregnancies │
│ • Infection │ • Malnutrition and poverty │
│ • Obstructed labour │ • Illiteracy │
│ • Unsafe abortion │ • Ignorance and prejudices │
│ │ • Delivery by untrained dais │
│ NON-OBSTETRIC: │ • Poor transport and communication │
│ • Anaemia │ • Lack of maternity services │
│ • Cardiac, renal disease │ • Low level of women's empowerment │
│ • Malaria, TB, hepatitis │ • Traditional preference for home │
│ • Malignancy, accidents │ deliveries │
└───────────────────────────┴─────────────────────────────────────┘
3. PREVENTION OF MATERNAL MORTALITY
"High maternal mortality reflects not only inadequacy of health care services, but also a low standard of living and socio-economic status of the community."
- Early registration of pregnancy
- At least 4 antenatal check-ups (ANC)
- Dietary supplementation - including correction of anaemia
- Prevention of infection and haemorrhage during puerperium
- Prevention of complications - eclampsia, malpresentations, ruptured uterus
- Treatment of medical conditions - hypertension, diabetes, tuberculosis
- Anti-malarial prophylaxis and Tetanus Toxoid (TT) immunization
- Clean delivery practices (aseptic technique)
- Training and deployment of ASHA and village-level health workers
- Institutional deliveries for high-risk women (bad obstetric history)
- Family planning - limit to 2 children; adequate birth spacing
- Identification and audit of every maternal death - searching for its cause
- Safe abortion services under MTP Act, 1971
4. NATIONAL PROGRAMME PROVISIONS
FLOWCHART: National Programmes to Reduce MMR
NATIONAL PROGRAMMES TO REDUCE MATERNAL MORTALITY
│
┌───────────┬───────────┬───┴───────┬──────────┬──────────┐
│ │ │ │ │ │
JSY JSSK PMSMA SUMAN LaQshya RMNCH+A
(2005) (2011) (2016) (2019) (2017)
│ │ │ │ │
Cash assist Free delivery Free ANC Zero Quality
for inst. + free diet on 9th of denial labour
delivery + free every policy room &
to BPL transport month OT care
women
1. JANANI SURAKSHA YOJANA (JSY) - (Launched: 12 April 2005)
- 100% Centrally Sponsored Scheme under NRHM
- Objective: Reduce MMR and neonatal mortality by promoting institutional deliveries
- ASHA works as a link worker escorting BPL pregnant women to health institutions
- Covers BPL women in both rural and urban areas
| Category | Rural (Mother + ASHA) | Urban (Mother + ASHA) |
|---|---|---|
| LPS (Low Performing States) | Rs.1400 + Rs.600 = Rs.2000 | Rs.1000 + Rs.400 = Rs.1400 |
| HPS (High Performing States) | Rs.700 + Rs.600 = Rs.1300 | Rs.600 + Rs.400 = Rs.1000 |
2. JANANI-SHISHU SURAKSHA KARYAKRAM (JSSK) - (Launched: 1 June 2011)
- Free delivery including Caesarean section (no out-of-pocket expense)
- Free drugs and consumables
- Free diet - up to 3 days (normal delivery), up to 7 days (C-section)
- Free diagnostics and free blood transfusion
- Free transport - home → institution → referral facility → drop-back home
- Similar entitlements for sick newborns up to 30 days after birth
- Benefits an estimated 12 million pregnant women per year
3. PRADHAN MANTRI SURAKSHIT MATRITVA ABHIYAN (PMSMA) - (Launched: June 2016)
- Fixed-day, free-of-cost, quality ANC to all pregnant women
- Services provided on the 9th of every month at government facilities
- Minimum ANC package - investigations + drugs
- Private sector doctors participate as volunteers
- 2.20 crore ANC check-ups conducted; 11.66 lakh high-risk pregnancies identified
4. SUMAN (Surakshit Matritva Aashwasan) - (Launched: 10 October 2019)
- Assured, dignified, respectful quality healthcare at ZERO cost
- Zero tolerance for denial of services to women and newborns
- Target: "Zero preventable maternal and newborn deaths"
5. LaQshya PROGRAMME - (Launched: 2017)
- Improves quality of care in Labour Rooms and Maternity OTs
- Implemented at District Hospitals, CHCs, FRUs and Medical Colleges
- 2,445 public health facilities identified; evidence-based approach
- Ensures Respectful Maternity Care during the most vulnerable period
6. OTHER KEY STRATEGIES
| Programme | Purpose |
|---|---|
| RMNCH+A | Reproductive, Maternal, Neonatal, Child and Adolescent Health Strategy |
| Maternal Death Review (MDR) | Facility + community-based audit to improve obstetric care quality |
| Mother and Child Tracking System (MCTS) | Ensures no pregnant woman is lost to follow-up |
| Village Health & Nutrition Day (VHND) | Monthly ANC, immunization, FP services at anganwadi |
| First Referral Units (FRUs) | Emergency obstetric care at community level |
| Anaemia Mukt Bharat Programme | Addresses anaemia in pregnant women |
| Safe Abortion Services (MTP Act 1971) | Manual Vacuum Aspiration (MVA) at PHC level |
SUMMARY / CONCLUSION
APPROACH TO REDUCE MATERNAL MORTALITY IN INDIA
│
┌──────────────┴──────────────┐
│ │
MEDICAL INTERVENTIONS SOCIO-ECONOMIC MEASURES
│ │
• ANC (≥4 visits) • Female literacy
• Institutional delivery • Women's empowerment
• Skilled birth attendants • Poverty alleviation
• Emergency obstetric care • Nutrition improvement
• National programmes • Community awareness
(JSY, JSSK, PMSMA, SUMAN, • Attack on social and
LaQshya, RMNCH+A) cultural factors
"Any attempt to lower MMR must address both medical causes AND social determinants through active community involvement and socio-economic development." (Park's Textbook of Preventive and Social Medicine, pp. 650-655)
- Underline/highlight all bold terms (MMR values, programme names, dates, percentages)
- Draw the pie chart of causes with percentages in your answer sheet - it immediately impresses the examiner
- Draw the flowchart of national programmes neatly with boxes and arrows
- Write the WHO definition exactly as given above - word-for-word accuracy scores marks
- The state-wise MMR table shows depth of knowledge - include it
- End with the summary flowchart - examiners love structured conclusions
Poshan Abhiyan (143) Government of India has launched "Poshan Abhiyan" on 18th December 2017 for a period of three years commencing from 2012 18, in all 36 states/UTs. The goals are to achieve improvement in nutritional status of children from 0-6 vears. adolestent girls, pregnant women and lactating mothers with fixed targets. It ensures convergence of various programmes i,e anganwadi services, Pradhan Mantri Matru Vandana Yojana; schemes for adolescent girls of Ministry of Women and Child Development; Janani Suraksha Yojana; National Health Mission of Ministry of Health and Family Welfare; Swachh Bharat Mission of Ministry of Jal Shakti etc. The objectives and targets are as follows (140): Prevent and reduce stunting in children (0-6 vears) Prevent and reduce under nutrition and underweight prevalence in children (0-6 years) 3. Reduce the prevalence of anaemia among children (6-59 months) 4. Reduce the prevalence of anaemia among girls and women in the age group (15-49 years) Reduce low birth weight (LBW) The Abhiyan aims to reduce malnutrition in the country through a life cycle approach. Two more schemes are being implemented at the ICDS level. They are Rajiv Gandhi Scheme for Empowerment of Adolescent Girls SABLA" Dor the age group 11 to 18 yease to improve their nutritional and heal arus and ndira Gandhi Matritva Sahyog Yojana (IGMSY) under which conditional cash transfer will be made to pregnant and lactating mothers in order to improve their nutritional and health status (67). At the end of 2019, about 7,075 ICDS projects and 13.77 lakh Anganwadi Centres/Mini-Anganwadi Centres were functional in the country. About 305.09 lakh children are pre-school education beneficiaries and 836.25 lakh supplementary nutrition beneficiaries are children and pregnant and lactating mothers. Help me to write 5 mark answer on topic POSHAN Abhiyan from above copied paragraph of community medicine from book k park mbbs 3 rd year Arrange the answer properly Highlight words or sentence Add flow chart where needed neededgive the answer from above paragraph only And answer should me impressive to the examiner who is my hod of community who will cheak my answer sheet as I have to write it in my university exams to score full marks
POSHAN ABHIYAN
INTRODUCTION
TARGET BENEFICIARIES
┌─────────────────────────────────────────────┐
│ TARGET BENEFICIARIES │
│ │
│ • Children (0–6 years) │
│ • Adolescent Girls │
│ • Pregnant Women │
│ • Lactating Mothers │
└─────────────────────────────────────────────┘
OBJECTIVES AND TARGETS
| S.No | Objective |
|---|---|
| 1. | Prevent and reduce Stunting in children (0–6 years) |
| 2. | Prevent and reduce Undernutrition and Underweight prevalence in children (0–6 years) |
| 3. | Reduce prevalence of Anaemia among children (6–59 months) |
| 4. | Reduce prevalence of Anaemia among girls and women (15–49 years) |
| 5. | Reduce Low Birth Weight (LBW) |
"The Abhiyan aims to reduce malnutrition in the country through a LIFE CYCLE APPROACH."
CONVERGENCE OF PROGRAMMES
POSHAN ABHIYAN
│
┌────────────────┼────────────────┐
│ │ │
Ministry of W&CD Ministry of HFW Ministry of
│ │ Jal Shakti
│ │ │
• Anganwadi • Janani • Swachh
Services Suraksha Bharat
• PM Matru Yojana (JSY) Mission
Vandana • National
Yojana Health
• Schemes for Mission
Adolescent (NHM)
Girls
OTHER SCHEMES AT ICDS LEVEL
-
SABLA (Rajiv Gandhi Scheme for Empowerment of Adolescent Girls)
- Target group: Age 11–18 years
- Aim: Improve nutritional and health status of adolescent girls
-
IGMSY (Indira Gandhi Matritva Sahyog Yojana)
- Conditional cash transfer to pregnant and lactating mothers
- Aim: Improve nutritional and health status of mothers
PROGRAMME COVERAGE (As of end of 2019)
| Indicator | Number |
|---|---|
| ICDS Projects functional | 7,075 |
| Anganwadi Centres / Mini-AWCs functional | 13.77 lakh |
| Children receiving Pre-school Education | 305.09 lakh |
| Supplementary Nutrition beneficiaries (children + pregnant/lactating mothers) | 836.25 lakh |
CONCLUSION
Poshan Abhiyan is a comprehensive, convergent, life-cycle approach to tackle malnutrition across all vulnerable groups - from the unborn child to the adolescent girl - by integrating multiple ministries, programmes and grassroots-level delivery systems under one umbrella.
- Underline/box the launch date, all programme names, and statistics
- Draw the convergence flowchart neatly - it stands out and shows conceptual clarity
- Write the 5 objectives as a numbered list - clean, easy to read, scores full marks
- The coverage statistics table at the end demonstrates depth - always include it
- Quote the "life cycle approach" phrase exactly - it is a key examiner-expected term