I need to know each and every detail of sigmoid colon cancer. Its etiology, pathophysiology, investigations, treatment everything
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Searching PubMed
"sigmoid colon cancer" AND treatment
Reading File
Reading File
Loading Image
Loading Image
I now have all the material needed for a complete, detailed answer. Here is the comprehensive overview:
Sigmoid Colon Cancer - Complete Clinical Guide
1. ANATOMY AND BACKGROUND
The sigmoid colon is the S-shaped segment of the large intestine extending from the descending colon (at the left iliac fossa) to the rectosigmoid junction. Its blood supply comes from the sigmoid arteries and superior rectal artery, both branches of the inferior mesenteric artery (IMA). The IMA originates from the aorta 2-3 cm caudal to the inferior mesenteric vein and is surrounded by the mesenteric and hypogastric nervous plexus - critical to know for surgical planning.
Colorectal cancer (CRC) is the third most common malignancy worldwide, with higher incidence in Western industrialized countries. The sigmoid colon is one of the most common sites for CRC, accounting for a significant proportion of left-sided tumors.
2. ETIOLOGY AND RISK FACTORS
Modifiable / Environmental Risk Factors
- Diet: High saturated/polyunsaturated fat diet increases risk; high fiber and oleic acid (olive oil, fish oil) diet is protective. Increased red meat and decreased fiber specifically linked.
- Obesity and sedentary lifestyle: Dramatically increase cancer-related mortality
- Alcohol consumption: Associated with increased CRC incidence
- Smoking: Associated with increased risk of colonic adenomas, especially after >35 years of use
- Type 2 diabetes / insulin resistance
- Pelvic irradiation: May increase risk, particularly for rectal/sigmoid cancers
Non-Modifiable Risk Factors
- Age >50 (incidence rises sharply; screening starts at 45 per current guidelines)
- Personal history of polyps or CRC
- Family history of CRC
- Inflammatory bowel disease (IBD): Long-standing colitis (ulcerative colitis or Crohn's) increases risk - duration and extent of colitis correlate with risk; presence of primary sclerosing cholangitis further increases risk
- Acromegaly: Elevated IGF-1 increases risk
- Ureterosigmoidostomy: Increases risk of adenoma and carcinoma at the junction
Hereditary Syndromes
| Syndrome | Gene | Mechanism | CRC Risk |
|---|---|---|---|
| Familial Adenomatous Polyposis (FAP) | APC (chr 5q) | Loss of WNT signaling suppression | ~100% by age 50 |
| Lynch Syndrome (HNPCC) | MLH1, MSH2, MSH6, PMS2 | Mismatch repair deficiency (MSI-H) | 40-80% lifetime |
| MUTYH-associated polyposis | MUTYH | Base excision repair defect | Elevated |
| Serrated polyposis syndrome | BRAF/RNF43 | Serrated pathway | Elevated |
- FAP accounts for ~1% of all CRC but has provided the most insight into CRC molecular biology.
- Lynch syndrome accounts for ~5% of all CRC.
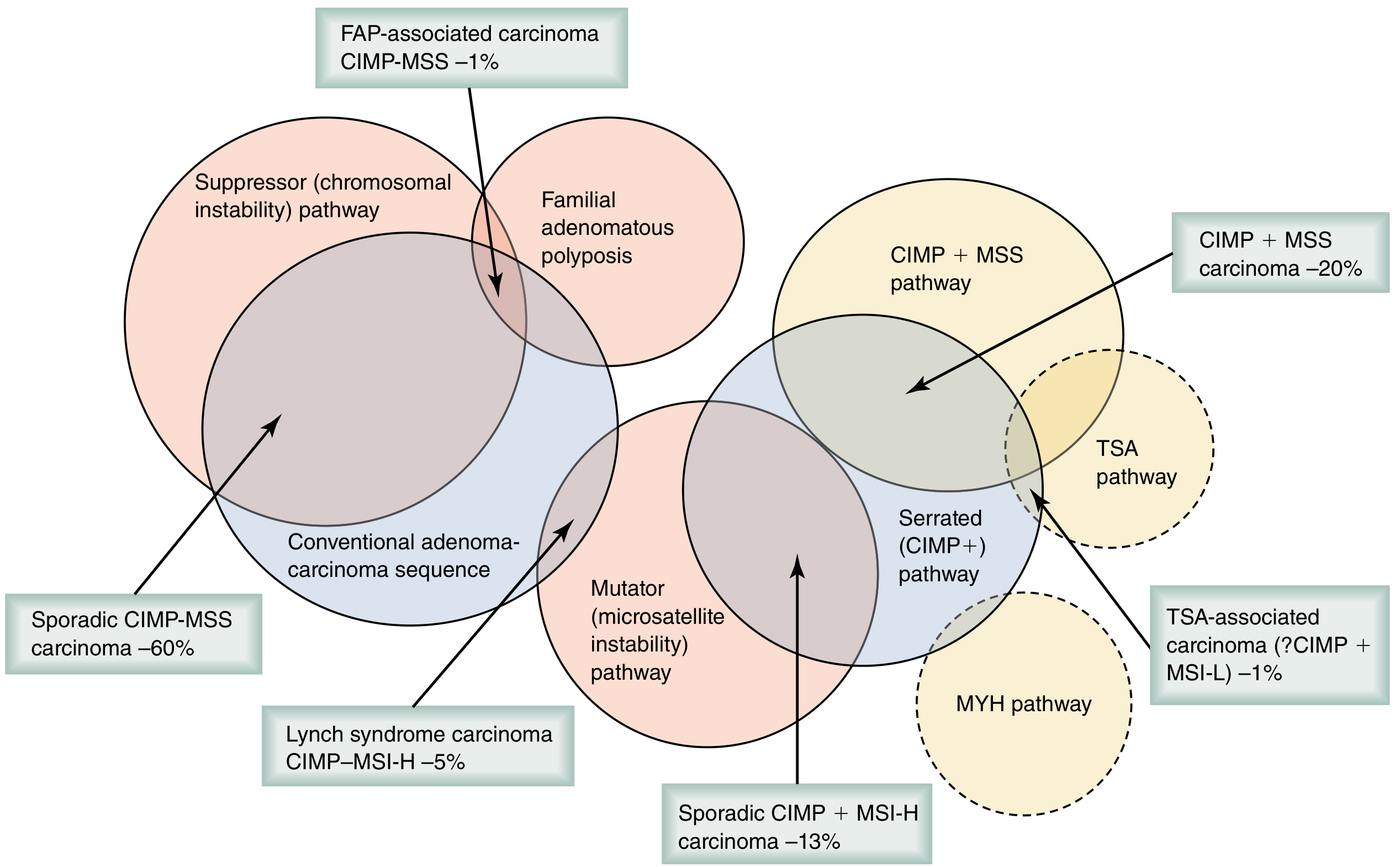
3. PATHOPHYSIOLOGY - MOLECULAR MECHANISMS
Three distinct but overlapping molecular pathways lead to CRC development:
Pathway 1: Chromosomal Instability (CIN) - 65-70% of CRCs
This is the classic adenoma-to-carcinoma sequence (Fearon and Vogelstein model):
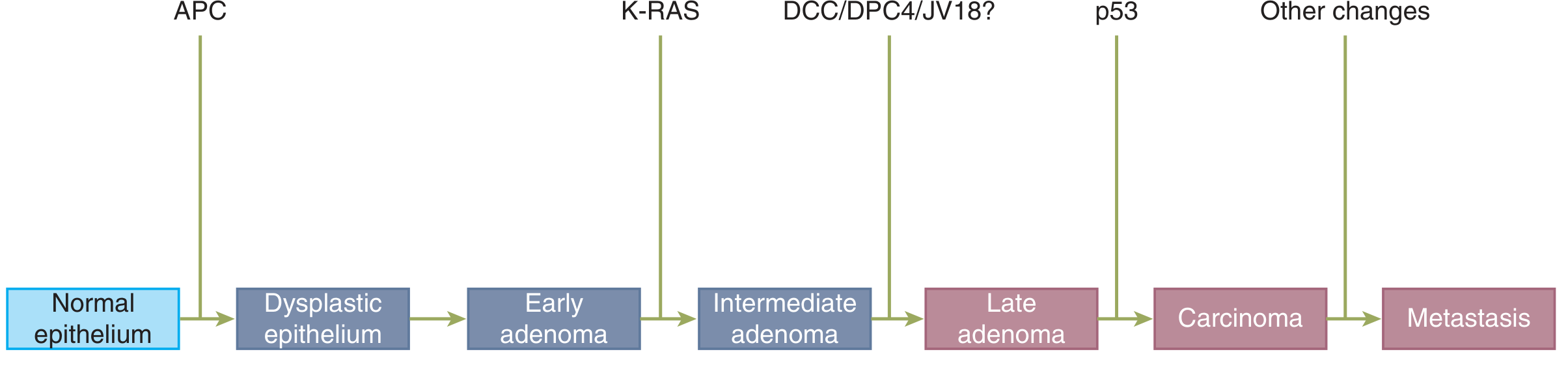
- Step 1: Mutation of APC gene (chr 5q) - activates WNT/β-catenin signaling → dysplastic epithelium → early adenoma. Present in 80% of CIN tumors.
- Step 2: KRAS mutation - promotes growth and extension of the adenoma
- Step 3: Loss of DCC/SMAD4 (chr 18q)
- Step 4: TP53 mutation - promotes invasion into surrounding tissue
- Result: Late adenoma → carcinoma → metastasis
Pathway 2: Serrated / Methylator (CpG Island Methylator Phenotype - CIMP) - 15-20%
- Initiating event: BRAF mutation
- Subsequent hypermethylation of promoter regions of tumor suppressor genes and DNA repair genes → silenced gene expression
- Methylation of CG-rich areas (CpG islands) in the 5' region of genes
- More common in older patients, females, and the right colon (though serrated lesions can occur in sigmoid too)
- Can be CIMP+ MSS (~20%) or CIMP+ MSI-H (~13%)
Pathway 3: Microsatellite Instability (MSI/Mutator) - 12-15%
- Loss of mismatch repair (MMR) function via:
- Germline pathogenic variant in MLH1, MSH2, MSH6, or PMS2 (Lynch syndrome)
- Hypermethylation of the MLH1 promoter (sporadic)
- Double somatic mutation in an MMR gene
- Loss of MMR leads to accumulation of DNA base-pair mismatches in microsatellite repeats → MSI-H
- Pathologic features: Crohn-like reaction, mucin, lymphocytic infiltration, high tumor mutational burden (TMB)
- MSI-H tumors actually have better prognosis (~15% improvement in survival vs MSS)
CRC Molecular Subtypes (Consensus Molecular Subtypes - CMS)
Four subtypes based on gene expression and transcriptome analysis (CMS1-4), each with distinct biology, clinical behavior, and drug sensitivity.
Microbiome Contribution
Intestinal microbes metabolize nitrosamines and polycyclic amines (carcinogenic). Conversely, butyrate (from fermentation of nondigestible carbohydrates) has anti-inflammatory and antitumor activity. Mucosal inflammation from intestinal infection may be an initiating factor.
4. PATHOLOGY
Macroscopic Types
- Polypoid/fungating (most common on the right, but occurs anywhere)
- Annular/constricting ("apple-core" lesion) - more common in sigmoid and left colon, causes obstruction
- Ulcerating
- Diffuse infiltrating (linitis plastica type)
Microscopic / Histological Types
- Adenocarcinoma - the vast majority (~95%)
- Mucinous adenocarcinoma - >50% extracellular mucin; worse prognosis
- Signet ring cell carcinoma - >50% signet ring cells; very poor prognosis (5-year survival 9-36%)
- Medullary carcinoma - associated with MSI-H; better prognosis
- Poorly differentiated carcinoma
Spread
- Direct: Through the bowel wall layers (mucosa → submucosa → muscularis propria → serosa/peritoneum → adjacent organs)
- Lymphatic: To pericolic, intermediate, and apical nodes along the sigmoid arteries and IMA
- Hematogenous: Portal vein → liver (most common distant site); also lungs, adrenals, ovaries, bone
- Peritoneal: Transcoelomic spread → peritoneal carcinomatosis
- Implantation: At anastomosis (rare if adequate margins)
5. CLINICAL PRESENTATION
Sigmoid colon tumors tend to cause left-sided symptoms due to the annular growth pattern and the narrower caliber of the left colon:
- Change in bowel habits: Alternating constipation and diarrhea, "pencil-thin stools" (classic for sigmoid obstruction)
- Rectal bleeding / hematochezia: Fresh or dark red blood mixed with stool
- Abdominal pain: Left iliac fossa or diffuse
- Microcytic (iron-deficiency) anemia: From chronic occult blood loss - may present as fatigue
- Obstructive symptoms: Increasing distension, obstipation, vomiting (in late/emergency cases)
- Perforation: Peritonitis, fever, acute abdomen (rare, emergency presentation)
- Palpable mass: Left iliac fossa in advanced disease
- Systemic symptoms: Weight loss, anorexia, cachexia in advanced disease
Many sigmoid cancers are identified on screening colonoscopy before symptoms develop.
6. INVESTIGATIONS
Blood Tests
- Complete Blood Count (CBC): Microcytic hypochromic anemia (iron deficiency from occult bleeding)
- Comprehensive Metabolic Panel: Liver function tests (for metastases), albumin (nutritional status)
- Serum CEA (Carcinoembryonic Antigen): Tumor marker. Pre-op CEA >5 ng/mL predicts worse disease-free survival. Used for monitoring recurrence post-resection, not for screening.
- CA 19-9: Less specific, used as adjunct
- Coagulation profile, Group & Save: Pre-operative
- LFTs, ALP: For liver metastases
Stool-Based Tests (for screening / initial detection)
- Fecal Occult Blood Test (FOBT) - annual
- Fecal Immunochemical Test (FIT) - annual
- Stool DNA-FIT (Cologuard) - every 1-3 years
- Any positive stool test → colonoscopy
Endoscopy
- Colonoscopy with biopsy: Gold standard for diagnosis. Visualizes the lesion, allows biopsy for histological confirmation, and detects synchronous polyps or cancers.
- CT Colonography (Virtual Colonoscopy): Every 5 years as a screening tool; useful if colonoscopy is incomplete
- Flexible Sigmoidoscopy: Every 5 years; detects sigmoid lesions specifically but misses proximal lesions
Imaging for Staging
- CT Chest/Abdomen/Pelvis with contrast: Primary staging modality. Assesses:
- T stage (local tumor extent, peritoneal involvement)
- N stage (regional lymphadenopathy)
- M stage (liver, lung, peritoneal metastases)
- MRI Abdomen/Pelvis: Better soft tissue resolution; used for liver metastasis characterization; essential for rectal cancer (mesorectal margin assessment), less routine for sigmoid
- PET-CT: Not routinely indicated; reserved for patients being considered for definitive resection of oligometastatic disease (e.g., isolated liver or lung metastasis)
- Chest X-ray: Baseline lung assessment
- Transrectal Ultrasound: Not applicable to sigmoid (used for rectal cancer staging)
Pathological / Molecular Testing (Biopsy)
- Histology and grade: Adenocarcinoma type, differentiation
- MMR status (IHC for MLH1, MSH2, MSH6, PMS2) or MSI testing: Guides immunotherapy eligibility and prognosis; Lynch syndrome screening
- KRAS/NRAS mutation testing: Predicts resistance to anti-EGFR therapy (cetuximab, panitumumab)
- BRAF V600E mutation: Poor prognosis in metastatic CRC; specific therapy targets available
- Tumor Mutation Burden (TMB): High TMB predicts response to immune checkpoint inhibitors (ICIs)
- NTRK fusion testing: Rare (<1%), usually MSI-H, specific TKI therapy available
7. STAGING
TNM Staging (AJCC 8th Edition)
Tumor (T):
| Stage | Definition |
|---|---|
| Tis | Carcinoma in situ (intramucosal, no through muscularis mucosa) |
| T1 | Invades submucosa |
| T2 | Invades muscularis propria |
| T3 | Through muscularis propria into pericolorectal tissues |
| T4a | Through visceral peritoneum |
| T4b | Invades/adheres to adjacent organs |
Nodes (N):
| Stage | Definition |
|---|---|
| N0 | No regional nodes |
| N1a | 1 positive node |
| N1b | 2-3 positive nodes |
| N1c | Tumor deposits in subserosa/mesentery, nodes negative |
| N2a | 4-6 positive nodes |
| N2b | 7+ positive nodes |
Distant Metastasis (M):
| Stage | Definition |
|---|---|
| M0 | No distant metastasis |
| M1a | 1 site/organ, no peritoneal |
| M1b | 2+ sites/organs, no peritoneal |
| M1c | Peritoneal metastasis |
Overall Stage Groups
| Stage | TNM | 5-Year Survival (approx.) |
|---|---|---|
| 0 | Tis N0 M0 | ~100% |
| I | T1-2 N0 M0 | ~90% |
| IIA | T3 N0 M0 | ~80% |
| IIB | T4a N0 M0 | ~72% |
| IIC | T4b N0 M0 | ~65% |
| IIIA | T1-2 N1/N1c | ~83% |
| IIIB | T3-4a N1, T2-3 N2a | ~64% |
| IIIC | T4a N2a, T3-4a N2b, T4b N1-2 | ~44% |
| IVA | Any T, any N, M1a | ~14% |
| IVB | Any T, any N, M1b | ~13% |
| IVC | Any T, any N, M1c | ~3% |
8. TREATMENT
A. Surgery (Primary Treatment for Localized Disease)
Sigmoid colectomy is the standard operation for sigmoid colon cancer:
- Extent: Segmental sigmoid resection following oncologic principles. The distal transection is at the upper rectum; proximal resection is at the distal descending colon.
- Vascular ligation: The IMA (or sigmoid arteries) are ligated at their origin (high ligation) to ensure harvest of the regional lymph nodes en bloc. A recent meta-analysis (2025) confirms the value of IMA ligation level in sigmoid/rectal cancer.
- Anastomosis: End-to-end colorectal anastomosis, typically with a double-stapled technique.
- Lymphadenectomy: Minimum 12 lymph nodes must be harvested for adequate staging.
Surgical Approach:
- Laparoscopic / Robotic (preferred): Less postoperative pain, shorter hospital stay, faster return of bowel function, lower wound infection rate - with equivalent oncologic outcomes to open surgery (proven by COST, COLOR, CLASSICC trials).
- Open (laparotomy): When minimally invasive not feasible.
For Obstructing Sigmoid Cancer:
- Urgent surgery is common
- Segmental resection of the primary tumor
- If proximal bowel is perforated/ischemic: subtotal colectomy
- Hartmann's procedure (resection + end colostomy + closure of rectal stump): Historically preferred; now primary anastomosis may be done in hemodynamically stable patients
- Endoscopic stenting as bridge to surgery: Relieves obstruction, allows elective surgery with higher rates of primary anastomosis and laparoscopic completion; contraindicated if ischemia or perforation suspected
For Synchronous Metastatic Disease:
- Symptomatic primary: Address primary first (palliation)
- Asymptomatic primary: Systemic treatment first
- Resectable liver metastasis: Combined or staged resection (neoadjuvant chemotherapy improves progression-free survival)
- Resectable lung metastasis: Surgical resection improves survival
- Peritoneal metastasis (selected): Cytoreductive surgery + HIPEC (hyperthermic intraperitoneal chemotherapy) after multidisciplinary discussion
B. Chemotherapy
Adjuvant Chemotherapy (post-surgery, curative intent):
- Stage I: No adjuvant chemo needed
- Stage II (low risk): Observation; chemotherapy generally not beneficial, especially in patients >70
- Stage II (high risk): Consider adjuvant chemo. High-risk features: poorly differentiated histology, LVI, bowel obstruction, <12 nodes sampled, localized perforation, positive/close margins, T4, high tumor budding
- Stage III: Adjuvant chemotherapy recommended
Preferred Adjuvant Regimens:
- CAPEOX (capecitabine + oxaliplatin): 3 months sufficient for low-risk stage III (T1-3 N1); 6 months for high-risk
- FOLFOX (leucovorin + 5-FU + oxaliplatin): 6 months for high-risk stage III (T4/N2); 3 months inferior to 6 months in this group
- Addition of oxaliplatin does NOT improve survival in stage II or patients >70
For dMMR/MSI-H stage II: Observation without adjuvant chemotherapy (counterintuitive but supported by evidence - fluoropyrimidines less effective)
Neoadjuvant Chemotherapy: Not standard for colon cancer (unlike rectal), but dMMR tumors show ~95% major pathologic response to checkpoint inhibitors (NICHE study) - an evolving area
Stage IV (Metastatic) Chemotherapy:
- First-line: Fluoropyrimidine (5-FU/leucovorin or capecitabine) + oxaliplatin (FOLFOX/CAPEOX) or irinotecan (FOLFIRI)
- Biological agents added based on molecular profile:
- Bevacizumab (anti-VEGF): Combined with FOLFOX or FOLFIRI in RAS-mutant CRC; objective response ~70%
- Cetuximab / Panitumumab (anti-EGFR): Only in RAS/NRAS/KRAS wild-type (no mutation) tumors; ineffective with KRAS or NRAS mutations
- BRAF V600E inhibitors (e.g., encorafenib + cetuximab): For BRAF-mutant metastatic CRC
- Pembrolizumab / Nivolumab (anti-PD-1): For MSI-H/dMMR metastatic CRC - pembrolizumab approved first-line
- TRK inhibitors (larotrectinib, entrectinib): For NTRK fusion-positive CRC (rare)
C. Radiation Therapy
- Sigmoid colon cancer: Radiation is NOT routinely used for colon cancer (unlike rectal cancer) due to the mobile nature of the colon and radiosensitivity of adjacent bowel.
- Exception: Locally advanced/fixed sigmoid cancers invading adjacent structures (T4b) may receive preoperative chemoradiotherapy.
- Recurrence: In selected recurrent cases, intraoperative radiation therapy (IORT/brachytherapy) may be added.
D. Endoscopic/Local Treatment
- Endoscopic mucosal resection (EMR) / Endoscopic submucosal dissection (ESD): For T1 lesions (confined to submucosa) without high-risk features (poor differentiation, LVI, deep submucosal invasion). Curative in select early-stage cases.
- Palliative colonic stenting: For malignant obstruction in patients unfit for surgery or as bridge to surgery.
9. PROGNOSTIC FACTORS
Beyond TNM stage, the following independently affect prognosis:
- Serum CEA >5 ng/mL (pre- and post-op): Worse disease-free survival
- Lymphovascular invasion (LVI): Worse DFS and OS in stage II/III
- Perineural invasion (PNI): Independent poor prognostic factor
- Tumor budding (single cells/small clusters in stroma): Intermediate/high budding → worse OS and DFS
- Mucinous histology: Worse progression-free and overall survival
- Signet ring cell histology: Very poor prognosis (5-year survival 9-36%)
- BRAF V600E mutation: Poor prognosis in metastatic CRC
- KRAS mutation: Worse prognosis; resistance to anti-EGFR agents
- MSI-H/dMMR status: Better prognosis (15% improvement in survival vs MSS); excellent immunotherapy response
- Number of lymph nodes sampled: <12 nodes = inadequate staging; associated with worse outcomes
- Surgical margin status: Positive margins = high recurrence risk
10. SURVEILLANCE AFTER CURATIVE RESECTION
- Physical examination + CBC + LFTs + CEA: Every 3 months for first 2 years, then every 6 months to 5 years
- CEA every 3 months: Sensitive marker for detecting otherwise undetectable recurrence
- Colonoscopy: 1 year post-resection, then every 3 years (patients have 3-5% risk of second CRC and >15% risk of adenoma)
- CT chest/abdomen/pelvis: Semi-annually to annually for first 3 postoperative years
- Circulating tumor DNA (ctDNA): Under investigation as biomarker for residual/recurrent disease
- Most recurrences occur within first 2 years after surgery
11. SCREENING (for at-risk individuals)
Per USPSTF and American College of Gastroenterology (all average-risk adults aged 45-75):
- Colonoscopy every 10 years
- FIT every 1 year
- Stool DNA-FIT every 1-3 years
- CT colonography every 5 years
- Flexible sigmoidoscopy every 5 years ± annual FIT
- Any positive non-invasive test → diagnostic colonoscopy
For Lynch syndrome: Colonoscopy every 1-2 years starting at age 20-25.
For FAP: Flexible sigmoidoscopy annually from age 10-15 + APC genetic testing; colectomy once polyps develop.
12. SPECIAL SITUATIONS
Obstructing Sigmoid Cancer (Surgical Emergency)
Complicates 8-29% of CRC. Acutely: obstipation, abdominal distension, pain, feculent vomiting. Options:
- Emergency segmental resection ± primary anastomosis (if stable)
- Hartmann's procedure (resection + colostomy)
- Endoscopic stent as bridge to elective surgery (preferred where available)
Perforated Sigmoid Cancer
Surgical emergency: peritonitis, sepsis. Requires urgent laparotomy, resection, and usually Hartmann's procedure.
Recurrent CRC
20-40% of patients develop recurrence after curative surgery; most within 2 years. Isolated local abdominal recurrence or liver/lung metastasis may be resectable with intent to cure. Salvage surgery after imaging (CT + PET) to exclude other metastases is appropriate in selected patients.
Sources:
- Sabiston Textbook of Surgery, 21st Ed. - Colorectal Cancer Genetics, Surgical Anatomy, Adjuvant Therapy sections
- Schwartz's Principles of Surgery, 11th Ed. - TNM staging, Inherited CRC, Recurrence treatment
- Harrison's Principles of Internal Medicine, 22nd Ed. - Localized colon cancer management, surveillance
- The Washington Manual of Medical Therapeutics - Epidemiology, staging, treatment overview
- Bailey and Love's Short Practice of Surgery, 28th Ed. - Molecular analysis in CRC
- Fischer's Mastery of Surgery, 8th Ed. - Etiology and pathophysiology
- Meta-analysis on IMA ligation level in sigmoid/rectal cancer surgery (BMC Cancer, 2025) - PMID 41063015
This is a shared conversation. Sign in to Orris to start your own chat.