Hey orris can you teach me signs of pulmonary embolism in chest x-ray with image and reason why it occurs please
Reading File
Finding Sources
Searching the Web
pulmonary embolism chest x-ray signs Westermark Hampton's hump Fleischner sign radiology
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Reading Web Page
https://radiopaedia.org/articles/signs-of-pulmonary-embolus-…
Reading File
Finding Sources
Loading Image
Loading Image
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the textbook content, authoritative images, and clinical details needed to give a thorough answer. Let me compile the complete response.
Pulmonary Embolism (PE) - Chest X-Ray Signs
The chest X-ray in PE is an important but humbling tool. As Harrison's Principles of Internal Medicine (2025) states: "A normal or nearly normal chest x-ray often occurs in PE" - and that near-normal film in a hypoxic, tachycardic patient is itself a clue. The named signs below are specific but not sensitive, meaning their presence is helpful but their absence does not rule out PE.
Why do CXR signs occur? - The Pathophysiology
When a thrombus (usually from deep vein thrombosis of the legs) travels to the pulmonary circulation, it causes:
- Obstruction of blood flow - the blocked artery receives no blood, so the lung tissue it supplied gets no perfusion, while ventilation continues (V/Q mismatch). The downstream segment becomes hyperlucent (Westermark sign).
- Pulmonary infarction - if the obstruction is large and collateral bronchial circulation is insufficient, the lung tissue undergoes ischemic necrosis, producing a pleural-based opacity (Hampton's hump).
- Proximal artery dilation - blood backs up behind the clot, distending the central pulmonary arteries (Fleischner sign, Palla's sign, Knuckle sign).
- Reactive pleural effusion - inflammation from the infarcted segment causes fluid to leak into the pleural space.
- Atelectasis/Raised hemidiaphragm - loss of surfactant in ischemic lung, reduced tidal volume due to pain, and diaphragmatic irritation.
Classic Named CXR Signs of PE
Here is a summary overview of all the main signs:

1. Hampton's Hump
What it looks like: A wedge-shaped (triangular), pleural-based opacity with the flat base touching the pleural surface and the rounded apex pointing inward toward the hilum. Classically in the lower lobes, above the diaphragm.
Why it occurs: This represents pulmonary infarction - not just ischemia. When the embolus is large enough to overcome collateral bronchial arterial supply, the distal lung tissue undergoes hemorrhagic infarction and consolidation. The shape is wedge-shaped because it follows a pulmonary arterial territory (a cone-shaped segment of lung).
"Hampton's hump - which is usually due to pulmonary infarction" - Harrison's Principles of Internal Medicine, 22nd ed.
Clinical note: More likely to appear with large, multiple emboli. Associated with pleuritic chest pain and hemoptysis (blood-stained infarct fluid).
Below is a real CXR showing Hampton's Hump (wedge opacity at left lung base, with confirmed large clot on CT):

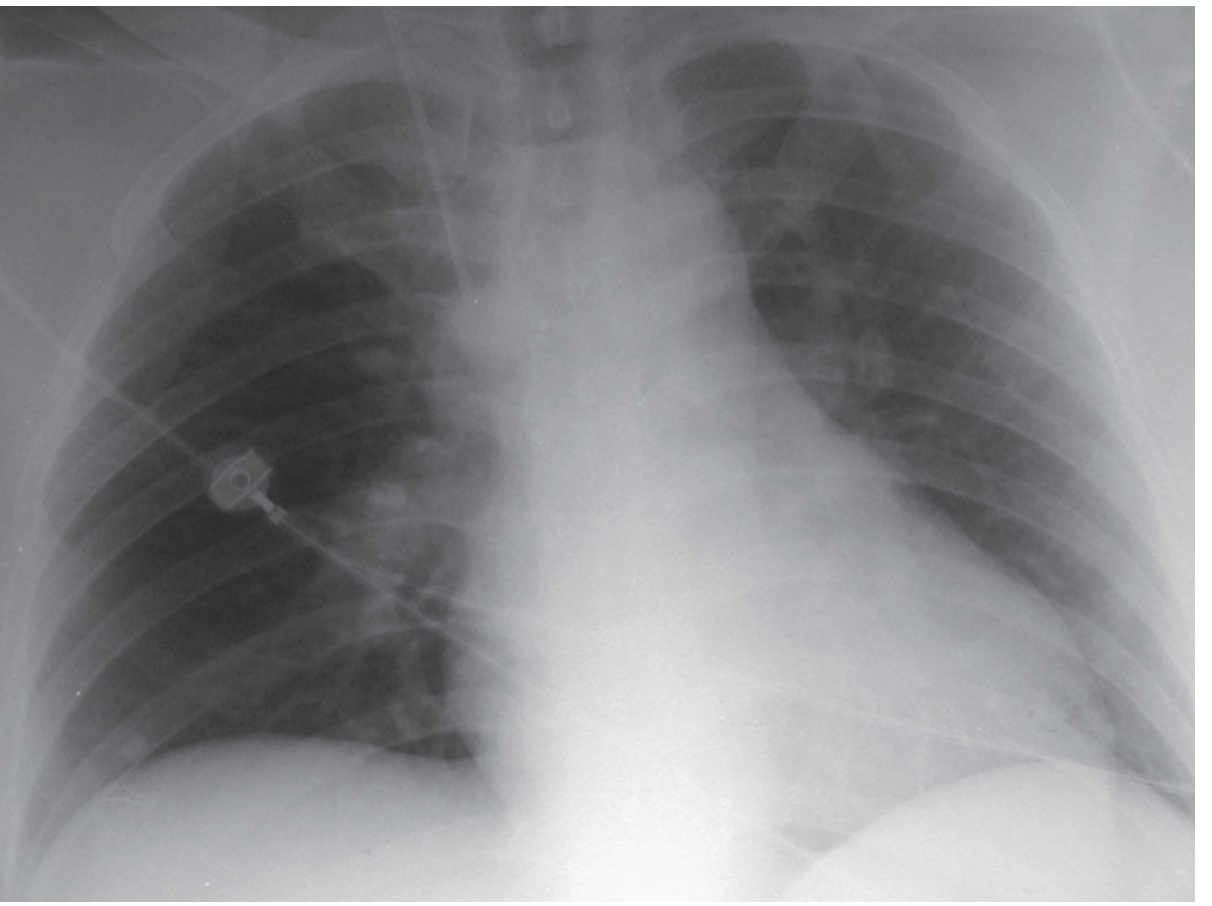
2. Westermark Sign
What it looks like: Focal hyperlucency (darker/blacker area) of one lung zone distal to the embolus compared to the rest of the lung. The affected zone appears relatively "empty" of vessels.
Why it occurs: When the pulmonary artery is obstructed, blood flow ceases to the distal lung. With no blood in those capillaries, the lung field appears darker on X-ray because there is less tissue density. This is called oligemia - a reduction of blood in the lung parenchyma. The sharp cut-off between normal and oligemic lung can sometimes be seen.
"Focal oligemia (Westermark's sign) indicates large central embolic occlusion." - Braunwald's Heart Disease, p. 3350
This is the Westermark sign in Murray & Nadel's Textbook (eFigure 81.6) - note the right thorax appears more hyperlucent (darker/blacker) than the left, indicating reduced blood flow:
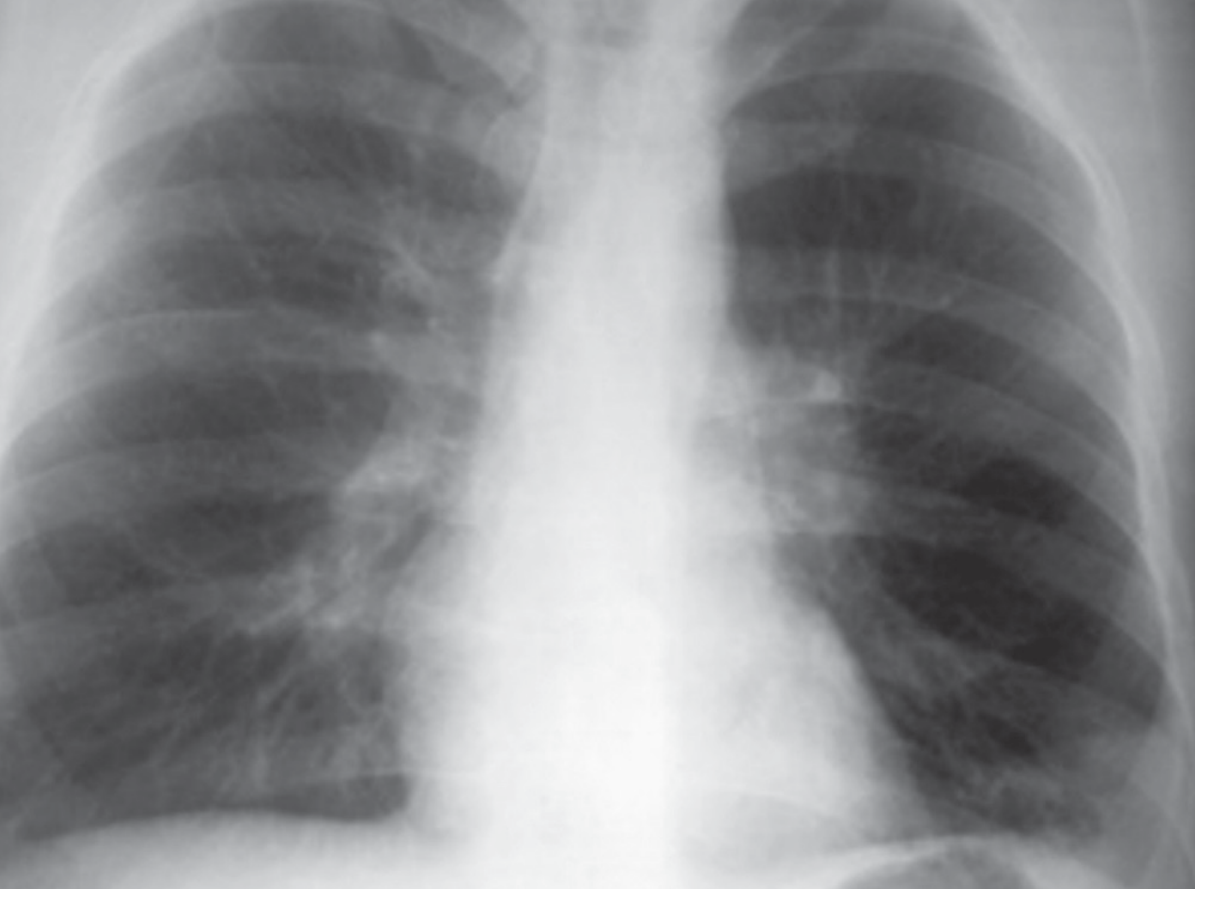
3. Fleischner Sign
What it looks like: Prominent (enlarged) central pulmonary artery - the right or left main pulmonary artery appears wider/more opaque than normal at the hilum.
Why it occurs: A large embolus lodging in or proximal to the main pulmonary artery causes distension of the vessel due to backpressure from the clot. The engorged pulmonary artery appears as a prominent hilar shadow.
"Fleischner sign (prominence of the central pulmonary artery)" - Murray & Nadel's Textbook of Respiratory Medicine
This CXR shows the Fleischner + Westermark sign together (eFigure 81.8) - enlarged left pulmonary artery with left thorax hyperlucency:
4. Palla's Sign
What it looks like: Enlargement of the right descending pulmonary artery (also called the right interlobar pulmonary artery) - it appears wider than normal in the right hilum.
Why it occurs: Similar to the Fleischner sign - clot burden in the right pulmonary artery causes dilatation of the descending branch. This is the most commonly measured vessel for assessing central PE on CXR.
"An enlarged right descending pulmonary artery (Palla's sign)" - Harrison's Principles of Internal Medicine 22nd ed.
5. Knuckle Sign
What it looks like: An abrupt tapering or cutoff of a pulmonary artery, giving it a "knuckle" shape - the artery appears to stop suddenly rather than taper gradually.
Why it occurs: The embolus sits directly in the artery lumen, causing the vessel to end abruptly at the level of the clot. The proximal artery is distended (swollen with backed-up blood), and then suddenly narrows at the site of obstruction, creating a knuckle-like contour.
6. Pleural Effusion
What it looks like: Blunting of the costophrenic angle (the usual finding for small effusions). The majority are small.
Why it occurs: Pleural inflammation from an adjacent pulmonary infarct causes fluid to leak into the pleural space. According to the PIOPED study, pleural effusions occur in ~half of PE patients but are usually small. When tapped, they are exudative with normal glucose and neutrophil predominance.
"Although pleural effusions are seen in almost half of the patients, the majority of effusions are small and involve only blunting of the costophrenic angle." - Murray & Nadel's Textbook of Respiratory Medicine
7. Elevated Hemidiaphragm
What it looks like: One hemidiaphragm appears higher than normal on the CXR.
Why it occurs: Loss of lung volume (atelectasis) in the infarcted/ischemic segment causes the lung to shrink and the diaphragm to ride up. Diaphragmatic irritation from adjacent pleural effusion or infarction also contributes.
8. Atelectasis / Pulmonary Opacities
What it looks like: Linear or plate-like opacities (Fleischner lines/discoid atelectasis), or irregular consolidation.
Why it occurs: In PIOPED, atelectasis and pulmonary opacities were actually the most common CXR findings in PE (though non-specific). They result from:
- Loss of surfactant in ischemic lung tissue
- Splinting of breathing due to pleuritic pain
- Mucus plugging from reduced ventilation
"In the PIOPED study, the most common radiographic abnormalities were atelectasis and pulmonary opacities." - Murray & Nadel's Textbook of Respiratory Medicine
9. Normal CXR (Important!)
A normal or near-normal CXR in a patient with significant hypoxemia and dyspnea is itself a red flag for PE. Most other causes of severe hypoxia (pneumonia, pulmonary edema, pneumothorax) show clear CXR changes. PE can present with a deceptively clear film.
Quick Summary Table
| Sign | Appearance on CXR | Mechanism |
|---|---|---|
| Hampton's Hump | Wedge-shaped pleural-based opacity | Pulmonary infarction - hemorrhagic necrosis of lung |
| Westermark Sign | Focal hyperlucency (dark zone) distal to clot | Oligemia - no blood flow to distal vessels |
| Fleischner Sign | Enlarged central pulmonary artery | Backpressure distends proximal artery |
| Palla's Sign | Enlarged right descending pulmonary artery | Same as Fleischner, specific vessel |
| Knuckle Sign | Abrupt arterial cutoff | Clot physically blocks and distends vessel |
| Pleural Effusion | Costophrenic angle blunting | Reactive exudate from adjacent infarct |
| Raised hemidiaphragm | Unilateral high diaphragm | Volume loss, atelectasis, diaphragmatic irritation |
| Atelectasis | Linear/plate-like opacities | Surfactant loss, splinting, mucus plugging |
| Normal CXR | Appears normal despite severe symptoms | No structural damage yet |
Important Clinical Caveat
None of these signs are pathognomonic or highly sensitive. As Murray & Nadel's points out, signs like the Westermark sign, Hampton's hump, and Fleischner sign "have not proved to have discriminatory value" in large studies. The main purpose of the CXR in suspected PE is to:
- Exclude alternative diagnoses (pneumothorax, pneumonia, heart failure)
- Assess the lung parenchyma before V/Q scanning
The gold standard for diagnosis is CT pulmonary angiography (CTPA).
Sources: Murray & Nadel's Textbook of Respiratory Medicine; Harrison's Principles of Internal Medicine 22nd ed. (2025); Braunwald's Heart Disease; Radiopaedia - Signs of PE on chest radiography; St. Vincent's University Hospital Radiology
This is a shared conversation. Sign in to Orris to start your own chat.