I now have all textbook content and all three intraoperative TRAP approach images. Here is the full surgical video script:
🎬 SURGICAL VIDEO SCRIPT
TRAP Approach (Triceps-Reflecting Anconeus Pedicle) for Distal Humerus Fracture ORIF
A Step-by-Step Operative Guide
Described by: O'Driscoll
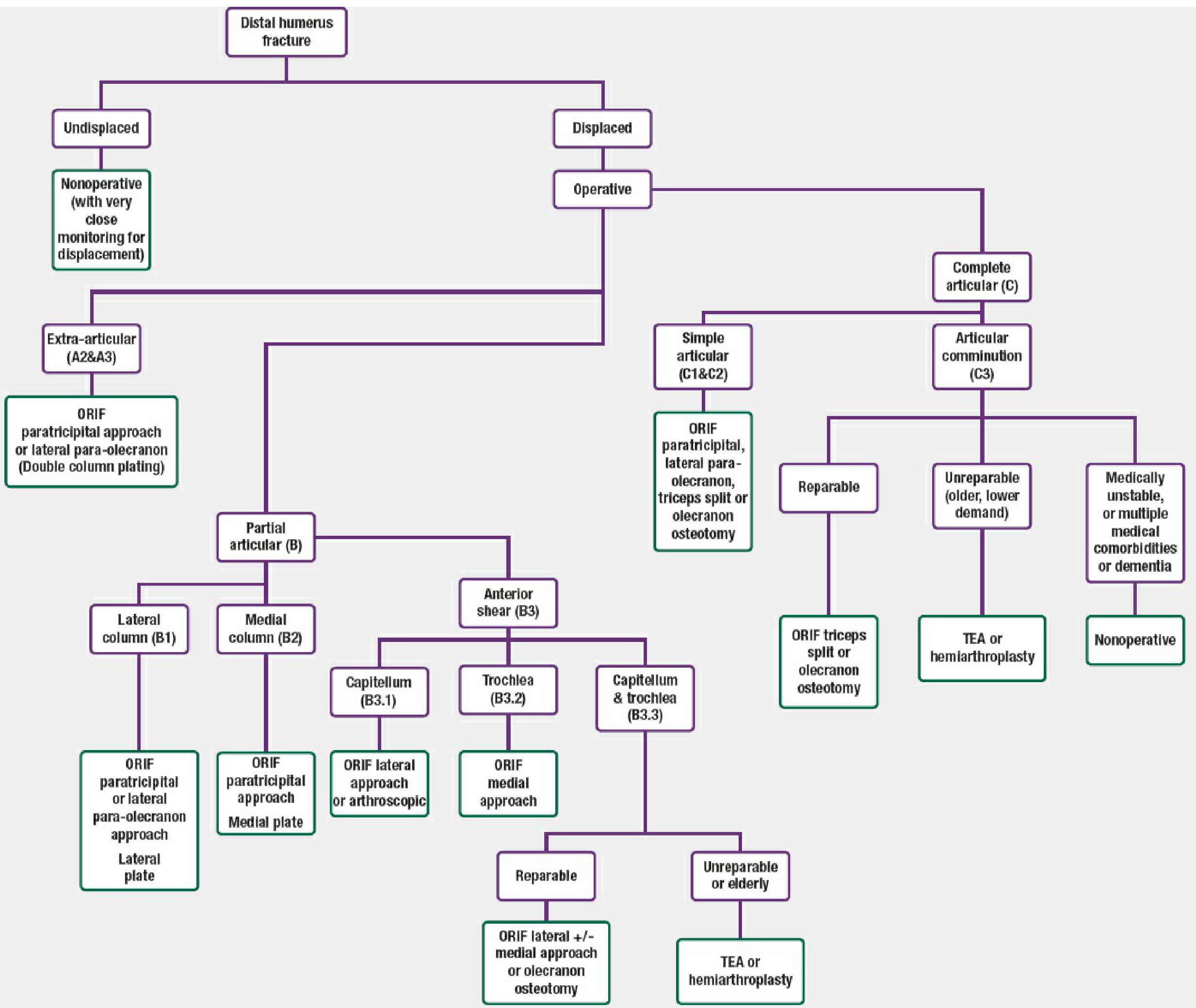
Indication: OTA/AO type C (complete articular) distal humerus fractures; complex intra-articular patterns; cases where olecranon osteotomy complications must be avoided
Key principle: Triceps and anconeus are reflected proximally together as a single vascularized pedicle flap, preserving the anconeus neurovascular supply while achieving wide posterior joint exposure
Based on: Rockwood & Green's Fractures in Adults (10th Ed, 2025) | Campbell's Operative Orthopaedics (15th Ed, 2026)
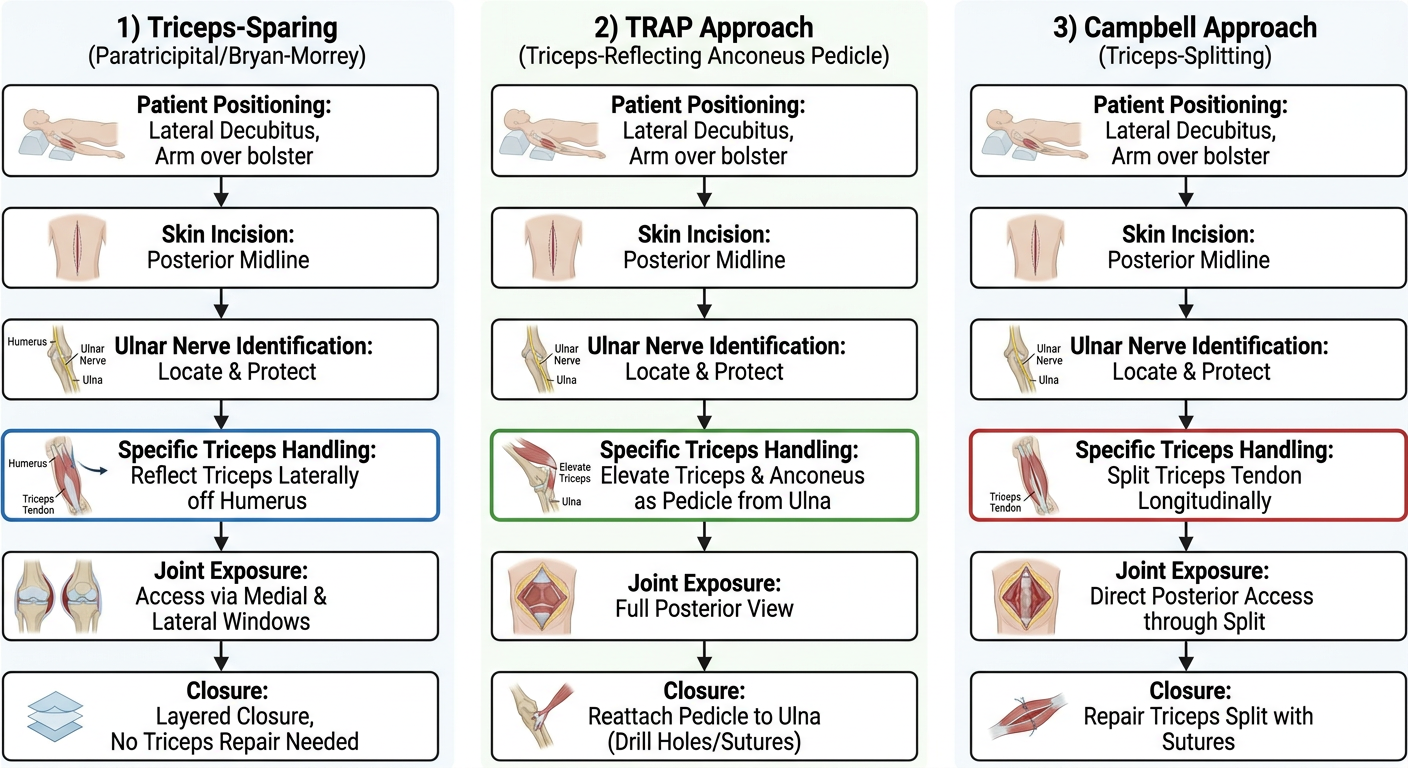
WHY THE TRAP APPROACH?
| Feature | Paratricipital | TRAP | Olecranon Osteotomy |
|---|
| Articular exposure | Limited | Good - full posterior joint | Best (58% articular surface) |
| Triceps status | Intact | Reflected off ulna | Intact (osteotomy not triceps) |
| Olecranon osteotomy | None | None | Required |
| Trochlear sulcus visible | No | Yes - used as reduction template | Yes |
| Early motion | Yes | Restricted (6 weeks) | Restricted (osteotomy healing) |
| Osteotomy complications | None | None | Nonunion, hardware pain (27%) |
| Best for | A2/A3, B1/B2, C1/C2 | C2/C3 ORIF, complex articular | C3, maximum articular exposure |
SCENE 1 - PREOPERATIVE SETUP & CHECKLIST
[VIDEO CUE: Overhead OR shot]
Indications for the TRAP Approach
- Intra-articular distal humerus fractures with moderate-to-high articular comminution where direct trochlear visualization is needed
- Cases where the surgeon wishes to avoid olecranon osteotomy complications (nonunion, hardware, ulnar nerve neuritis - reported at 33% in osteotomy series)
- Complex articular fractures where the trochlear sulcus is needed as a reduction template
- Intraoperative conversion from ORIF to TEA remains possible through the same exposure
Preoperative Checklist
| Item | Detail |
|---|
| Imaging | AP + lateral elbow XR; CT scan with 3D reconstructions mandatory for C-type fractures |
| Templating | Bicolumnar locking plates (parallel and orthogonal systems), headless compression screws, mini-fragment set |
| Antibiotics | IV cephalosporin 30 min before tourniquet |
| Tourniquet | Sterile pneumatic tourniquet to arm |
| Neuro baseline | Document ulnar nerve (little finger sensation, intrinsic power) and radial nerve (wrist/finger extension) |
| Contingency | Have olecranon osteotomy instruments available if further exposure needed |
⚠️ Important: Pre-brief the team that this approach involves complete triceps detachment. Postoperative extension restriction will be in place for 6 weeks. All team members should be aware.
SCENE 2 - PATIENT POSITIONING
[VIDEO CUE: Patient being positioned]
NARRATOR: "The TRAP approach is most commonly performed in the lateral decubitus position, though supine with a chest bolster is equally acceptable."
Preferred - Lateral Decubitus:
- Patient in lateral decubitus on a bean bag or padded support
- Operative arm draped free over an arthroscopy arm positioner or padded support, elbow flexed approximately 90°
- Arm positioned so elbow hangs free, allowing gravity-assisted retraction during the approach
- Tourniquet on the upper arm, sterile field from mid-arm distally
- Surgeon stands posterior to the patient; assistant on the opposite side
Alternative - Supine:
- Bolster under ipsilateral scapula
- Elbow rests on a folded sterile sheet on the patient's chest
🎯 Tip: The lateral decubitus position allows the arm to be repositioned (pronated/supinated, flexed/extended) freely during different phases - essential for visualizing anterior articular fragments via internal rotation of column fragments.
SCENE 3 - SKIN INCISION
[VIDEO CUE: Posterior elbow marked with pen]
NARRATOR: "The posterior midline incision is identical to all posterior elbow approaches."
Steps:
3.1 Mark bony landmarks with a marking pen:
- Tip of the olecranon
- Medial epicondyle
- Lateral epicondyle
3.2 Plan a posterior midline longitudinal incision:
- Begin 10-12 cm proximal to the olecranon tip, in the posterior midline of the arm
- Curve slightly medial to the olecranon tip (avoids direct pressure over the incision post-op)
- Extend distally 6-8 cm along the subcutaneous border of the ulna (this distal extension is important for the TRAP - you need access along the full length of the ulnar border)
3.3 Infiltrate subcutaneous tissue with 1:200,000 adrenaline solution to minimize bleeding.
3.4 Incise skin with a #10 blade to subcutaneous fat in a single pass.
3.5 Raise full-thickness fasciocutaneous flaps medially and laterally:
- Maintain the plane immediately on the deep fascia
- Thick flaps protect the subdermal plexus and reduce wound healing complications
- Expose the olecranon, medial epicondyle, and lateral epicondyle fully
⚠️ Hazard: The medial antebrachial cutaneous nerve branches cross the medial flap distally. Protect them during flap elevation to avoid dysesthesia.
SCENE 4 - ULNAR NERVE IDENTIFICATION AND TRANSPOSITION
[VIDEO CUE: Medial side of elbow, forceps lifting the nerve]
NARRATOR: "Ulnar nerve identification is the first and most critical step before any further dissection. It must be protected at every subsequent stage."
Steps:
4.1 Palpate the medial epicondyle and cubital tunnel retinaculum (Osborne's ligament).
4.2 Incise the cubital tunnel retinaculum longitudinally with scissors.
4.3 Identify the ulnar nerve in its groove immediately posterior to the medial epicondyle.
- Bluish-white cord, approximately 4-5 mm diameter
- First branch (to FCU) exits ~3 cm distal to the epicondyle
4.4 Pass a vessel loop (yellow) around the nerve immediately.
4.5 Mobilize the nerve proximally - release the medial intermuscular septum for 5-6 cm into the arm using scissors (this septum must be excised during the medial dissection anyway and releasing it now protects the nerve).
4.6 Mobilize the nerve distally into the forearm - release the FCU fascial roof for 3-4 cm. Identify but preserve the first motor branch to FCU.
4.7 Transpose the ulnar nerve anteriorly subcutaneous and secure with a loose suture to the anterior flap. The vessel loop remains visible throughout.
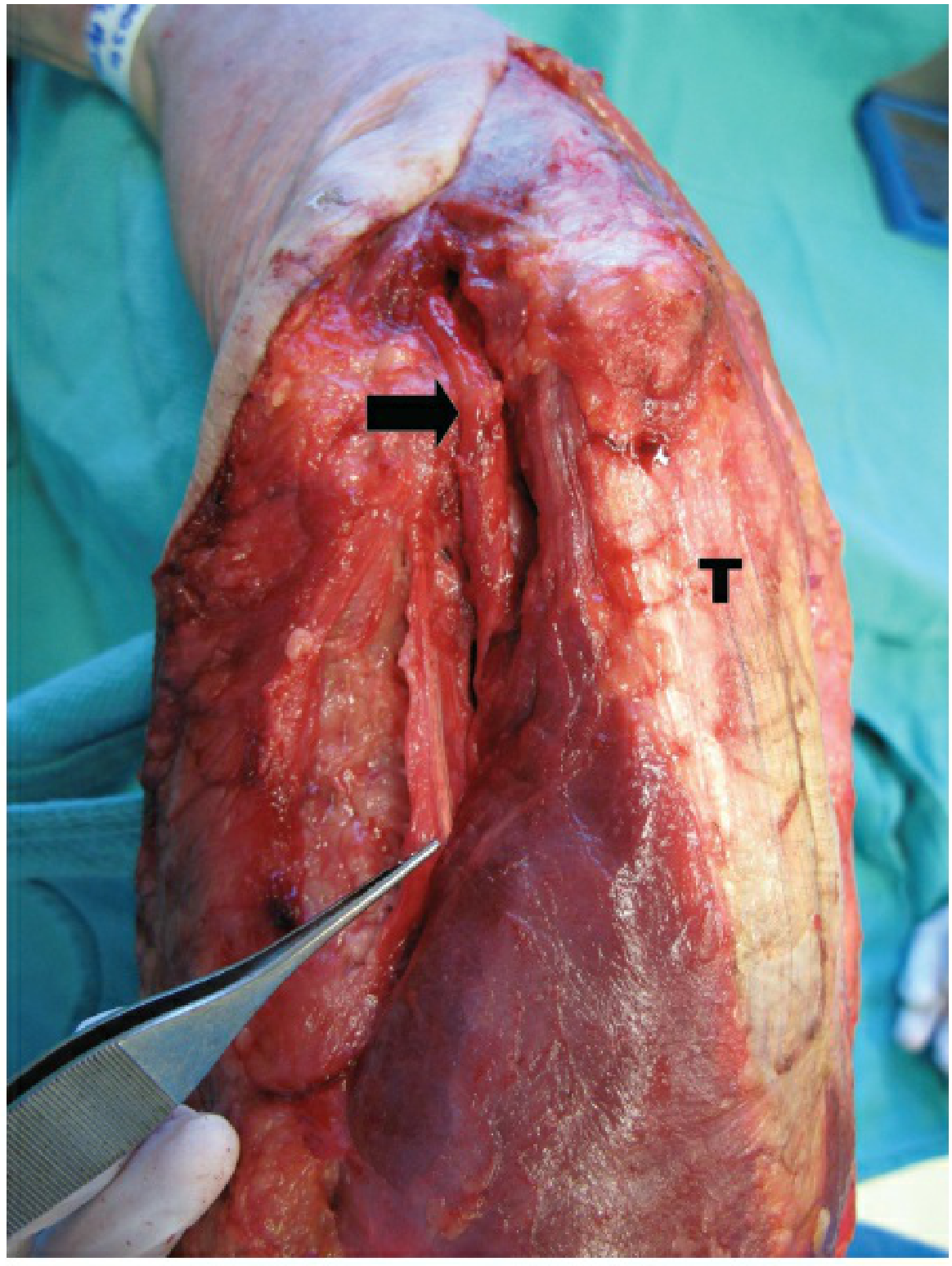
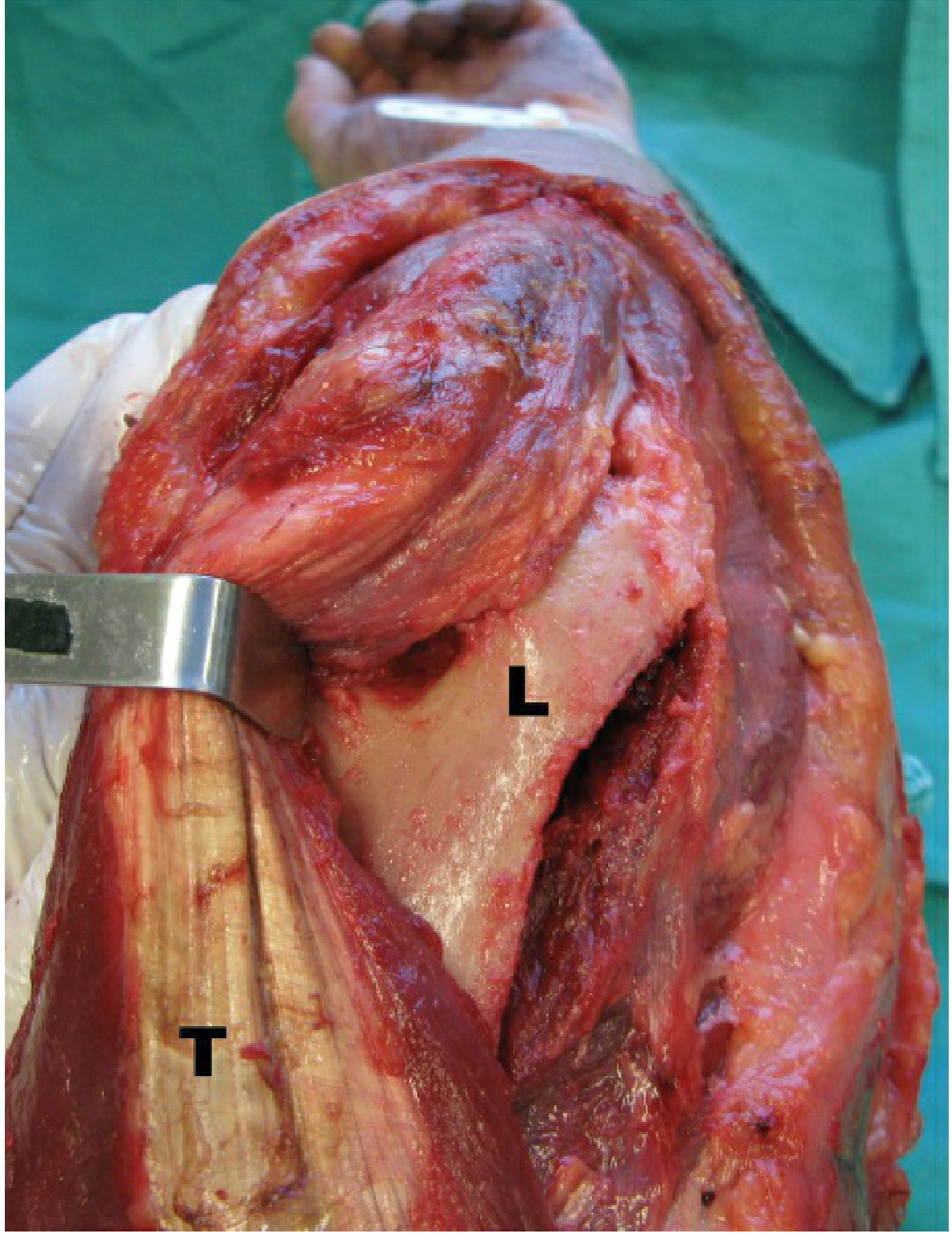
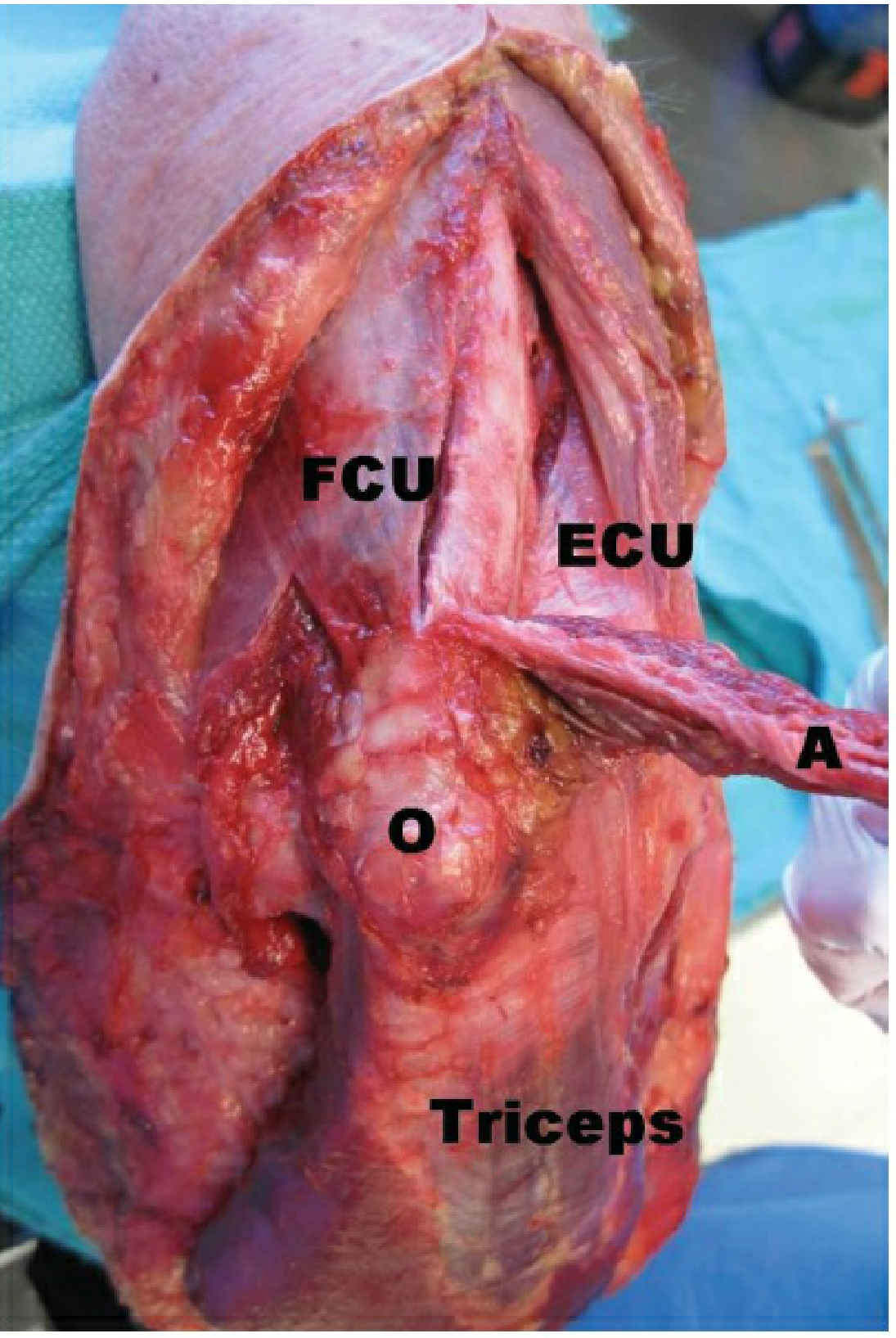
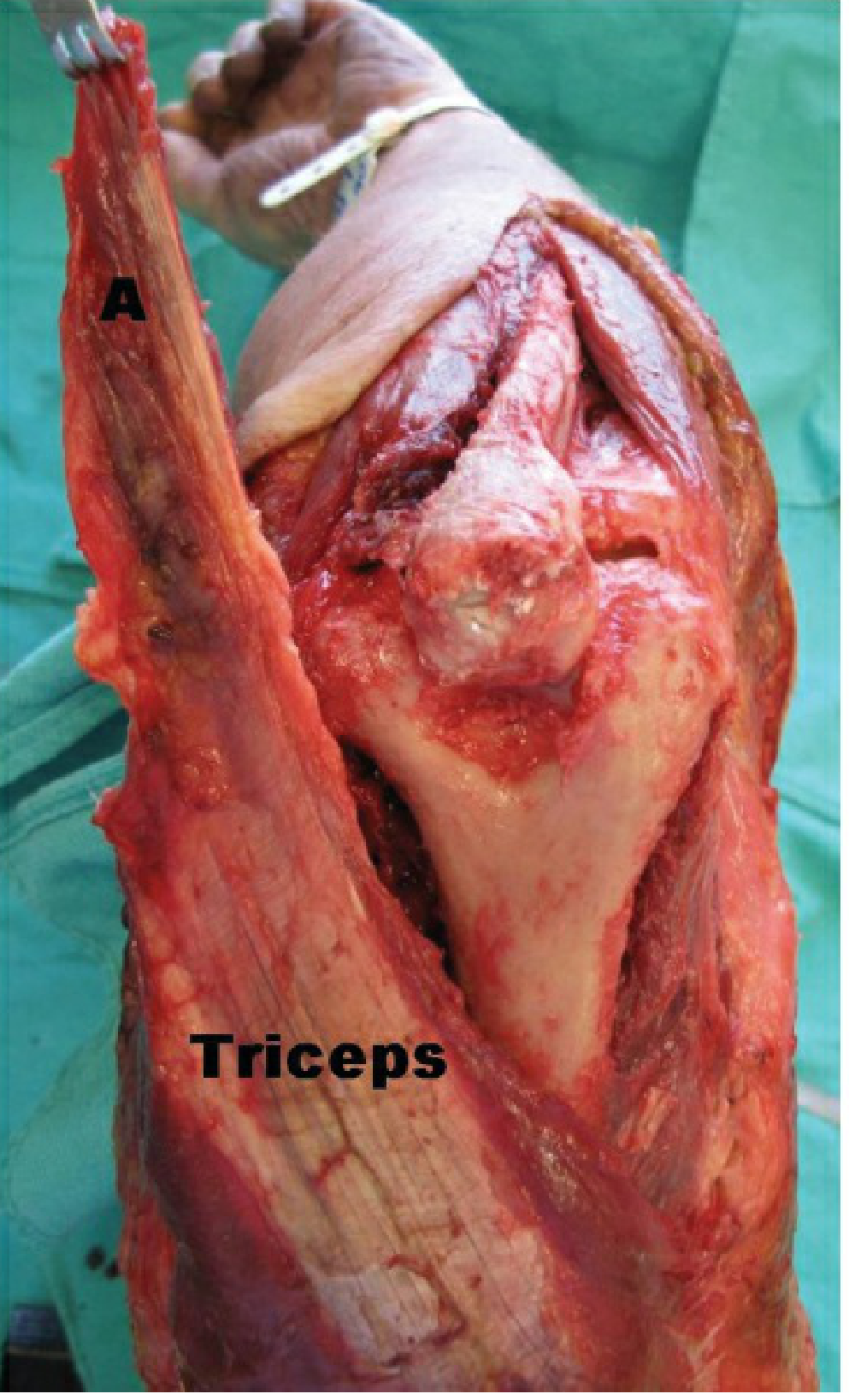
Fig 39-22A: TRAP approach - lateral side. Kocher interval used to elevate anconeus (A). O = olecranon tip. FCU = flexor carpi ulnaris (medial side visible). ECU = extensor carpi ulnaris (lateral). Triceps = distal muscle belly. (Rockwood & Green's, 10th Ed)
⚠️ Critical: Ulnar nerve neuritis was reported in 0% of TRAP/triceps-tongue cases vs 33% in olecranon osteotomy cases. The TRAP approach's zero neuritis rate depends on meticulous nerve handling.
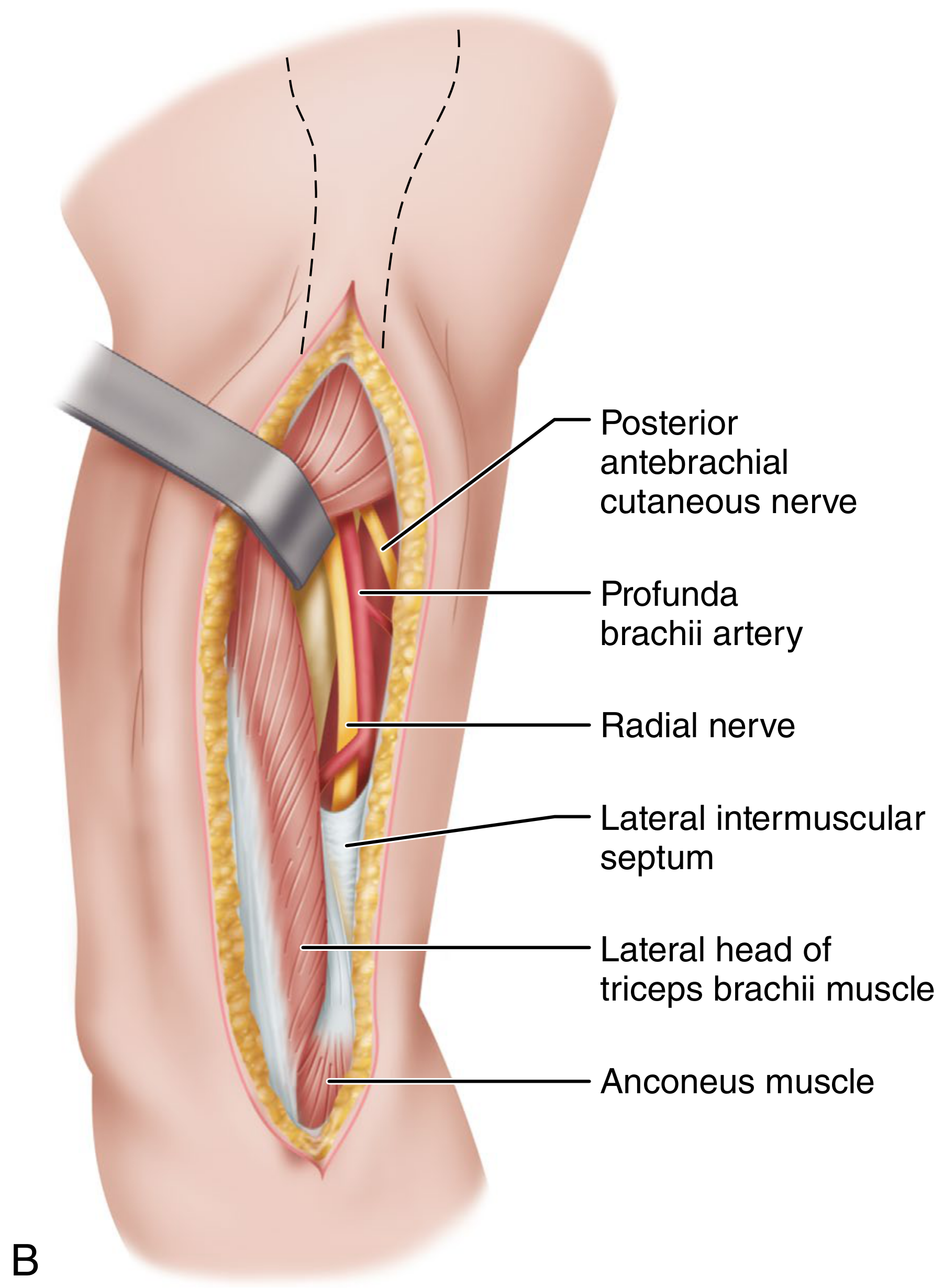
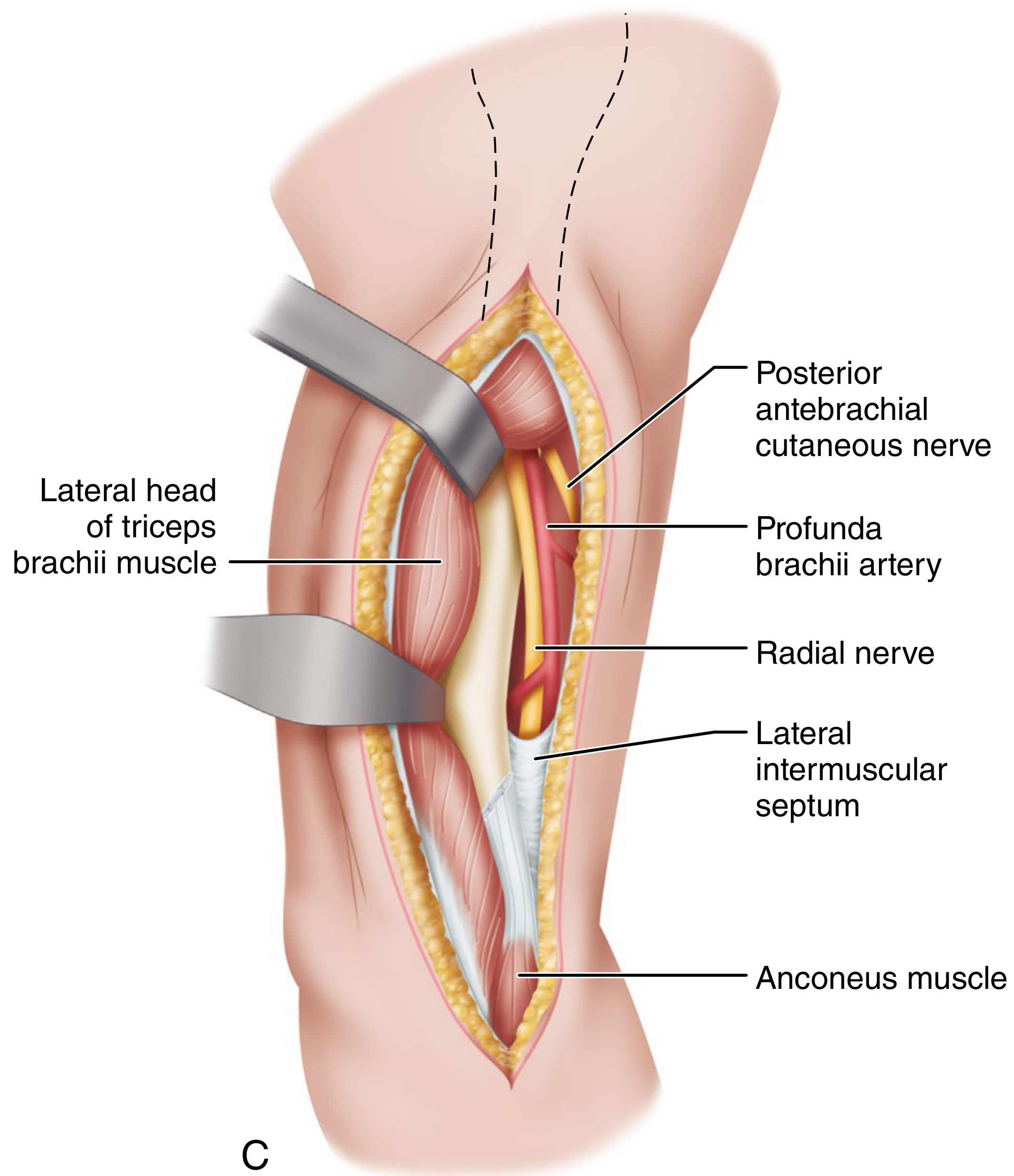
SCENE 5 - LATERAL FLAP: KOCHER INTERVAL AND ANCONEUS ELEVATION
[VIDEO CUE: Lateral elbow, surgeon working Kocher interval]
NARRATOR: "The TRAP flap is built from the lateral side first using the Kocher interval. This is the foundation of the entire approach."
Understanding the Key Anatomy First:
- Kocher interval = the surgical plane between ECU (extensor carpi ulnaris) and anconeus
- The interval is marked by a thin fat stripe running longitudinally, or by the perforating branches of the recurrent posterior interosseous artery
- The anconeus originates from the lateral epicondyle and inserts broadly on the posterior ulna
- The anconeus receives its nerve supply (branch of radial nerve) proximally - therefore, reflecting it distally-to-proximally is safe and preserves innervation
Steps:
5.1 Identify the Kocher interval on the lateral side of the elbow:
- Palpate the lateral epicondyle
- The interval runs from the lateral epicondyle distally along the posterior-lateral forearm
- Look for the thin fat stripe between ECU (anterior) and anconeus (posterior)
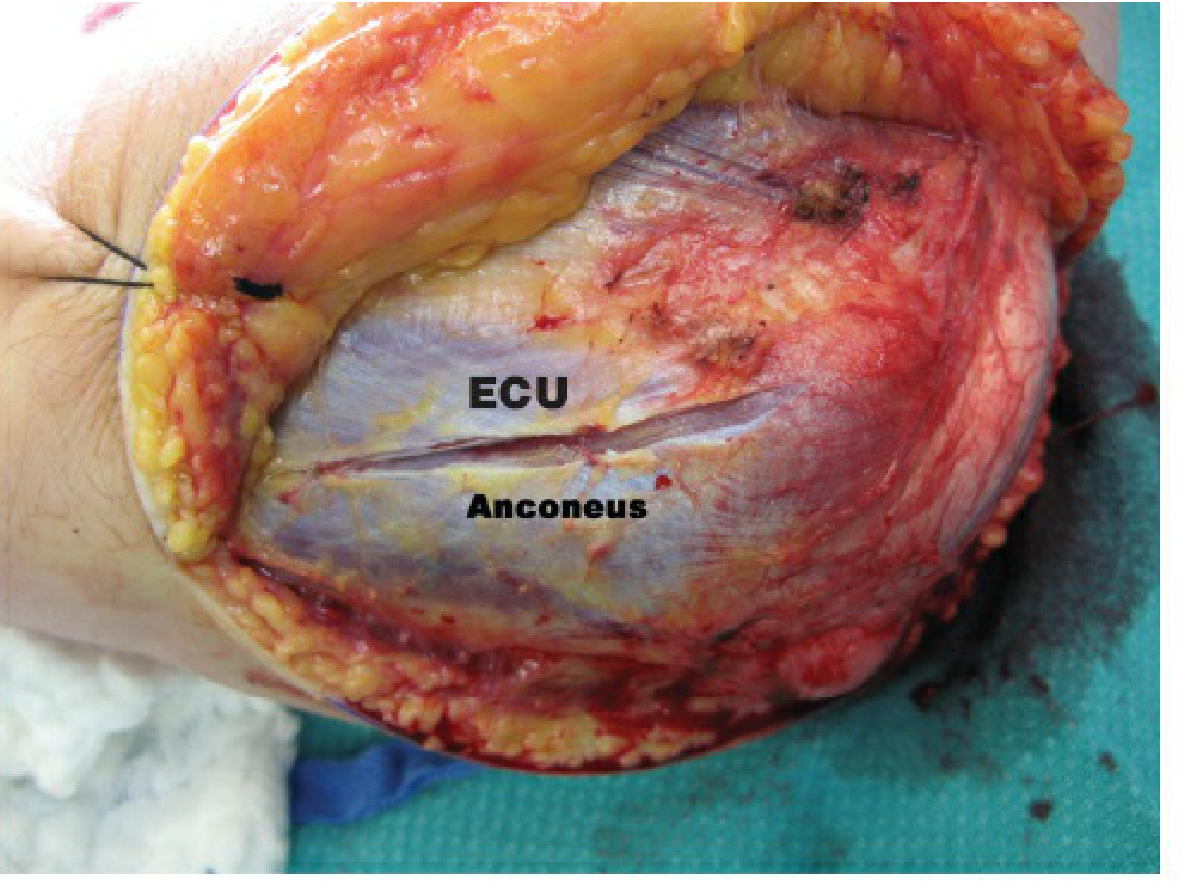
Fig 39-23B: ECU and anconeus labeled. The Kocher interval lies between these two muscles. (Rockwood & Green's, 10th Ed)
5.2 Incise the fascia in the Kocher interval with scissors from the lateral epicondyle distally along the lateral ulna.
5.3 Develop the interval by bluntly undermining the anconeus using scissors and a periosteal elevator - this exposes the elbow joint capsule and the lateral ulnar collateral ligament (LUCL) beneath.
⚠️ Hazard: The posterior interosseous nerve (PIN) lies at risk if the interval is extended distally below the radial neck. Pronate the forearm during distal extension - this moves the PIN anteriorly and increases the safe working distance.
5.4 Elevate the anconeus off the lateral epicondyle and posterior lateral humerus subperiosteally using a periosteal elevator. Work from distal to proximal.
5.5 Continue subperiosteal elevation to free the anconeus from the lateral border and posterior surface of the ulna (distal-to-proximal direction).
5.6 The anconeus is now mobilized as the distal lateral portion of the TRAP flap. It is reflected proximally toward the olecranon, tethered at its origin from the lateral epicondyle.
SCENE 6 - MEDIAL FLAP: SUBPERIOSTEAL DISSECTION FROM THE ULNAR BORDER
[VIDEO CUE: Medial side, periosteal elevator on subcutaneous ulna border]
NARRATOR: "We now develop the medial portion of the combined triceps-anconeus flap by stripping the triceps and soft tissues off the medial ulna subperiosteally."
Steps:
6.1 On the medial side, identify the subcutaneous border of the ulna (the palpable sharp ridge running from olecranon to the ulnar styloid).
6.2 Incise the periosteum and triceps attachment along the medial ulnar border with a scalpel, starting 4-5 cm distal to the olecranon tip and working proximally.
6.3 Elevate the periosteum and overlying soft tissues off the medial ulna using a periosteal elevator, working in a subperiosteal plane from medial-to-lateral across the posterior ulna.
6.4 Continue the subperiosteal elevation across the posterior surface of the proximal ulna toward the midline.
6.5 Connect the medial dissection to the lateral (Kocher) dissection across the posterior ulna - the two planes now meet in the midline of the posterior ulna.
🎯 Tip: Keep the dissection strictly subperiosteal throughout. Staying on bone avoids injury to the ulnar nerve (medially) and PIN (laterally), and keeps the flap vascular.
SCENE 7 - REFLECTING THE TRICEPS-ANCONEUS FLAP PROXIMALLY
[VIDEO CUE: The critical moment - flap reflected en bloc upward]
NARRATOR: "The anconeus flap is now reflected proximally. This exposes the triceps insertion on the olecranon, which is then sharply released. The entire triceps-anconeus unit is lifted off the elbow joint."
Steps:
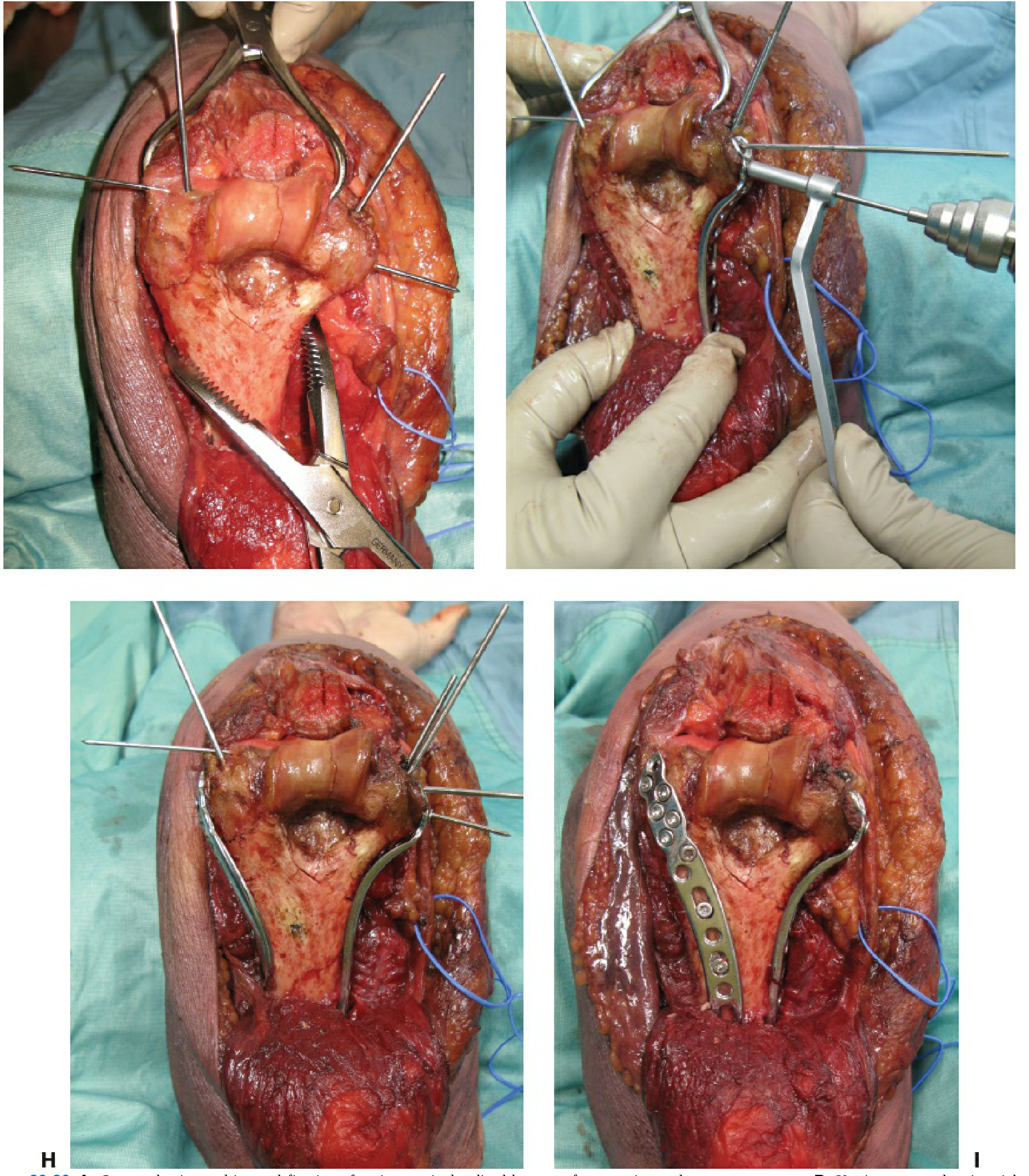
7.1 With the medial and lateral flap components mobilized and connected, reflect the combined anconeus + proximal ulnar periosteum flap proximally toward the olecranon. The olecranon tip is now exposed.
7.2 The triceps insertion on the olecranon tip is now visible from below/laterally.
7.3 Sharply release the triceps tendon insertion from the olecranon with a scalpel or electrocautery, cutting directly off the bone:
- Keep the release as close to bone as possible to preserve maximum tendon length for later reattachment
- Release proceeds from lateral to medial across the entire olecranon footprint
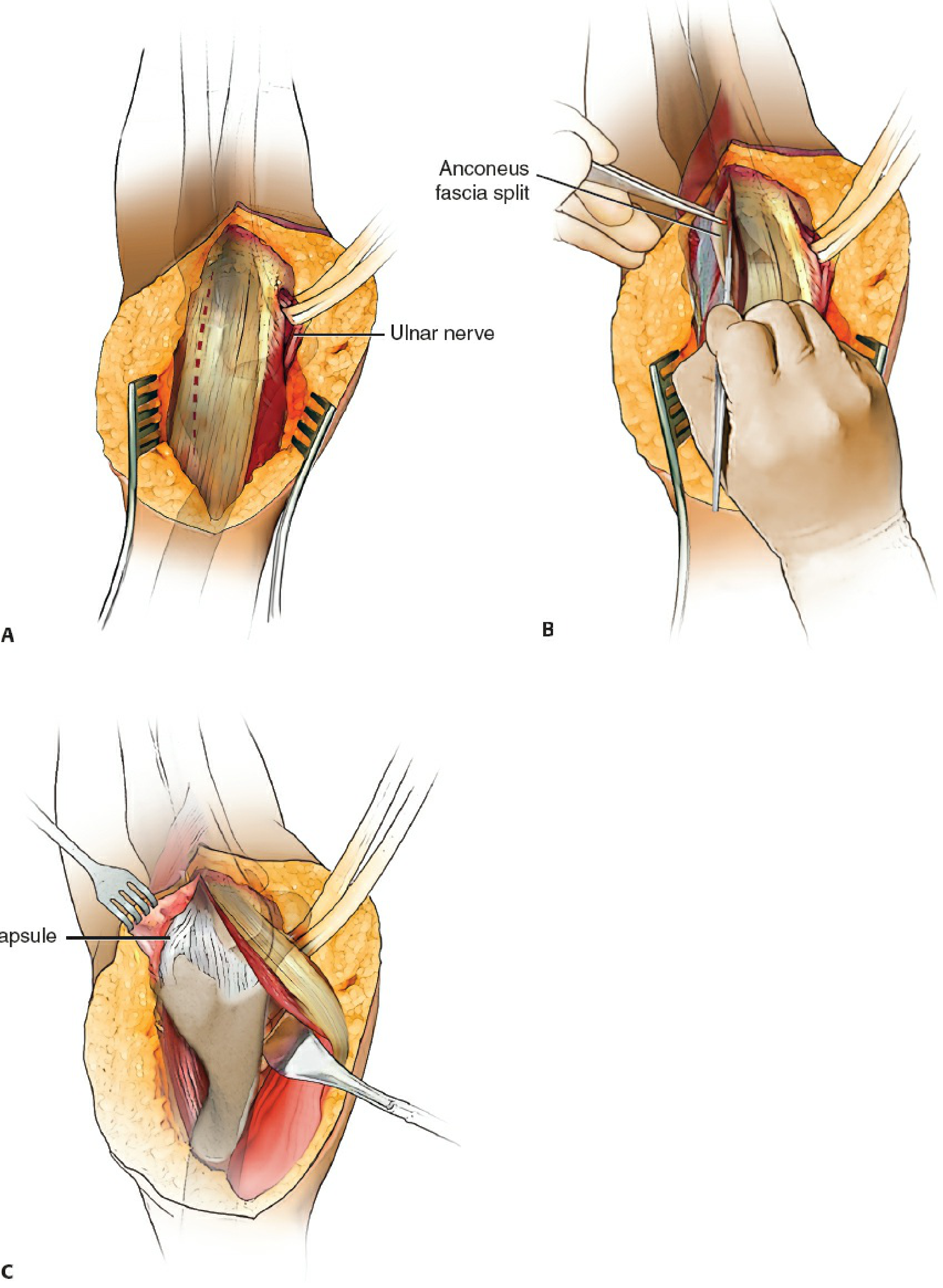
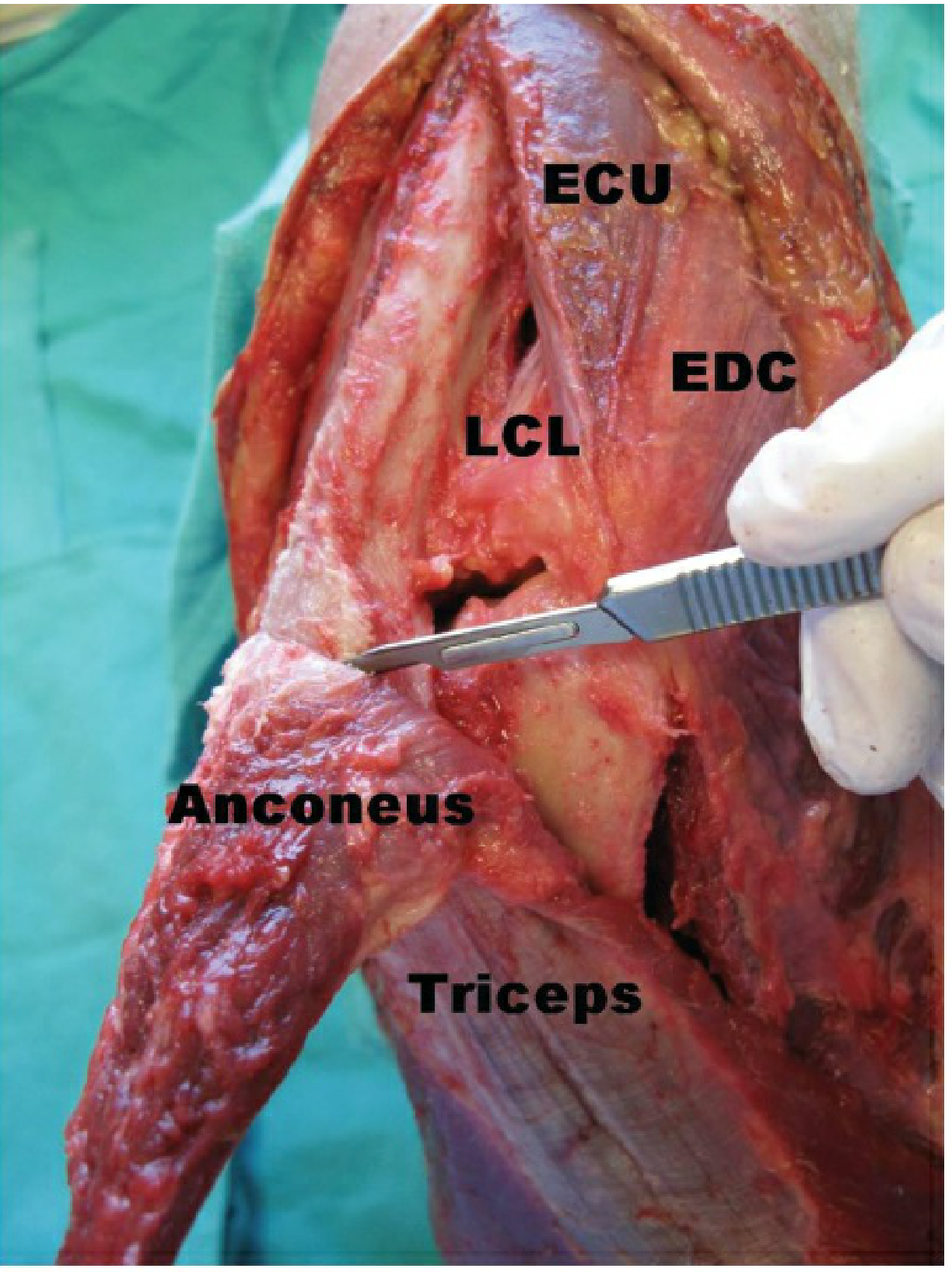
Fig 39-22B: Triceps insertion being sharply released from olecranon. Anconeus (A) and triceps both visible. LCL = lateral collateral ligament; ECU = extensor carpi ulnaris; EDC = extensor digitorum communis. (Rockwood & Green's, 10th Ed)
7.4 Continue to elevate the triceps muscle off the posterior surface of the distal humerus using a periosteal elevator, working proximally along the posterior shaft.
7.5 The entire triceps-anconeus unit is now reflected proximally, hinged at the proximal triceps musculotendinous junction. Hold it with a moist gauze and a proximal retractor.
7.6 The posterior elbow joint is now fully exposed:
- Entire olecranon fossa
- Both medial and lateral columns
- Trochlear sulcus (key articular landmark - used as reduction template)
- Posterior capitellum
- Posterior trochlea
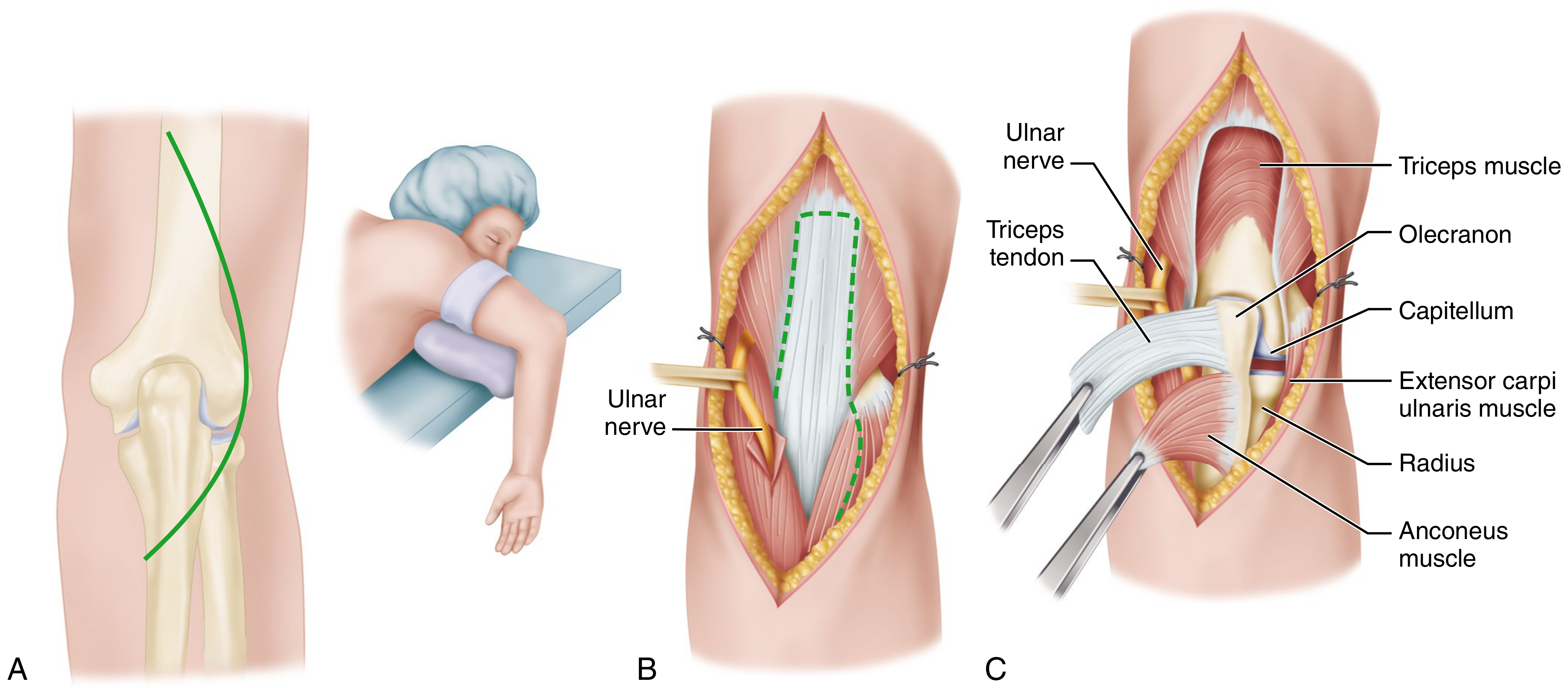
Fig 39-22C: Complete TRAP flap reflected. A = anconeus. Triceps = reflected proximal muscle belly. Full posterior elbow joint exposure achieved. (Rockwood & Green's, 10th Ed)
🎯 The Signature Advantage: The trochlear sulcus is now directly visible and can be used as a template for articular reduction - a unique benefit of the TRAP approach not available with the paratricipital or triceps-splitting approaches.
⚠️ Hazard: Keep the vessel loop on the ulnar nerve visible at all times. With the entire posterior joint now open, it is easy to lose sight of the nerve especially when placing retractors medially.
SCENE 8 - FRACTURE ASSESSMENT, REDUCTION, AND FIXATION
[VIDEO CUE: Wide posterior joint exposure with fracture fragments visible]
NARRATOR: "With the entire posterior elbow visible, we systematically reduce and fix the articular fracture using the trochlear sulcus as our primary reference landmark."
Stage 8A - Fracture Inventory
8A.1 Irrigate thoroughly to remove hematoma and identify all fracture fragments.
8A.2 Map fracture anatomy against the preoperative CT:
- Identify the capitellar fragment (lateral)
- Identify the trochlear fragment(s) (medial)
- Identify any free osteochondral fragments
- Confirm the trochlear sulcus is identifiable - this is the central reference point
8A.3 Tag any small osteochondral fragments with a provisional suture or K-wire stub to prevent them being lost during the case.
Stage 8B - Articular Reconstruction: Trochlea-First Strategy
8B.1 Begin with the trochlear sulcus as the foundation of the reduction. It is the keystone of the distal humerus articular surface.
8B.2 Use 1.6 mm K-wires as joysticks to manipulate the trochlear and capitellar fragments.
8B.3 Reduce the capitellar and trochlear fragments together, restoring the spool-shaped articular block:
- The trochlear sulcus must be anatomically restored
- The capitellar articular surface must be flush with the lateral trochlear ridge
8B.4 Apply a large reduction tenaculum to compress the fragments, clamping across the condyles.
8B.5 Confirm provisional reduction fluoroscopically (AP and lateral).
8B.6 Provisionally fix with 1.6-2.0 mm K-wires passed across the articular block.
8B.7 Insert definitive articular screws (headless compression screws 3.0-4.0 mm, or small-diameter lag screws) along the capitellar-trochlear axis - lateral to medial, perpendicular to the fracture plane:
- Countersink screw heads to avoid articular prominence
- Confirm screw length on fluoroscopy (must not protrude beyond medial cortex)
8B.8 For small anterior osteochondral fragments: internally rotate the relevant column fragment to expose the anterior articular surface. Fix with headless compression screws, mini-plates, or bioabsorbable pins as appropriate.
Stage 8C - Column Fixation: Articular Segment to Shaft
NARRATOR: "The articular block is now reconstructed. We attach it to the humeral shaft with bicolumnar plating."
8C.1 Reduce the reconstructed articular block to the humeral shaft using long bicortical K-wires (2.0 mm) placed provisionally up each column.
8C.2 Confirm reduction fluoroscopically - AP and lateral.
8C.3 Apply anatomically precontoured bicolumnar plates:
Parallel plating technique (preferred):
- Medial column plate along the medial column
- Lateral column plate along the lateral column
- Plates sit roughly in the same coronal plane; distal screws from each plate interdigitate
Orthogonal plating technique (alternative):
- One plate on the posterior medial column
- One plate on the posterolateral column (90° to the first plate)
8C.4 Distal screw fixation principles:
- Insert as many screws as possible through both plates into the articular segment
- Screws should be as long as possible, spanning the full width of the articular segment
- Each screw should engage as many articular fragments as possible
- Avoid the olecranon fossa - screws through the fossa cause impingement and block full extension
8C.5 Shaft fixation:
- Insert the first diaphyseal screw eccentrically in the plate's shaft holes to compress the supracondylar fracture site
- Fill remaining shaft holes with locking or cortical screws
- Minimum 3 bicortical shaft screws each side above the fracture
8C.6 Final fluoroscopy: AP, lateral, and oblique views to confirm:
- Articular congruence
- Column reduction and alignment
- All screw lengths safe (no articular prominence, none through olecranon fossa)
- Carrying angle approximately correct
🎯 Tip: The TRAP approach allows the trochlear sulcus to guide articular reduction. Unlike the paratricipital approach where the articular surface is obscured by the intact triceps, here you can directly visualize and confirm articular congruence under direct vision before plating.
SCENE 9 - CHECK RANGE OF MOTION UNDER DIRECT VISION
[VIDEO CUE: Elbow moved through arc of motion]
NARRATOR: "Before closure, assess intraoperative range of motion and confirm no impingement."
9.1 With the tourniquet still inflated (or released), gently flex and extend the elbow.
- Normal flexion arc: 0-140° should be achievable
- Listen and feel for any crepitus or bony block
9.2 If impingement in extension is felt, examine the olecranon fossa fluoroscopically for:
- Screw in olecranon fossa (remove and replace)
- Residual small bony fragment in the fossa (remove)
- Olecranon tip overhang (partial tip excision)
9.3 Confirm stability: apply varus/valgus and posterolateral rotatory stress - fixation should be rigid.
SCENE 10 - WOUND CLOSURE
[VIDEO CUE: Final fixation confirmed, tourniquet released]
NARRATOR: "Closure of the TRAP approach requires secure reattachment of the triceps-anconeus flap to the olecranon. This is the most critical part of the closure."
Steps:
10.1 Release the tourniquet. Achieve hemostasis with bipolar electrocautery. Irrigate copiously (3L normal saline).
10.2 Remove all provisional K-wires not serving as final fixation.
10.3 Ulnar nerve final position:
- Confirm the ulnar nerve is positioned in the anterior subcutaneous transposition
- Secure the transposition with a loose Z-plasty fascial sling (2-0 Vicryl) - the sling must allow finger to pass under it without resistance
- Remove the vessel loop
10.4 TRICEPS-ANCONEUS FLAP REATTACHMENT - The critical step:
10.4a Drill 2-3 transosseous bone tunnels through the olecranon with a 2.0 mm drill:
- One tunnel on the medial side of the olecranon
- One tunnel on the lateral side
- Optional third tunnel in the middle
- Tunnel orientation: from posterior (dorsal) olecranon surface through to the anterior (articular) surface of the triceps footprint
10.4b Pass non-absorbable braided sutures (FiberWire #2 or equivalent) through the bone tunnels using a suture passer.
10.4c Pass the corresponding sutures through the triceps tendon in a locking Krackow or Bunnell configuration - capture maximum tendon.
10.4d With the elbow in full extension, tie the sutures firmly over the olecranon. Tension the repair with the elbow extended to maximize tendon purchase and prevent gap formation.
⚠️ Critical: Triceps dehiscence is the most feared complication of the TRAP approach. A weak or inadequate repair here directly leads to extensor mechanism failure. Use the strongest available suture; do not spare the number of passes.
10.4e Check repair integrity: hold the arm up with elbow extended and then flex it - the tendon repair should be visibly and palpably taut in extension.
10.5 Close the Kocher interval fascia with interrupted 0 Vicryl sutures - reapproximate the ECU/anconeus fascia.
10.6 Close the deep posterior fascia medially and laterally with interrupted absorbable sutures.
10.7 Place a surgical drain (optional, but recommended given the extensive dissection).
10.8 Subcutaneous layer: interrupted Vicryl 2-0.
10.9 Skin: interrupted nylon or staples.
10.10 Apply a padded posterior plaster splint with the elbow at 30-45° of flexion (not full extension) to reduce wound tension. This will be adjusted at the first dressing change.
SCENE 11 - POSTOPERATIVE PROTOCOL
[VIDEO CUE: Patient in recovery with arm splinted and elevated]
Key difference from paratricipital approach: Because the triceps was fully detached and reattached, elbow extension is restricted for 6 weeks to protect the triceps repair.
| Time Point | Protocol |
|---|
| Day 0-1 | Elevation at heart level. Ice. Check ulnar nerve (little finger sensation + adduction), radial nerve (finger/wrist extension). |
| Day 1-2 | Remove drain. Wound check. Active hand and wrist exercises immediately. |
| Week 1 | Convert splint to hinged elbow brace locked at 30-90° arc. Begin passive assisted flexion. No active extension. |
| Week 2 | Suture/staple removal. Increase flexion range passively. |
| Week 3-4 | Brace arc extended: 0-110° passively assisted. Gentle active-assisted flexion only. |
| Week 6 | Radiograph to confirm fracture healing and triceps attachment. Begin active elbow extension carefully if healed. Remove brace restriction. |
| Week 8-12 | Progressive resistive exercises. Functional activities. |
| 6 months | Return to full activity if healed. |
SCENE 12 - PITFALLS AND HOW TO AVOID THEM
| Pitfall | Mechanism | Prevention |
|---|
| Triceps dehiscence | Weak transosseous repair; early unrestricted motion | Krackow suture through bone tunnels; FiberWire #2; brace restricted to 6 weeks; counsel patient |
| Extensor mechanism weakness | Dehiscence, poor healing, premature loading | Protect repair; delay active extension to week 6 |
| Ulnar nerve injury | Traction during flap reflection; unrecognized during medial periosteal strip | Vessel loop always visible; transpose before starting the flap |
| PIN injury | Kocher interval taken too far distally | Pronate forearm when working distally; stay proximal to radial neck |
| Anconeus devascularization | Flap reflected distal-to-proximal (wrong direction) | Always reflect from distal-to-proximal; nerve and blood supply enter from proximal |
| Inadequate articular exposure | Flap not fully mobilized medially | Ensure full medial subperiosteal elevation before reflecting |
| Olecranon fossa screws | Misdirected distal plate screws | Pre-plan screw trajectories; lateral fluoroscopy before tightening |
| Intra-articular screw prominence | Articular screws too long | Measure depth; AP and oblique fluoroscopy |
| Wound necrosis | Thin flaps, excessive tension | Full-thickness fasciocutaneous flaps; splint at 30-45° not full extension |
| Stiffness | Delayed physiotherapy, inadequate bony fixation | Begin passive ROM week 1; active ROM week 6 |
COMPLETE SURGICAL CHECKLIST (Quick Reference Card)
PRE-OP
□ CT reviewed, fracture pattern mapped (AO/OTA type)
□ Trochlear sulcus identifiable on CT (landmark for reduction)
□ Bicolumnar plates templated; headless screw set available
□ Contingency plan if conversion to TEA needed
□ IV antibiotics before tourniquet inflation
□ Ulnar nerve baseline documented
POSITIONING
□ Lateral decubitus or supine with chest bolster
□ Arm draped free
□ Sterile tourniquet applied
APPROACH
□ Posterior midline incision - curves medial to olecranon tip
□ Extends distally 6-8 cm along subcutaneous ulnar border
□ Full-thickness fasciocutaneous flaps raised medially and laterally
□ Ulnar nerve identified, vessel-looped, anterior subcutaneous transposition
□ LATERAL: Kocher interval (ECU/anconeus) incised; anconeus elevated from lateral epicondyle and lateral ulna, distal-to-proximal
□ Forearm pronated during distal dissection (protects PIN)
□ MEDIAL: Periosteal elevation off medial ulnar border, medial-to-lateral across posterior ulna
□ Medial and lateral planes connected across posterior ulna
□ Anconeus flap reflected proximally → triceps insertion exposed
□ Triceps insertion sharply released from olecranon (close to bone)
□ Triceps muscle elevated subperiosteally off posterior distal humerus
□ Full posterior joint exposed; trochlear sulcus identified
REDUCTION & FIXATION
□ Fracture hematoma irrigated
□ All fragments inventoried vs. preop CT
□ Trochlear sulcus used as primary reduction reference
□ K-wire joysticks for fragment manipulation
□ Articular segment reduced and provisionally K-wired
□ Fluoroscopy confirms provisional reduction
□ Definitive articular screws (capitellar-trochlear axis)
□ Parallel or orthogonal bicolumnar plates applied
□ Maximum screws into articular segment
□ First diaphyseal screw eccentric (fracture compression)
□ No screws in olecranon fossa
□ Final AP + lateral + oblique fluoroscopy
□ Intraoperative ROM check - no impingement
CLOSURE
□ Tourniquet released; hemostasis; 3L irrigation
□ Ulnar nerve transposition secured (fascial sling, finger passes freely)
□ Vessel loop removed
□ Transosseous bone tunnels drilled in olecranon (2-3 tunnels)
□ Triceps reattached with FiberWire #2 Krackow through bone tunnels
□ Repair tensioned in full extension and tied
□ Repair integrity tested (flex/extend cycle under direct vision)
□ Kocher interval fascia closed
□ Deep fascia closed
□ Drain placed
□ Skin closed
□ Posterior splint at 30-45° flexion
POST-OP
□ Neurovascular check (ulnar nerve first)
□ Elevation and ice
□ Active hand/wrist exercises from day 1
□ Elbow extension restricted 6 weeks (hinged brace)
□ Active elbow extension begins week 6 (after radiograph)
TRAP vs PARATRICIPITAL - SIDE-BY-SIDE SUMMARY
| Step | Paratricipital | TRAP |
|---|
| Ulnar nerve | Anterior transposition | Anterior transposition |
| Triceps | Never touched - windows around it | Fully detached from olecranon |
| Anconeus | Elevated off lateral column only | Elevated from Kocher interval + reflected en bloc with triceps |
| Articular view | Columns + fossa (triceps obscures joint) | Full posterior joint + trochlear sulcus visible |
| Key reduction tool | Fluoroscopy | Direct trochlear sulcus visualization |
| Closure - triceps | No repair needed | Transosseous suture reattachment |
| Active extension | Day 1 | Week 6 |
| Brace requirement | None | Hinged brace 0-6 weeks |
| Dehiscence risk | None | Present - primary concern |