Define choledocholithiasis
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive content to deliver a thorough answer. Here is the full definition and overview:
Choledocholithiasis
Choledocholithiasis is the presence of stones within the common bile duct (CBD). It occurs in approximately 5-20% of patients with symptomatic gallstones (cholelithiasis).
Classification
There are two main types, based on how the stones arise:
| Type | Description | Stone Type | Population |
|---|---|---|---|
| Primary | De novo stone formation within the CBD itself | Brown pigment stones (precipitated bile pigments + cholesterol) | More common in Asian populations; associated with bacterial infection |
| Secondary | Stones formed in the gallbladder that migrate into the CBD | Cholesterol or black pigment stones | More common in the United States |
A subset called retained stones refers to secondary stones identified in the CBD within 2 years after cholecystectomy; these occur in 1-2% of post-cholecystectomy patients.
- Sabiston Textbook of Surgery, p. 1832
Clinical Presentation
Choledocholithiasis may be asymptomatic (incidental finding) or may present with a spectrum of manifestations:
- Biliary colic - right upper quadrant (RUQ) or epigastric pain
- Obstructive jaundice - scleral icterus, dark urine, pale/acholic stools; onset is typically painful (distinguishing it from malignant obstruction, which is painless)
- Ascending cholangitis (Charcot's triad: fever, jaundice, RUQ pain) - due to ascending bacterial infection from the duodenum; bacteremia is present in ~74% of cases
- Gallstone pancreatitis - if the stone obstructs the pancreatic duct at the ampulla of Vater
Complications are frequently the presenting manifestation.
- Symptom to Diagnosis: An Evidence Based Guide, p. 50
Diagnosis
Laboratory Findings
No lab test is pathognomonic. Key findings include:
- Elevated total bilirubin - low sensitivity, high specificity for choledocholithiasis; >4 mg/dL is a very strong predictor
- Elevated AST, ALT, ALP - early in the disease, transaminases rise first; later, an obstructive pattern (elevated ALP, bilirubin) dominates
- Leukocytosis - raises concern for cholangitis
- Lipase >3x upper limit of normal - diagnostic for concomitant pancreatitis
- When elevated bilirubin is combined with an abnormal ultrasound, pre-test probability for choledocholithiasis approaches 90%; a patient with normal LFTs and normal ultrasound has <5% probability
Imaging
| Modality | Notes |
|---|---|
| Transabdominal ultrasound | Sensitivity ~80%, specificity ~90% for CBD stones; CBD dilation >5-6 mm is suggestive; only ~25% of cases show a dilated CBD |
| CT scan | Only ~75% sensitive - not the test of choice |
| MRCP | Highly accurate, non-invasive; preferred for intermediate-risk patients |
| EUS (Endoscopic Ultrasound) | Highly sensitive and specific; preferred for low-to-intermediate risk patients to avoid unnecessary ERCP |
| ERCP | Gold standard - both diagnostic and therapeutic; proceed directly in high-risk patients |
- Sabiston Textbook of Surgery, p. 1832
ASGE Risk Stratification (Predictors of Choledocholithiasis)
| Predictor Strength | Criteria |
|---|---|
| Very strong | CBD stone on transabdominal US; ascending cholangitis; bilirubin >4 mg/dL |
| Strong | Dilated CBD (>6 mm) on US; bilirubin 1.8-4 mg/dL |
| Moderate | Abnormal liver biochemical tests (other than bilirubin); age >55; clinical gallstone pancreatitis |
-
Any very strong predictor = high likelihood
-
Both strong predictors present = high likelihood
-
No predictors = low likelihood
-
All other patients = intermediate likelihood
-
Mulholland and Greenfield's Surgery, p. 3073-3074
Intraoperative Cholangiogram
Below is an intraoperative cholangiogram demonstrating choledocholithiasis - note the filling defect (stone, indicated by arrow) in the CBD with no filling of the duodenum:
Intraoperative cholangiogram showing choledocholithiasis in an asymptomatic patient (arrow). - Sabiston Textbook of Surgery, p. 1832
Management
Management depends on the clinical context (jaundice, cholangitis, pancreatitis, or incidental finding), gallbladder status, and available expertise. The main options are:
1. Endoscopic Approach (First-line in most cases)
- ERCP with endoscopic sphincterotomy and stone extraction - the primary therapy; success rate ~84-89% for complete duct clearance in a single session
- Recommended in high-risk patients and for acutely ill patients with cholangitis requiring biliary decompression
- Recommended for stones identified before cholecystectomy: clear duct endoscopically, then proceed with laparoscopic cholecystectomy
2. Surgical Approach
- Laparoscopic bile duct exploration (transcystic or transcholedochal approach) - stone clearance rates average 95%, operative mortality ~0.5%
- Preferred when choledocholithiasis is discovered intraoperatively and surgeon expertise allows it
- Open bile duct exploration - reserved for large impacted stones, multiple failed endoscopic attempts, or anatomy precluding endoscopy (e.g., prior Roux-en-Y gastric bypass)
3. Percutaneous Approach
- Used when endoscopic and surgical options are not feasible
Summary of Timing Decisions
| Scenario | Preferred Approach |
|---|---|
| High risk + cholangitis | ERCP first, then cholecystectomy |
| Severe gallstone pancreatitis with persistent CBD stones | ERCP first |
| Stone found preoperatively, no cholangitis | ERCP + laparoscopic cholecystectomy OR single-stage laparoscopic cholecystectomy + CBD exploration |
| Stone found during laparoscopic cholecystectomy | Laparoscopic CBD exploration OR complete cholecystectomy + postoperative ERCP |
| Large/impacted stones or failed ERCP | Open CBD exploration |
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease, p. 1267
- Mulholland and Greenfield's Surgery, p. 3074-3075
In summary, choledocholithiasis is the presence of gallstones in the common bile duct, most commonly arising from migration of gallbladder stones (secondary type). It can range from asymptomatic to life-threatening cholangitis. Risk stratification using clinical, laboratory, and imaging findings guides the choice between ERCP, laparoscopic CBD exploration, or open surgery, and the sequencing of these procedures relative to cholecystectomy.
Give me the answer on biliary struc- strictures. Describe the cause and risk factor of the biliary strictures. Explain the pathophysiology of the same and their effect on bile flow and liver function. Describe the clinical manifestation of biliary strictures.
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
Reading File
Loading Image
Reading File
Biliary Strictures
A biliary stricture is an abnormal narrowing of the bile duct lumen - either the intrahepatic or extrahepatic biliary tree - that impairs or obstructs the flow of bile from the liver to the duodenum. Strictures can be benign or malignant in origin.
1. Causes and Risk Factors
Biliary strictures are broadly categorized as benign or malignant.
A. Benign Biliary Strictures
i. Iatrogenic / Postoperative (Most Common)
Operative injury is the leading cause of benign biliary stricture, accounting for the vast majority of cases.
- Cholecystectomy - responsible for >90% of postoperative biliary strictures in the US; laparoscopic cholecystectomy carries a 2-3x higher rate of major bile duct injury (0.4-1.3%) compared to the open technique (0.2-0.3%)
- Choledochotomy (bile duct exploration)
- Gastrectomy
- Hepatic resection
- Liver transplantation - hepatic artery thrombosis post-transplant is a recognised cause of ischemic biliary stricture
The classic laparoscopic injury involves misidentification of the common bile duct (CBD) as the cystic duct, leading to clipping and division of the CBD.
Risk factors for intraoperative bile duct injury:
| Category | Specific Factors |
|---|---|
| Pathologic | Acute cholecystitis, cholangitis, gallstone pancreatitis, severe portal hepatis inflammation |
| Anatomic | Short cystic duct, low cystic duct insertion, long common wall between cystic duct and CBD, aberrant right sectoral duct |
| Technical | Limited laparoscopic field of view, excessive clip placement, injudicious electrocautery, bleeding obscuring anatomy, obesity |
- Maingot's Abdominal Operations, p. 1057-1058
ii. Inflammatory / Chronic
- Choledocholithiasis (CBD stones) - recurrent stone impaction and cholangitis produce fibrosis and stricture formation
- Chronic pancreatitis - fibrosis of the pancreatic head compresses the intrapancreatic portion of the CBD
- Cholangitis (acute/recurrent) - ascending bacterial infection causes ductal wall inflammation and subsequent scarring
- Primary Sclerosing Cholangitis (PSC) - autoimmune disease, more common in males, strongly associated with inflammatory bowel disease (especially ulcerative colitis); causes multifocal fibro-inflammatory stricturing of intra- and extrahepatic bile ducts
- IgG4-related cholangitis - immune-mediated segmental or diffuse narrowing; responds to corticosteroids
- Parasitic infections - liver flukes (Clonorchis sinensis, Opisthorchis viverrini), Ascariasis; mechanical obstruction plus chronic ductal inflammation leads to fibrosis
- AIDS cholangiopathy - opportunistic infections (CMV, Cryptosporidium) in immunocompromised patients
iii. Congenital
- Biliary atresia - fibro-inflammatory obliteration of the bile ducts in neonates
iv. Radiation-induced
- Radiotherapy to the upper abdomen can cause late-onset ductal fibrosis and stricture
v. Traumatic
- Blunt abdominal trauma; penetrating injury to extrahepatic bile ducts
vi. Mirizzi's Syndrome
- External compression of the common hepatic duct by a large stone impacted in the cystic duct or gallbladder neck, causing a functional biliary stricture
B. Malignant Biliary Strictures
-
Cholangiocarcinoma - most common primary malignancy causing biliary stricture; patients with PSC have significantly elevated risk
-
Pancreatic carcinoma - compresses the intrapancreatic CBD; typically presents as painless progressive jaundice
-
Gallbladder carcinoma - causes obstruction by direct invasion or secondary stricture
-
Ampullary carcinoma - obstruction at the ampulla of Vater
-
Metastatic lymphadenopathy - periportal nodes compressing the hilum
-
Frameworks for Internal Medicine, p. 9376-9381; Bailey and Love's Short Practice of Surgery, p. 1275
2. Pathophysiology - Effect on Bile Flow and Liver Function
A. Mechanical Obstruction of Bile Flow
A biliary stricture creates a fixed mechanical barrier to the antegrade flow of bile. The sequence of events is:
- Increased luminal pressure proximal to the stricture - bile continues to be secreted by hepatocytes but cannot drain freely
- Proximal ductal dilation - the bile ducts upstream of the stricture dilate as back-pressure builds
- Biliary stasis - stagnant bile predisposes to stone formation, infection, and colonization by enteric bacteria (ascending cholangitis)
- Cholestasis - impaired bile flow leads to accumulation of bile constituents (bilirubin, bile acids, cholesterol) in the hepatic parenchyma and bloodstream
"Cholestasis occurs with impaired bile flow, leading to accumulation of bile pigment in the hepatic parenchyma. Large bile duct obstruction is most commonly associated with gallstones and carcinomas; ascending cholangitis may develop. Chronic obstruction can lead to secondary sclerosing cholangitis and cirrhosis."
- Robbins, Cotran & Kumar Pathologic Basis of Disease
B. Effects on Liver Function
Prolonged biliary obstruction has a cascade of hepatic consequences:
| Effect | Mechanism |
|---|---|
| Conjugated (direct) hyperbilirubinemia | Conjugated bilirubin accumulates in hepatocytes and is secreted into the circulation; being water-soluble, it is filtered in the urine (bilirubinuria) |
| Elevated Alkaline Phosphatase (ALP) and GGT | Biliary obstruction stimulates increased synthesis and release of ALP from bile duct epithelium; GGT is an early, sensitive marker |
| Mild transaminase elevation | Secondary hepatocellular injury from bile acid toxicity |
| Bile acid retention | Bile acids accumulate in the blood, depositing in skin and causing pruritus |
| Fat malabsorption | Deficient bile delivery to the duodenum impairs emulsification and absorption of dietary fats and fat-soluble vitamins (A, D, E, K) |
| Coagulopathy | Vitamin K malabsorption leads to deficient production of clotting factors II, VII, IX, X; PT/INR prolonged |
| Secondary biliary fibrosis | Persistent cholestasis activates hepatic stellate cells via bile acid-mediated and inflammatory pathways, driving periportal and periductal fibrosis |
| Secondary biliary cirrhosis | Untreated, long-standing obstruction leads to progressive fibrosis, loss of hepatic architecture, and cirrhosis within approximately 5 years |
| Portal hypertension | Cirrhosis-related increased resistance in the portal circulation leads to portal hypertension with its sequelae (varices, ascites, splenomegaly) |
| Liver failure | End-stage consequence of unrelieved obstruction |
"Inflammation of the biliary tree results in fibrosis and stricture formation. Due to stricture formation, biliary stasis occurs, which predisposes patients to infection and hepatic abscess formation. Long-term complications include cirrhosis and liver failure."
- Yamada's Textbook of Gastroenterology
"Bile duct strictures that go unrecognized or are improperly managed can lead to severe complications such as recurrent cholangitis, secondary biliary cirrhosis, and portal hypertension."
- Schwartz's Principles of Surgery, p. 1446
C. Inflammatory Pathways (PSC)
In PSC and inflammatory strictures, the mechanism is distinct: periductal inflammation and fibrosis develop concentrically around the bile ducts ("onion-skin" pattern on histology), progressively obliterating the ductal lumen. This leads to the same downstream consequences of cholestasis but also to multisegmental stricturing and beading of the biliary tree.
3. Classification of Biliary Strictures (Bismuth Classification)
Biliary strictures are classified by anatomical level, which guides surgical planning:
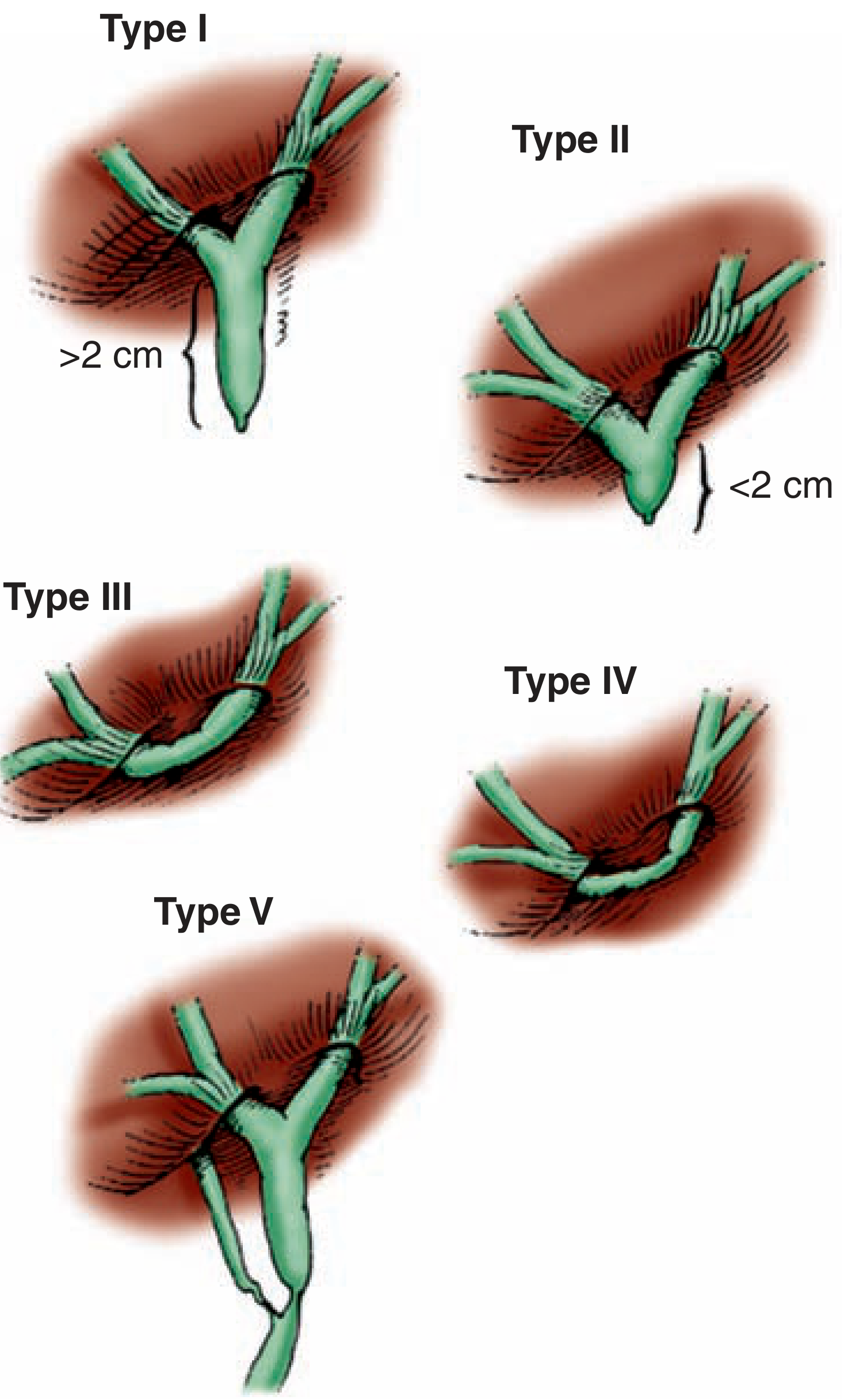
Bismuth classification of bile duct strictures based on level in relation to the confluence of hepatic ducts. Types III-V are considered complex. - Maingot's Abdominal Operations
| Bismuth Type | Location |
|---|---|
| I | Stricture >2 cm below the hepatic confluence |
| II | Stricture <2 cm below the hepatic confluence |
| III | Stricture at the hepatic confluence; hepatic ducts remain in continuity |
| IV | Stricture involving right and left hepatic ducts; ducts not in continuity |
| V | Stricture involving a right sectoral duct |
The Strasberg classification expands this to include types A-E, with E subtypes corresponding to Bismuth types I-V.
4. Clinical Manifestations
A. Early / Acute Presentation (Bile Duct Injury / Leak)
When a bile duct injury is unrecognized at surgery and results in a bile leak:
- Abdominal pain and distension - typically within the first week post-operatively
- Nausea and vomiting
- Fever and signs of sepsis - tachycardia, hypotension in severe cases
- Bilious drainage from incision sites or operative drains
- Biloma - loculated bile collection, presenting as a low-grade fever and localized pain
- Chemical peritonitis or frank biliary peritonitis if bile drains freely into the peritoneum
- Biliary ascites in severe leaks
B. Subacute and Chronic Presentation (Established Stricture)
Bile duct strictures may present months to years after the inciting event:
| Symptom/Sign | Description |
|---|---|
| Jaundice | Yellow discoloration of skin, sclera, and mucous membranes; detectable when serum bilirubin >2.5-3 mg/dL; may be the sole presenting feature |
| Pruritus | Intense itching due to bile acid deposition in skin; often preceding or accompanying jaundice; patients may have multiple excoriations on examination |
| Right upper quadrant (RUQ) pain | Dull aching or biliary colic-type pain from ductal distension |
| Dark urine (bilirubinuria) | Water-soluble conjugated bilirubin filtered by kidneys |
| Pale/acholic stools | Absence of bile pigment (urobilinogen) from stool |
| Cholangitis (Charcot's Triad) | Fever + jaundice + RUQ pain; the most common presentation of benign biliary strictures; may progress to sepsis with hypotension and altered consciousness (Reynolds' Pentad) |
| Steatorrhoea | Fatty, malodorous stools from fat malabsorption due to deficient intraluminal bile |
| Weight loss | Malabsorption and anorexia |
| Hepatomegaly | Palpable enlarged liver due to intrahepatic bile duct dilation or underlying hepatocellular damage |
| Splenomegaly | Suggests portal hypertension from secondary biliary cirrhosis |
| Unexplained fever / malaise | Particularly in isolated right sectoral duct injuries; episodes of mild cholangitis |
"Bile duct strictures most commonly result in recurrent episodes of cholangitis but may present with isolated jaundice without infection. Liver function tests usually show evidence of cholestasis with elevations of bilirubin and alkaline phosphatase."
- Schwartz's Principles of Surgery, p. 1446
"Patients with a slowly evolving stricture may have nonspecific abdominal complaints, jaundice, pruritus, cholangitis, or derangements in liver function tests... patients can present with painless jaundice, which can be confused with a malignant stricture."
- Maingot's Abdominal Operations, p. 1061
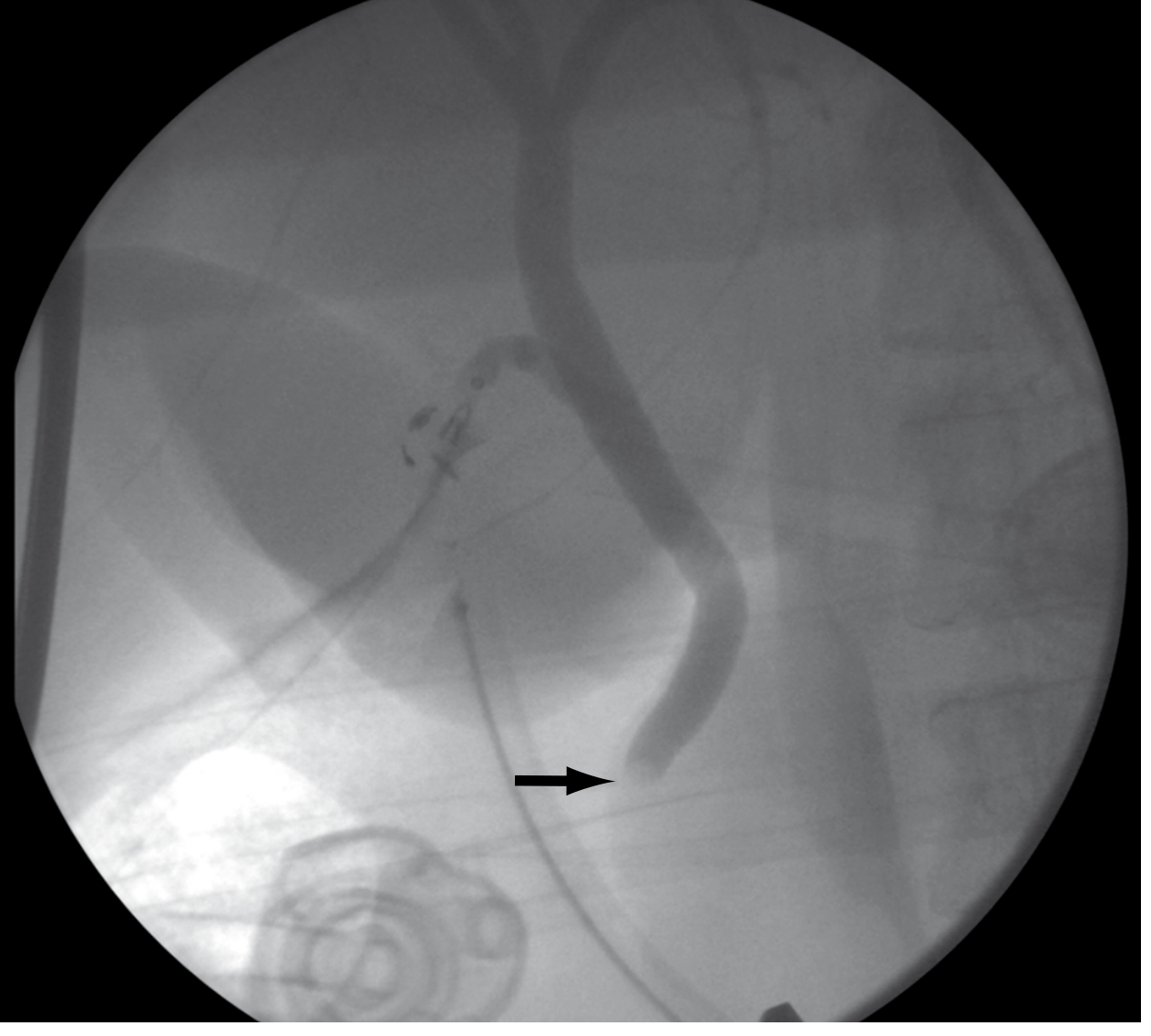
ERCP Imaging of Biliary Strictures
Below: ERCP showing a stricture of the common hepatic duct (arrow) in a patient following laparoscopic cholecystectomy. Clips from the operation are visible projected over the CBD.
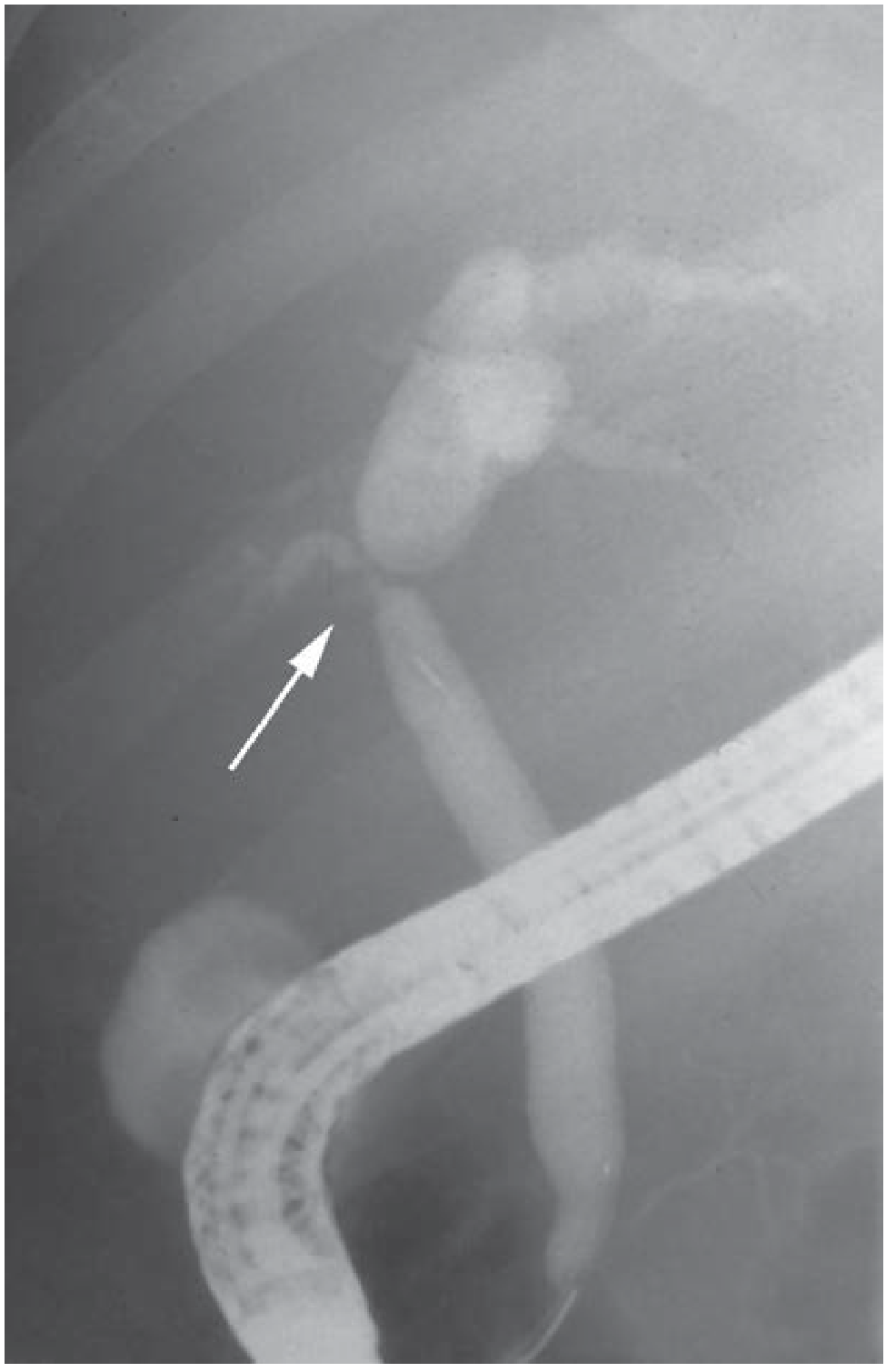
ERCP showing stricture of the common hepatic duct (arrow) - Schwartz's Principles of Surgery
PSC: Stricturing and Beading Pattern on ERCP
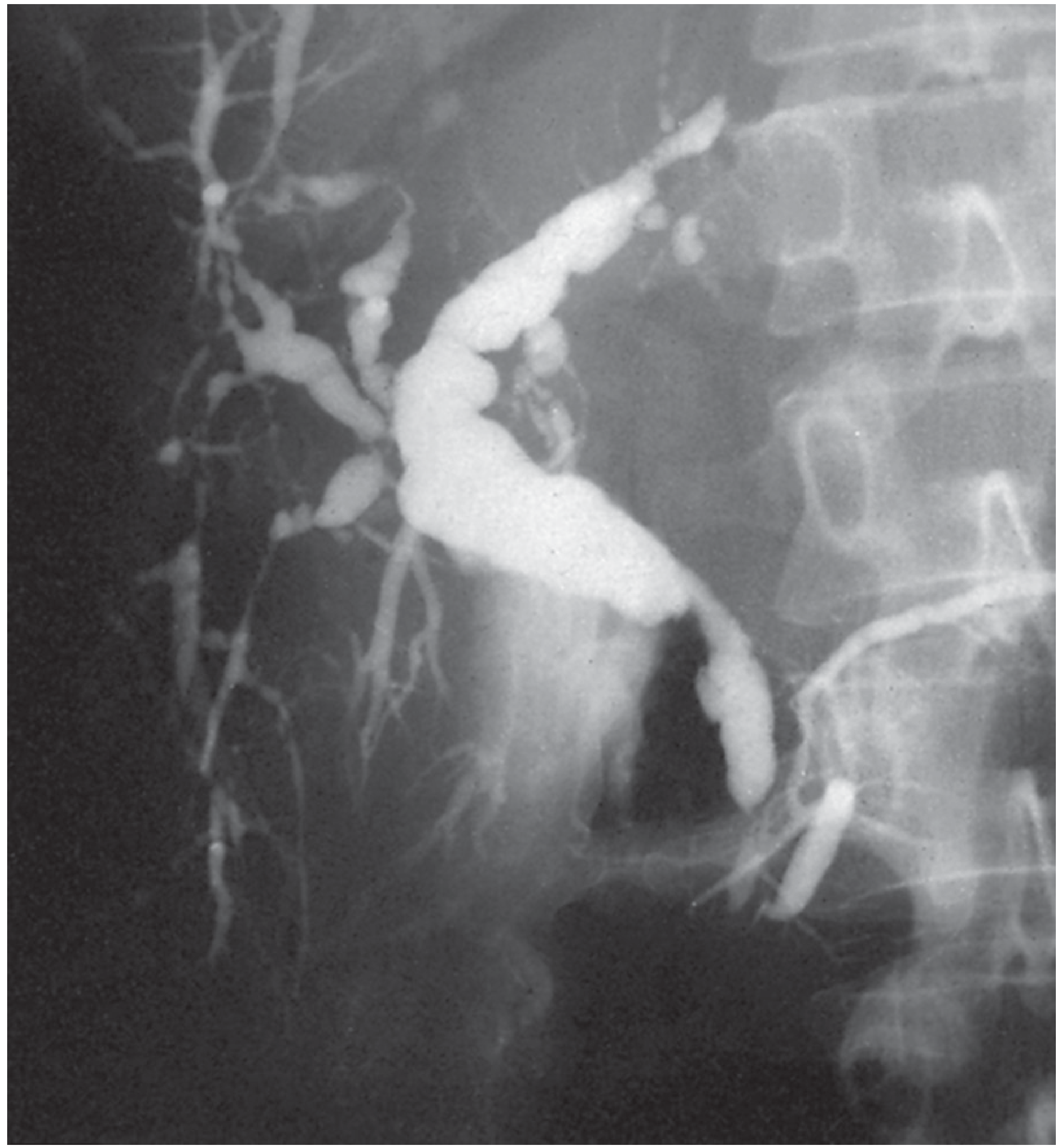
ERCP demonstrating the characteristic stricturing and beading pattern of PSC in a patient with ulcerative colitis - Bailey & Love's Short Practice of Surgery, p. 1276
5. Laboratory Findings Summary
| Test | Expected Finding | Significance |
|---|---|---|
| Serum bilirubin (conjugated) | Elevated | Cholestasis from obstruction |
| Alkaline phosphatase (ALP) | Markedly elevated | Biliary epithelial synthesis/release |
| GGT | Elevated | Sensitive early marker of hepatobiliary obstruction |
| AST / ALT | Mildly elevated | Secondary hepatocellular injury |
| Prothrombin time (PT/INR) | Prolonged | Vitamin K malabsorption |
| WBC | Elevated (leukocytosis) | Suggests superimposed cholangitis |
| IgG4 levels | May be elevated | Suggests IgG4-related cholangiopathy |
| Lipase | Elevated >3x ULN | Concomitant pancreatitis |
In summary, biliary strictures arise most commonly from surgical injury (especially laparoscopic cholecystectomy), but also from inflammatory, autoimmune, parasitic, malignant, and congenital processes. The core pathophysiology is mechanical obstruction of bile flow, producing upstream ductal hypertension and biliary stasis, which triggers cholestasis, hepatocellular injury, fibrosis, and eventually secondary biliary cirrhosis if untreated. Clinically, they manifest as recurrent cholangitis, obstructive jaundice with its systemic consequences (pruritus, steatorrhoea, coagulopathy), and ultimately liver failure - with the clinical picture varying depending on whether the presentation is acute (bile leak) or chronic (established stricture).
This is a shared conversation. Sign in to Orris to start your own chat.