Stroke clinical examination
Reading File
Finding Sources
Finding Sources
Searching PubMed
"stroke" AND "clinical examination" AND "neurological assessment"
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Now I have all the content I need to compile a thorough, well-structured answer on stroke clinical examination.
Stroke: Clinical Examination
Definition and Classification
A stroke (cerebrovascular accident, CVA) is the interruption of blood flow to the brain or brainstem resulting in impaired neurological function lasting more than 24 hours. Neurological impairment resolving within 24 hours is a transient ischemic attack (TIA). Strokes are broadly classified as:
-
Ischemic (~80%): thrombotic or embolic. The most common type is embolic, often from atherosclerotic carotid plaques.
-
Hemorrhagic (~20%): rupture of blood vessels (intracerebral or subarachnoid).
-
Gray's Anatomy for Students, p. 1019; Morgan and Mikhail's Clinical Anesthesiology, p. 896
1. History
The hallmark of acute ischemic stroke is abrupt onset of a focal neurological deficit in the distribution of a specific vascular territory. The history alone often establishes the differential diagnosis:
- A patient with atrial fibrillation who abruptly develops word-finding difficulties with right hemiparesis likely had a cardiogenic embolus to the left MCA.
- Acute onset of diplopia, vertigo, and hemiparesis suggests a brainstem lesion.
Key history points to obtain:
- Time of onset - or last known well time (critical for thrombolysis eligibility)
- Concomitant medical illnesses and risk factors (hypertension, diabetes, atrial fibrillation, smoking, dyslipidemia)
- Medications, anticoagulants, oral contraceptives
- Allergies
- Stroke mimics must be excluded
- A witness may be required if the patient cannot communicate
- Goldman-Cecil Medicine, p. 3936
2. General Physical Examination
| Finding | Clinical Significance |
|---|---|
| Severely elevated BP with basal ganglia/thalamus/pons/cerebellar deficits | Suggests hemorrhagic stroke |
| Reduced BP in one arm with transient vertigo on arm movement | Subclavian steal syndrome |
| Anterior cervical bruit (contralateral to MCA territory deficit) | Symptomatic carotid stenosis |
| Irregularly irregular pulse ± cardiac murmur | Atrial fibrillation → cardioembolic etiology |
| Cholesterol emboli on fundoscopy (Hollenhorst plaque) | Proximal atheroembolism |
| Fundoscopy - retinal emboli (shiny white or reddish) | Carotid artery disease |
| Fundoscopy - diabetic/hypertensive retinopathy | Small-vessel disease risk factors |
- Goldman-Cecil Medicine, p. 3937; Adams and Victor's Principles of Neurology, p. 800
3. Neurological Examination
A full neurological examination is required, covering:
a) Cognition and Language
- Aphasia: present in dominant hemisphere (usually left) MCA infarcts. May be expressive (Broca), receptive (Wernicke), or global.
- Dysarthria: slurred speech without aphasia; can occur in any territory.
- Spatial neglect: non-dominant hemisphere strokes.
- Apraxia / Agnosia: cortical signs, absent in lacunar infarcts.
b) Cranial Nerves
- Visual fields: homonymous hemianopia (MCA/PCA territory); monocular visual loss (amaurosis fugax = ophthalmic artery TIA).
- Eye movements: horizontal gaze palsy; "eyes deviate toward the lesion" in frontal cortex strokes, "away from the lesion" in pontine strokes.
- Facial palsy: upper motor neuron pattern (sparing forehead) in cortical strokes.
- Diplopia, nystagmus, vertigo: posterior circulation/brainstem.
c) Motor System
- Hemiparesis / Hemiplegia: contralateral to the lesion.
- MCA territory: arm > leg (arm and face primarily affected).
- ACA territory: leg > arm.
- Tone: initially flaccid acutely; progresses to spasticity.
- Reflexes: brisk deep tendon reflexes + extensor plantar response (Babinski) contralaterally.
- Pronator drift: sensitive screen for subtle upper limb weakness.
d) Sensory System
- Hemisensory loss: contralateral loss of pain, temperature, proprioception, vibration.
- Thalamic infarcts produce dense contralateral hemianesthesia.
- Spinothalamic (pain/temperature) vs. dorsal column (proprioception/vibration) dissociation helps localize.
e) Coordination and Gait
- Limb ataxia: present in posterior circulation strokes (cerebellar/PICA/AICA territory).
- Finger-nose-finger and heel-shin tests.
- Ataxic hemiparesis: a classic lacunar syndrome.
f) Reflexes
- Babinski sign (extensor plantar): indicates upper motor neuron lesion.
- Hoffman sign in upper limbs.
4. Vascular Territory Localization
| Territory | Classic Signs |
|---|---|
| MCA (dominant) | Contralateral hemiparesis (arm > leg), hemisensory loss, homonymous hemianopia, aphasia |
| MCA (non-dominant) | Contralateral hemiparesis, hemisensory loss, hemianopia, spatial neglect, anosognosia |
| ACA | Contralateral leg > arm weakness, frontal lobe signs (abulia, incontinence) |
| PCA | Contralateral homonymous hemianopia, memory loss; no hemiparesis (cortex spared) |
| Brainstem (basilar) | Cranial nerve palsies ipsilateral + long tract signs contralateral ("crossed signs"), diplopia, dysarthria, dysphagia, ataxia |
| PICA (Wallenberg's) | Ipsilateral facial anesthesia + Horner's, contralateral pain/temperature loss, ipsilateral ataxia, hiccups, dysphagia |
| Lacunar | Pure motor stroke, pure sensory stroke, ataxic hemiparesis, clumsy hand-dysarthria; cortical signs ABSENT |
- Goldman-Cecil Medicine, p. 3936; Morgan and Mikhail's Clinical Anesthesiology, p. 896
5. Standardized Neurological Scales
NIH Stroke Scale (NIHSS) - Range 0 to 42
The most widely used tool for measuring stroke severity. A score can be obtained in under 10 minutes (training required for reliability). The scale emphasizes motor deficits and has lower sensitivity for posterior circulation and non-dominant hemisphere deficits.
| NIHSS Item | Score Range |
|---|---|
| 1A. Level of consciousness | 0-3 |
| 1B. Response to month/age (orientation) | 0-3 |
| 1C. Blink eyes/squeeze hand (commands) | 0-2 |
| 2. Horizontal eye movements | 0-2 |
| 3. Visual fields | 0-3 |
| 4. Facial palsy | 0-3 |
| 5A/5B. Arm drift (left/right) | 0-4 each |
| 6A/6B. Leg drift (left/right) | 0-4 each |
| 7. Limb ataxia | 0-2 |
| 8. Sensation | 0-2 |
| 9. Aphasia | 0-3 |
| 10. Dysarthria | 0-2 |
| 11. Extinction/inattention | 0-2 |
Severity thresholds:
- <5: Mild
- 5-14: Mild-to-moderate
- 15-24: Severe
- >25: Very severe
Modified Rankin Scale (mRS) - Range 0 to 6
Measures functional outcome/disability post-stroke (0 = no symptoms; 6 = death).
ABCD² Score (for TIA risk stratification) - Range 0 to 8
-
Age >60: 1 point
-
BP >140/90: 1 point
-
Unilateral weakness: 2 points; Dysarthria without weakness: 1 point
-
TIA duration 10-59 min: 1 point; >60 min: 2 points
-
Diabetes: 1 point
-
Score 0-3 = low risk; higher scores = increasing 2-day and 90-day stroke risk
-
Adams and Victor's Principles of Neurology, pp. 800-801
6. Investigations (Immediate)
All patients:
- Non-contrast CT brain (within 20 min of arrival) - to exclude hemorrhage; MRI/DWI for acute ischemia
- Blood glucose (hypoglycemia is a stroke mimic)
- Oxygen saturation
- CBC + platelet count
- PT/INR, aPTT
- Serum electrolytes, renal function
- Troponin
- ECG (atrial fibrillation, ischemia)
Selected patients:
- CT/MR angiography (suspected large vessel occlusion)
- CT/MR perfusion (penumbra assessment)
- Carotid Doppler ultrasound
- Echocardiogram
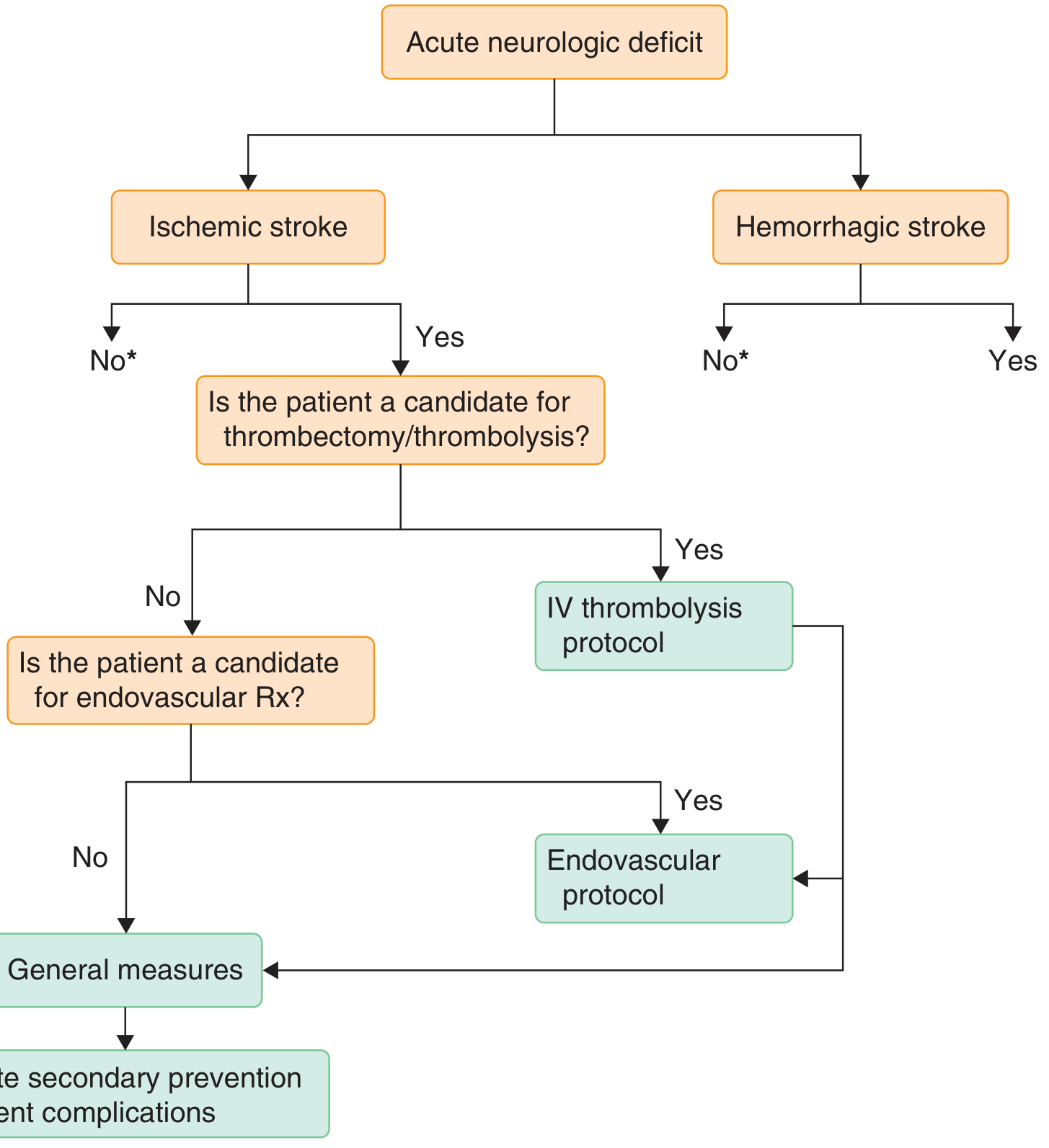
The diagnostic flowchart for acute neurologic deficit:
- Goldman-Cecil Medicine, pp. 3937-3938; Gray's Anatomy for Students, p. 1019
7. Key Points for Clinical Examination
- Time is brain - document symptom onset time immediately; thrombolysis window is 3-4.5 hours.
- The neurological examination both documents deficits and localizes the vascular territory affected.
- Cortical signs (aphasia, agnosia, apraxia, hemianopia) distinguish cortical from lacunar infarcts.
- "Crossed signs" (ipsilateral cranial nerve + contralateral long tract) = brainstem lesion.
- NIHSS is a surrogate for - not a replacement of - a careful bedside neurological examination.
- Posterior circulation strokes are misdiagnosed in >34% of cases (most often as vestibular neuritis); always consider stroke in acute vertigo with any additional neurological signs.
- Symptom to Diagnosis, 4th Edition, p. 3050; Adams and Victor's Principles of Neurology, p. 801
History taking
Asking for Preferences
This is a shared conversation. Sign in to Orris to start your own chat.