Antenatal care of Gynecology and obstetrics
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Now I have comprehensive material. Let me compile the full answer.
Antenatal Care (ANC) - Gynecology & Obstetrics
Source: Park's Textbook of Preventive and Social Medicine
Definition
Antenatal care (ANC) is defined as care provided by skilled health-care professionals to pregnant women and pregnant adolescent girls in order to ensure the best health conditions for both mother and baby during pregnancy. It includes risk identification, prevention and management of pregnancy-related or concurrent diseases, and health education and promotion.
ANC reduces maternal and perinatal morbidity and mortality both directly (through detection) and indirectly (by identifying women at increased risk of complications during labour and delivery, ensuring referral to appropriate care).
Objectives of ANC
- Promote, protect, and maintain the health of the mother during pregnancy
- Detect "high-risk" cases and give them special attention
- Foresee complications and prevent them
- Remove anxiety and dread associated with delivery
- Reduce maternal and infant mortality and morbidity
- Teach the mother elements of child care, nutrition, personal hygiene, and environmental sanitation
- Sensitize the mother to the need for family planning
- Attend to the under-fives accompanying the mother
Antenatal Visits
Ideally: once a month during the first 7 months, twice a month in the 8th month, weekly thereafter if normal.
Minimum recommended schedule (4 visits):
| Visit | Timing |
|---|---|
| 1st visit | Within 12 weeks - register pregnancy and first check-up |
| 2nd visit | 14-26 weeks |
| 3rd visit | 28-34 weeks (advisable to see a medical officer at PHC) |
| 4th visit | 36 weeks to term |
Components of Every ANC Check-up
I. History Taking (First Visit)
- Confirm the pregnancy
- Identify complications from previous pregnancy/confinement
- Record date of 1st day of Last Menstrual Period (LMP) and calculate Expected Date of Delivery (EDD) - add 9 months and 7 days to the 1st day of LMP
- Record danger symptoms: fever, persistent vomiting, abnormal vaginal discharge or bleeding, breathlessness, generalized swelling, severe headache, blurred vision, burning micturition, decreased fetal movements
- Past medical history: hypertension, diabetes, heart disease, TB, renal disease, epilepsy, asthma, jaundice, malaria, RTI, STD, HIV/AIDS
- Family history: hypertension, diabetes, TB, thalassaemia, twins, congenital malformations
- Drug allergies and habit-forming drugs
II. Physical Examination
General examination:
- Weight measurement (at every visit)
- Blood pressure monitoring
- Respiratory rate
- Check for pallor (anaemia) and oedema
- Thyroid examination
- Breast examination - check for inverted or flat nipples
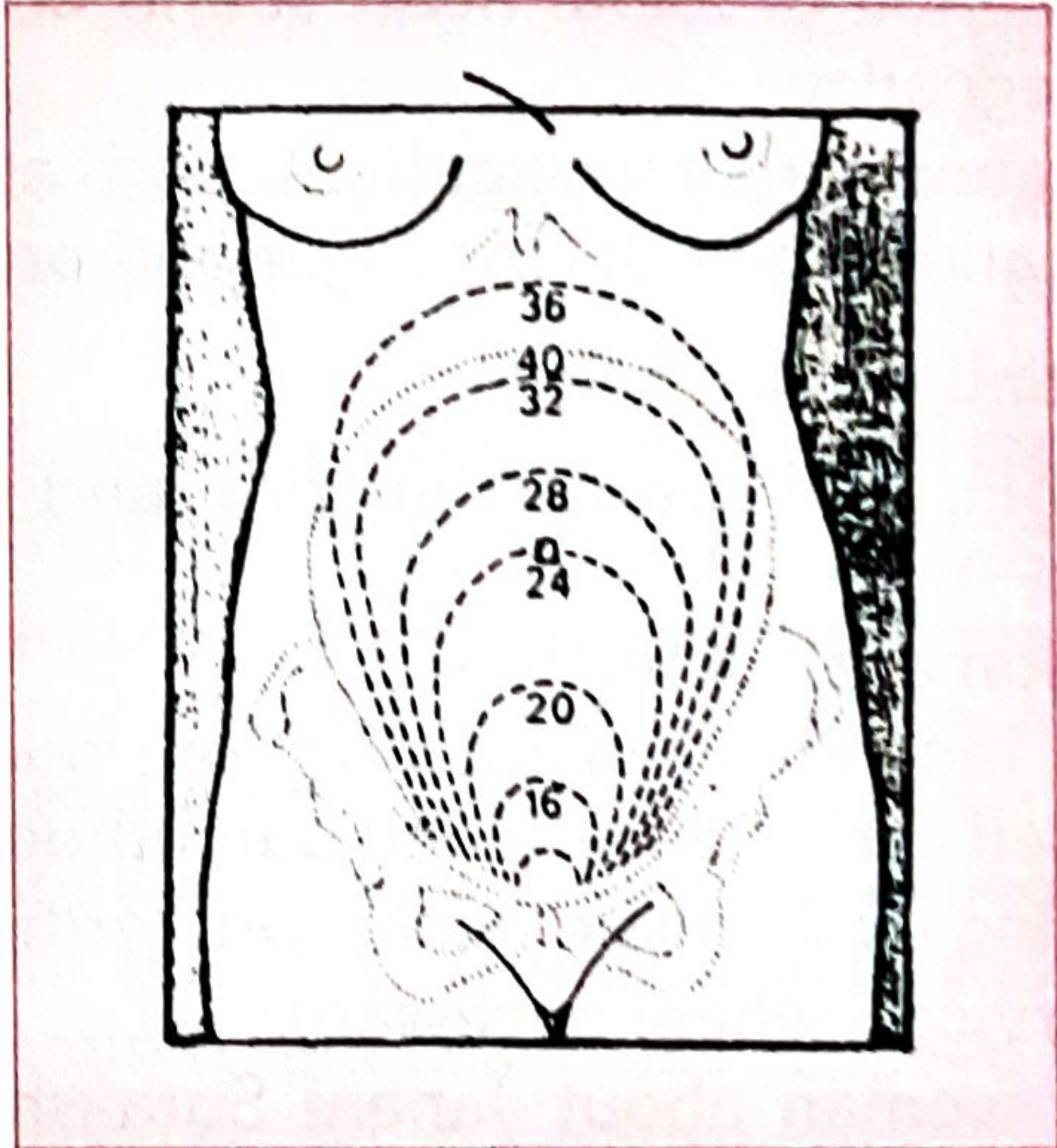
III. Abdominal Examination
The uterine fundal height is assessed at each visit to monitor fetal growth:
| Gestational Age | Fundal Height |
|---|---|
| 12 weeks | Just palpable per abdomen |
| 16 weeks | Between symphysis and umbilicus |
| 20 weeks | Flat at lower border of umbilicus |
| 24 weeks | At the level of umbilicus |
| 28 weeks | 4 fingers above umbilicus |
| 32 weeks | Midway between umbilicus and xiphisternum |
| 36 weeks | At the level of xiphisternum |
| 40 weeks | Slightly lower (fetal head descends) |
Uterine Fundal Height at Various Stages of Pregnancy (numbers indicate weeks):
Other abdominal findings:
- Fetal heart sounds - heard after 6th month; normal rate 120-140/min
- Fetal movements - felt by examiner after 18-22 weeks
- Fetal parts - distinguishable (head, back, limbs) after 28 weeks
- Fetal lie and presentation - relevant after 32 weeks
- Suspect multiple pregnancy if uterus larger than expected gestational age
IV. Assessment of Gestational Age
- Most accurate method: early ultrasound (before 20 weeks)
- LMP-based calculation using Naegele's rule
- Clinical assessment using fundal height
V. Laboratory Investigations
At Sub-centre:
- Pregnancy detection test
- Haemoglobin estimation
- Urine test for albumin and sugar
- Rapid malaria test
At PHC/CHC/FRU:
- Blood group including Rh factor
- VDRL/RPR (syphilis)
- HIV testing
- Blood sugar testing
- HBsAg (Hepatitis B)
- TB skin test (where available)
Preventive Interventions
1. Iron and Folic Acid (IFA) Supplementation
- Given throughout pregnancy to prevent/treat anaemia
- WHO recommends 60 mg elemental iron + 400 mcg folic acid daily
2. Tetanus Toxoid (TT) Immunization
- Unimmunized woman: 2 doses - 1st at 16-20 weeks, 2nd at 20-24 weeks (minimum 1 month interval)
- Previously immunized: 1 booster dose sufficient (provides cover for next 5 years)
- No pregnant woman should be denied even one dose if seen late in pregnancy
- Avoid TT at every successive pregnancy due to risk of hyperimmunization
3. Nutritional Counselling
- Adequate caloric intake, protein, vitamins, calcium
- Advice on tobacco cessation if applicable
4. Referral Services
- Inform about Janani Suraksha Yojana and other government incentives
Screening and Detection of Complications
(i) Anaemia
- Most common complication in pregnancy
- Haemoglobin < 11 g/dL indicates anaemia
- Severe anaemia (Hb < 7 g/dL) requires urgent management
(ii) Hypertensive Disorders
- Blood pressure monitoring at every visit
- Presence of hypertension + proteinuria = pre-eclampsia/toxaemia
- Requires close monitoring and timely referral
(iii) Asymptomatic Bacteriuria (ASB)
- Midstream urine culture is the recommended method for diagnosis
- Can lead to pyelonephritis, preterm birth, low birth weight if untreated
(iv) Gestational Diabetes
- Hyperglycaemia first detected during pregnancy
- Family history of diabetes to be recorded at first visit
- Screen with blood glucose testing
- Risk of hypertension, preeclampsia, large baby (>4.5 kg), stillbirth
(v) Syphilis (VDRL)
- Test blood at first visit; ideally retest later in pregnancy
- Congenital syphilis is preventable - treat with procaine penicillin
- Fetal infection most likely after the 6th month
Risk Approach - "High-Risk" Cases
The central purpose of ANC is to identify high-risk cases early. These include:
- Elderly primigravida (30 years and above)
- Short-statured primigravida (140 cm and below)
- Malpresentations (breech, transverse lie)
- Antepartum haemorrhage, threatened abortion
- Pre-eclampsia and eclampsia
- Anaemia
- Twins, hydramnios
- Previous stillbirth, intrauterine death, or manual removal of placenta
- Previous abortion
- Elderly grandmultiparas
- Prolonged pregnancy (>14 days after EDD)
- History of previous caesarean or instrumental delivery
- Pregnancy with systemic diseases: cardiovascular disease, kidney disease, diabetes, tuberculosis, liver disease, malaria, HIV, RTI/STI
Indications for Emergency Referral During Labour
- Fits or loss of consciousness
- Severe headache, blurring of vision, or diastolic BP >90 mmHg
- Prolapse of cord or hand
- Meconium-stained liquor or abnormal fetal heart rate
- Excessive "show" or bleeding during labour
- Collapse during labour
- Placenta not separated within 30 minutes after delivery
- Postpartum haemorrhage or collapse
- Temperature of 38°C or above during labour
Postnatal Transition
ANC care transitions into postnatal care after delivery:
- Mother observed for 48 hours after normal delivery
- Rooming-in (baby's crib beside mother) is encouraged to promote breastfeeding and bonding
- Postpartum complications to watch for: puerperal sepsis, thrombophlebitis
Park's Textbook of Preventive and Social Medicine, pp. 612-618
Fetal development
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Reading File
I now have comprehensive, authoritative data from "The Developing Human." Let me compile the full answer.
Fetal Development
Source: The Developing Human: Clinically Oriented Embryology
Overview of Prenatal Development
Human prenatal development is divided into two main periods:
| Period | Timeframe | Key Features |
|---|---|---|
| Embryonic period | Fertilization - end of Week 8 (Stage 1-23) | Rapid cell proliferation, differentiation, establishment of all major organs |
| Fetal period | Week 9 - Birth | Growth and functional differentiation of tissues/organs; rate of body growth increases |
By convention, gestational age is counted from the first day of the Last Normal Menstrual Period (LNMP). Embryonic/fertilization age begins ~14 days later at fertilization. The most critical stages of development occur in the first trimester (first 13 weeks).
Three Phases of Prenatal Development
1. Germinal Stage (Weeks 1-2)
- Begins at fertilization (union of oocyte and sperm) in the uterine tube
- Zygote undergoes cleavage as it travels toward the uterus
- Forms a morula (solid ball of cells), then a blastocyst (with inner cell mass + trophoblast)
- Implantation into endometrium at ~days 6-7
- Key structure formed: placenta (from trophoblast cells)
- Disturbances in this period either kill the embryo or are corrected by the embryo's regulatory properties - they do not typically cause birth defects
2. Embryonic Period (Weeks 3-8)
This is the most critical period of development. All major organ systems are established. Developmental disturbances here may give rise to major birth defects.
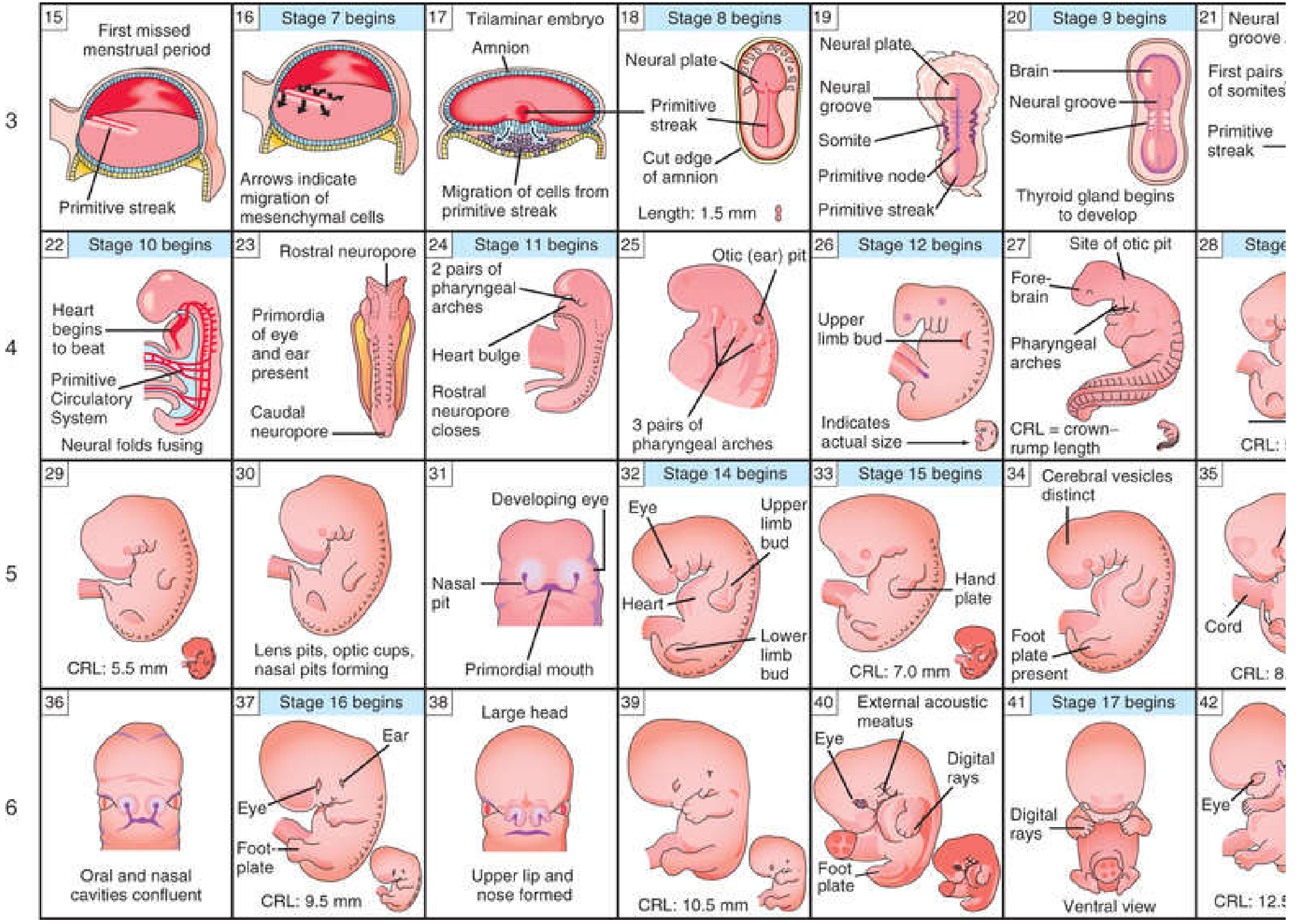
Week 3
- Primitive streak forms; gastrulation begins (converts bilaminar disc to trilaminar disc with 3 germ layers: ectoderm, mesoderm, endoderm)
- Neural plate and neural groove appear
- Somites begin forming
- Primitive circulatory system starts developing
Week 4
- Heart begins to beat (day 22-23)
- Neural folds fuse to form the neural tube
- Rostral neuropore closes
- Primordia of eyes and ears appear
- Pharyngeal arches form
- C-shaped cylindric embryo takes shape after folding
- Foregut, midgut, hindgut established
- CRL ~ 1.5-3 mm
Week 5
- Head growth exceeds all other regions (brain developing rapidly)
- Facial prominences develop
- Second pharyngeal arch overgrows 3rd and 4th (forms cervical sinus)
- Mesonephric kidneys develop (interim excretory organs)
- CRL ~ 4-7 mm
Week 6
- Lens pits, optic cups, nasal pits forming
- Upper and lower limb buds appear
- Heart bulge visible
- Oral and nasal cavities become confluent
- CRL ~ 9.5 mm
Timetable of Human Embryonic Development (Weeks 3-6):
Week 7
- Eyelids forming
- Grooves between digital rays indicate fingers
- Head large but chin poorly formed
- CRL ~ 13 mm
Week 8
- Upper limbs longer and bent at elbows
- Fingers distinct but still webbed
- External genitalia have begun to differentiate (but not yet distinguishable as male or female)
- Toes visible
- Large forehead
- By end of week 8 (Stage 23, day 56): all major organ systems established
- CRL ~ 27-31 mm
Embryonic to early fetal development (Weeks 7-10):
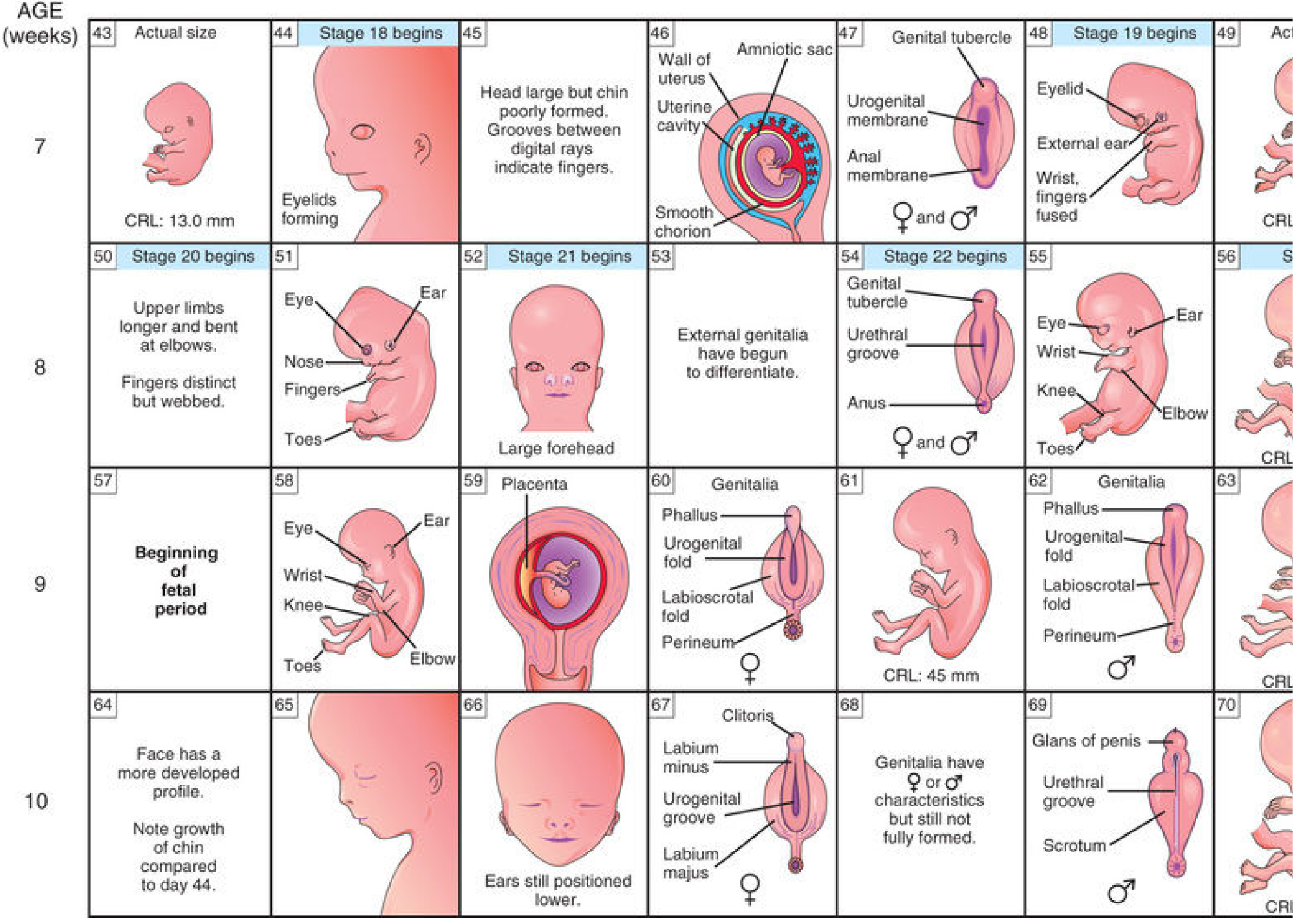
3. Fetal Period (Week 9 to Birth)
The name change from "embryo" to "fetus" is significant - it means the primordia of all major systems have formed. Development is now primarily rapid body growth and functional differentiation.
Highlights of Fetal Period: Week-by-Week
Weeks 9-12
| Week | CRL | Weight | Key Features |
|---|---|---|---|
| 9 | 50 mm | 8 g | Eyelids closing/closed. Head large and rounded. External genitalia NOT yet distinguishable. Some small intestines still in umbilical cord. Ears low set. |
| 10 | 61 mm | 14 g | Intestines now in abdomen. Early fingernail development. |
| 12 | 87 mm | 45 g | Sex distinguishable externally. Well-defined neck. Urine begins to form. |
- Liver is the major site of erythropoiesis (red blood cell formation)
- By end of 12 weeks: limbs well developed, face has characteristic human appearance
- Spontaneous movements occur (not yet felt by mother)
- Ossification centers appear in skeleton
Weeks 13-16
| Week | CRL | Weight | Key Features |
|---|---|---|---|
| 14 | 120 mm | 110 g | Head erect. Eyes face anteriorly. Ears near definitive position. Lower limbs well developed. Early toenail development. |
| 16 | 140 mm | 200 g | External ears stand out from head. |
- Rapid growth phase
- Scalp hair pattern determined
- Eyes and ears approach definitive positions
- Fetal movements may be recognized by experienced examiner (not yet by mother)
- Meconium formation begins in intestines
Weeks 17-20
| Week | CRL | Weight | Key Features |
|---|---|---|---|
| 18 | 160 mm | 320 g | Vernix caseosa covers skin. Quickening (first movements felt by mother) |
| 20 | 190 mm | 460 g | Head and body hair (lanugo) visible. |
- Quickening (first fetal movements perceived by mother) occurs at ~18 weeks in multiparas, ~20 weeks in primiparas
- Vernix caseosa (greasy white protective coating) appears on skin
- Lanugo (fine, downy hair) covers entire body
- Fetal movements increase
- Myelination of spinal cord begins
Weeks 21-25 (Viability Threshold)
| Week | CRL | Weight | Key Features |
|---|---|---|---|
| 22 | 210 mm | 630 g | Skin wrinkled, translucent, pink to red |
| 24 | 230 mm | 820 g | Fingernails present. Lean body. |
- Age of viability is approximately 22-26 weeks gestational age
- Innovations in neonatology have lowered this threshold (previously 28 weeks)
- Surfactant production begins - critical for lung function at birth
- Substantial weight gain
- Skin is red, wrinkled, and translucent (due to lack of subcutaneous fat)
Weeks 26-29
| Week | CRL | Weight | Key Features |
|---|---|---|---|
| 26 | 250 mm | 1000 g | Eyelids partially open. Eyelashes present. |
| 28 | 270 mm | 1300 g | Eyes wide open. Scalp hair present. Skin slightly wrinkled. |
- Eyes re-open (had been fused since ~week 9)
- CNS sufficiently mature to direct rhythmic breathing movements
- Adequate control of body temperature begins
- Survival possible with intensive neonatal care from 26 weeks onward
Weeks 30-34
| Week | CRL | Weight | Key Features |
|---|---|---|---|
| 30 | 280 mm | 1700 g | Toenails present. Body filling out. Testes descending. |
| 32 | 300 mm | 2100 g | Fingernails reach fingertips. Skin smooth (subcutaneous fat depositing). |
- Testes begin descending into scrotum
- Subcutaneous fat deposits give the body a more rounded appearance
- Lanugo begins to disappear from face
Weeks 35-38 (Full Term)
| Week | CRL | Weight | Key Features |
|---|---|---|---|
| 36 | 340 mm | 2900 g | Body plump. Lanugo almost absent. Toenails reach tips. Firm grasp. |
| 38 | 360 mm | 3400 g | Testes in scrotum. Nails extend beyond fingertips. |
- Normal birth weight at term: 2500-4200 g
- Skull bones remain separated (fontanelles and sutures) to allow passage through birth canal
- Lanugo almost completely shed
- Vernix caseosa present in skin folds
- Firm grasp reflex
Derivation from the Three Germ Layers
| Germ Layer | Derived Structures |
|---|---|
| Ectoderm | Brain, spinal cord, peripheral nervous system, skin epidermis, hair, nails, lens of eye, inner ear, enamel of teeth |
| Mesoderm | Skeleton, muscles (cardiac, skeletal, smooth), connective tissue, kidneys, gonads, cardiovascular system, spleen |
| Endoderm | Lining of GI tract, respiratory tract, urinary bladder; liver parenchyma, pancreas, thyroid, parathyroid, thymus |
Critical Periods of Development
| Organ System | Critical Period (from fertilization) | Effect of Teratogen |
|---|---|---|
| Brain (CNS) | 3-16 weeks (also postnatal) | Cognitive deficiency, neural tube defects |
| Heart | 3-7 weeks | Cardiac malformations |
| Eyes | 4-8 weeks | Cataracts, glaucoma, microphthalmia |
| Ears | 4-9 weeks | Deafness |
| Limbs | 4-8 weeks | Limb defects (phocomelia) |
| Teeth | 7 weeks - 8 years postnatal | Discolouration (tetracycline), hypoplasia |
| External genitalia | 7-9 weeks | Ambiguous genitalia |
- Weeks 1-2: Environmental disturbances kill the embryo OR are fully corrected - they do NOT cause birth defects (all-or-nothing law)
- Weeks 3-8 (organogenetic period): Most susceptible to teratogens - major structural birth defects result
- Week 9 to birth (fetal period): Physiologic defects and minor morphologic defects more likely; functional disturbances such as cognitive deficiency
Factors Influencing Fetal Growth
- Cigarette smoking - reduces fetal growth; associated with low birth weight
- Multiple pregnancy - each fetus grows more slowly than a singleton
- Alcohol and illicit drugs - fetal alcohol syndrome; IUGR
- Impaired uteroplacental blood flow - pre-eclampsia, placental abruption
- Genetic factors - chromosomal abnormalities, single gene disorders
Prematurity Classification
| Category | Gestational Age |
|---|---|
| Mild preterm | 32-37 weeks |
| Very preterm | 28-31 weeks |
| Extremely preterm | < 28 weeks |
Birth weight classification:
- Normal: 2500-4200 g
- Low birth weight (LBW): < 2500 g
- Very low birth weight (VLBW): < 1500 g
- Extremely low birth weight (ELBW): < 1000 g
Assessment of Fetal Status
| Method | Use |
|---|---|
| Ultrasonography | Gestational age, growth monitoring, anomaly detection |
| Amniocentesis | Chromosomal analysis, alpha-fetoprotein assay |
| Chorionic Villus Sampling (CVS) | Genetic diagnosis (10-13 weeks) |
| Fetal heart rate monitoring (CTG) | Assessment of fetal wellbeing |
| MRI | Detailed anatomy when ultrasound inconclusive |
| Percutaneous umbilical cord blood sampling (PUBS/cordocentesis) | Blood disorders, infection |
Crown-Rump Length (CRL) by transvaginal ultrasound is the most accurate method for estimating gestational age, with accuracy of ±1-4 days between 6-12 weeks.
The Developing Human: Clinically Oriented Embryology, pp. 46-292
- Miller's Anesthesia, 10th Edition, p. 10543
Schizophrenia
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
I now have comprehensive material from three authoritative sources. Let me compile the full answer.
Schizophrenia
Sources: Kaplan & Sadock's Comprehensive Textbook of Psychiatry, Goldman-Cecil Medicine, Goodman & Gilman's Pharmacological Basis of Therapeutics
Definition
Schizophrenia is the prototypical psychotic disorder, characterized by:
- Positive symptoms (hallucinations, delusions)
- Negative symptoms (affective flattening, abulia, apathy, social withdrawal)
- Disorganized symptoms (disorganized speech and behavior)
- Cognitive impairment
- Major impairment in one or more areas of functioning (occupational, interpersonal, self-care)
No single sign or symptom by itself justifies the diagnosis - the pattern and combination of symptoms matters.
Epidemiology
| Feature | Data |
|---|---|
| Lifetime prevalence | Slightly less than 1% |
| Annual incidence | ~15 per 100,000 (marked variability across populations) |
| Peak onset | Late adolescence to young adulthood |
| Sex difference | Slightly more common in males; earlier onset in males than females |
| Life expectancy | Shortened by 10-15 years |
| Suicide risk (lifetime) | ~5-6% |
Etiology and Pathobiology
The pathogenesis of schizophrenia remains unknown and is multifactorial.
Genetic Factors
- Twin studies show genetic factors account for up to 50% of risk
- Multiple gene loci are involved (highly heterogeneous)
- Large number of severe ultrarare mutations related to synaptic plasticity
- Higher concordance in monozygotic twins for negative symptoms than positive symptoms
- Increased familial risk for negative and disorganization symptoms over psychotic symptoms
Neuropathology
- Nongliotic neuropathologic process with subtle disruptions of cortical cytoarchitecture
- Postmortem brain studies reveal these subtle abnormalities (distinguishing it from neurodegenerative conditions)
- Considerable neuroimaging evidence supports cerebral dysfunction
- Frontal lobe abnormalities correlate particularly with negative symptoms
Neurotransmitter Hypotheses
Dopamine Hypothesis (most established):
- All clinically effective antipsychotic drugs have high affinity for D2 dopamine receptors
- Psychostimulants that increase extracellular dopamine can induce or worsen psychosis in schizophrenic patients
- Subcortical DA hyperfunction (especially striatum) → positive symptoms (respond well to antipsychotics)
- Prefrontal cortex DA hypofunction (mesocortical pathway) → negative and cognitive symptoms (treatment-refractory)
Glutamate:
- Glutamatergic systems also play an important role in psychotic symptom production
- NMDA receptor hypofunction is implicated (this explains why NMDA antagonists like PCP mimic schizophrenia)
Neurodevelopmental Theory
- A non-localizable brain lesion is either present at birth or acquired early in life
- Psychosocial factors and neurodevelopment interact with this lesion
- Psychosocial stressors can precipitate exacerbations and worsen the overall course
DSM-5 TR Diagnostic Criteria
Criterion A - Two or more of the following for a significant portion of time during a 1-month period (at least one must be 1, 2, or 3):
- Delusions
- Hallucinations
- Disorganized speech (derailment, incoherence)
- Grossly disorganized or catatonic behavior
- Negative symptoms (diminished emotional expression, avolition)
Criterion B - Level of functioning in work, interpersonal relations, or self-care is markedly below pre-onset level
Criterion C - Duration of at least 6 months (including at least 1 month of Criterion A symptoms; may include prodromal/residual phases)
Criterion D - Schizoaffective disorder and depressive/bipolar disorder with psychotic features ruled out
Criterion E - Not due to substance or medication effects
Criterion F - Not better explained by autism spectrum disorder or communication disorder
Note: ICD-11 requires only a minimum duration of 1 month (not including prodromal phase)
Core Symptom Domains
1. Psychotic Symptoms (Positive Symptoms)
Hallucinations:
- Perceptions without external stimuli - most commonly auditory (hearing voices)
- Voices may provide a running commentary, refer to the patient in third person, or give commands
- Schneiderian first-rank symptoms: hearing one's thoughts spoken aloud (écho de la pensée), voices referring to oneself, a running commentary - these were historically considered pathognomonic but are now known to occur in other disorders too
- Hallucinations can occur in any sensory modality (auditory most common; visual, tactile, olfactory also seen)
Delusions:
- Fixed, false beliefs held despite contradictory evidence
- Persecutory delusions most common
- Referential delusions - belief that neutral events/objects have special personal significance
- Delusions of control/passivity - belief that thoughts, feelings, or actions are controlled by external forces
- Other types: grandiose, religious, somatic, nihilistic, erotomanic
2. Negative Symptoms (Five Core Categories - NIMH MATRICS Consensus)
| Negative Symptom | Description |
|---|---|
| Avolition | Inability to initiate and persist in goal-directed activities |
| Anhedonia | Inability to experience pleasure from normally pleasurable activities |
| Asociality | Lack of interest in social interactions |
| Affective blunting | Reduced facial expression, vocal expression, expressive gestures |
| Alogia | Poverty of speech; sparse, brief, empty responses |
Key clinical points about negative symptoms:
- Associated with: male gender, poor premorbid function, earlier onset, longer duration of untreated illness
- Correlate with frontal lobe dysfunction and neuropathology
- Greater genetic heritability than positive symptoms
- More reliably associated with outcome than positive symptoms
- Reciprocal relationship with affective symptoms (more prominent affective symptoms = milder negative symptoms)
3. Disorganization Symptoms
Disorganized speech (formal thought disorder):
- Loose associations (derailment) - ideas slip off the track
- Tangentiality - replies to questions obliquely, never reaching the point
- Circumstantiality - excessive irrelevant detail before reaching the point
- Incoherence (word salad) - speech lacks logical connections
- Poverty of thought - little information conveyed
- Neologisms - invented words
- Echolalia - meaningless repetition of another's words
Disorganized behavior:
- Difficulty performing goal-directed activities
- Inappropriate affect
- Impulsive, unpredictable behavior
4. Motor Symptoms and Catatonia
Motor symptoms:
- Repetitive hand movements, complex purposeless movements
- Mannerisms (odd caricature of normal movements)
- Echopraxia (mimicking others' movements)
- Rocking, hand-wringing
Catatonia (separate specifier in DSM-5 TR):
- "Marked decrease in reactivity to the environment"
- Requires ≥3 of 12 motor signs: stupor, catalepsy, waxy flexibility, mutism, negativism, posturing, mannerism, stereotypy, agitation, grimacing, echolalia, echopraxia
- Lifetime prevalence in schizophrenia ~8%
- Catatonic excitement (agitated catatonia) is the most common type seen today
5. Cognitive Symptoms
- Impairment in working memory, attention, processing speed, executive function
- Deficits in recognition of emotion
- Cognitive impairment is a distinct domain from negative symptoms (modest but consistent correlation)
- Cognitive deficits are often present before first psychotic episode
Prodrome
- Social withdrawal, declining academic/occupational performance
- Attenuated psychotic symptoms (odd beliefs, magical thinking, ideas of reference)
- Disrupted sleep-wake cycle, irritability
- May begin years before overt psychosis
- Early identification and intervention in the prodromal phase is an active area of clinical focus
Course and Prognosis
- Typically characterized by acute psychotic episodes (exacerbations) superimposed on progressively deteriorating baseline functioning
- Prognosis often poor overall
- A small proportion may recover completely
- Antipsychotic drugs significantly reduce relapse rates
Predictors of poor prognosis:
- Male sex
- Prominent negative symptoms
- Younger age at first onset
- Enduring psychosocial stressors and family discord
- Longer duration of untreated psychosis (DUP)
Differential Diagnosis
| Disorder | Key Distinguishing Feature |
|---|---|
| Brief psychotic disorder | < 1 month duration; return to full baseline |
| Schizophreniform disorder | 1-6 months duration |
| Schizoaffective disorder | Concurrent schizophrenic symptoms + mood syndrome; with ≥2 weeks of psychosis without mood |
| Delusional disorder | Non-bizarre delusions ≥1 month; functioning otherwise not markedly impaired |
| Bipolar disorder with psychosis | Psychosis confined to mood episodes |
| Substance-induced psychosis | Psychosis due to drugs (stimulants, cannabis, PCP, etc.) |
| Autoimmune encephalitis | Especially anti-NMDA receptor encephalitis mimics first-episode psychosis |
| Mood disorder with psychotic features | Mood episode predominates |
Treatment
Antipsychotic Medications
First-Generation (Typical) Antipsychotics:
- Mechanism: D2 receptor antagonism
- Prototype: Chlorpromazine (first antipsychotic), Haloperidol
- Effective for positive symptoms
- NOT effective for negative or cognitive symptoms
- Side effects: extrapyramidal symptoms (EPS) - parkinsonism, akathisia, acute dystonia, tardive dyskinesia; hyperprolactinemia
Second-Generation (Atypical) Antipsychotics:
- Lower D2 receptor occupancy (faster dissociation) + serotonin 5-HT2A antagonism
- Lower rates of EPS and tardive dyskinesia
- Less likely to cause hyperprolactinemia
- Efficacy for positive symptoms is generally NOT better than first-generation
- Important agents:
| Drug | Key Features |
|---|---|
| Clozapine | Greatest efficacy (including treatment-resistant cases); requires monitoring for agranulocytosis; associated with lowest relapse rates |
| Risperidone | Commonly used; highest prolactin elevation among atypicals |
| Olanzapine | Effective; significant metabolic side effects |
| Quetiapine | Low EPS; sedating |
| Aripiprazole | Partial D2 agonist; weight-neutral |
| Cariprazine | May be superior to risperidone for predominantly negative symptoms |
Long-Acting Injectable (LAI) antipsychotics:
- Associated with greatest reduction in relapse rates (along with clozapine)
- Addresses the major problem of medication non-adherence
Metabolic Monitoring
- Second-generation antipsychotics contribute to obesity and metabolic syndrome in chronic schizophrenia
- Regular monitoring of weight, glucose, lipids is mandatory
Psychosocial Interventions
- Comprehensive psychosocial rehabilitation programs are important for functional outcomes
- Assertive Community Treatment (ACT)
- Cognitive Behavioral Therapy for psychosis (CBTp)
- Family psychoeducation
- Social skills training
- Supported employment
- Prompt use of psychosocial programs at initial onset may improve long-term course
Comorbidities
| Comorbidity | Notes |
|---|---|
| Depression | Can mimic negative symptoms (important to distinguish); Calgary Depression Scale used |
| Anxiety / PTSD | PTSD amplifies schizophrenia core symptom severity |
| Metabolic syndrome | Worsened by antipsychotic medications |
| Substance use disorders | Common; cannabis especially associated with psychosis exacerbation |
| Cardiovascular disease | Major contributor to reduced life expectancy |
| Suicide | Lifetime risk ~5-6% |
Kaplan & Sadock's Comprehensive Textbook of Psychiatry, pp. 4381-4428
Goldman-Cecil Medicine, International Edition, pp. 3764-3765
Goodman & Gilman's The Pharmacological Basis of Therapeutics, pp. 320-321
This is a shared conversation. Sign in to Orris to start your own chat.