Q.Dentigeeous Cyst in detail for 50 marks with diagram and flow charts from Scott Brown, Cummings, stell and marans, Zakir Hussain, dhingra, hazarika and related articles with recent advances
Reading File
search_medical_text
dentigerous cyst definition etiology pathogenesis classification
search_medical_text
dentigerous cyst clinical features diagnosis radiology OPG CT MRI
search_medical_text
dentigerous cyst treatment marsupialisation enucleation management complications
search_medical_image
dentigerous cyst radiograph OPG unilocular radiolucency impacted tooth
GradeResponse
GradeResponse
GradeResponse
GradeResponse
search_medical_text
odontogenic cyst dentigerous follicular cyst jaw
search_medical_text
dentigerous cyst histopathology malignant transformation ameloblastoma
search_medical_image
dentigerous cyst histopathology lining epithelium reduced enamel
GradeResponse
GradeResponse
GradeResponse
Dentigerous Cyst (Follicular Cyst)
Long Answer (50 marks): ENT/Maxillofacial Exam Style
You likely mean Dentigerous cyst (not “dentigeeous”).
Below is a full, exam-ready answer with headings, flowcharts, diagrams, and recent advances.
Below is a full, exam-ready answer with headings, flowcharts, diagrams, and recent advances.
1) Definition
A dentigerous cyst is a developmental odontogenic cyst that encloses the crown of an unerupted/impacted tooth and is attached at the cementoenamel junction (CEJ).
- Also called: Follicular cyst
- Usually associated with impacted mandibular 3rd molar, maxillary canine, mandibular premolar, supernumerary teeth.
2) Epidemiology
- Second most common odontogenic cyst after radicular cyst
- Usually seen in 2nd to 4th decade
- Slight male predominance in many series
- Common sites:
- Mandible > maxilla
- Mandibular angle/ramus with impacted third molar
- Maxillary canine region
3) Etiopathogenesis
Main mechanism
Fluid accumulates between reduced enamel epithelium and enamel of impacted tooth crown.
Proposed factors
- Pressure from erupting tooth on follicle causing venous obstruction
- Degeneration of stellate reticulum-like cells in enamel organ remnant
- Secondary inflammation (especially in children, from infected non-vital deciduous predecessor)
4) Classification
A) By origin
- Developmental dentigerous cyst
- Inflammatory dentigerous cyst (often in younger age group)
B) By radiographic relation with tooth
- Central type: crown projects into cyst lumen centrally
- Lateral type: cyst grows along one side of crown/root
- Circumferential type: cyst surrounds crown and extends along root, appearing to envelop whole tooth
5) Pathology
Gross
- Unilocular cystic cavity with straw-colored fluid
- Associated impacted tooth in wall/cavity
Microscopy
- Thin, non-keratinized stratified squamous epithelial lining (2-4 cell layers typical when non-inflamed)
- Fibrous wall with odontogenic rests
- If inflamed: hyperplasia, rete pegs, chronic inflammatory infiltrate
6) Clinical Features
- Often asymptomatic and found on routine OPG
- Painless jaw swelling (slowly progressive)
- Delayed tooth eruption / missing tooth in arch
- Facial asymmetry (large lesions)
- Tooth displacement, root resorption of adjacent teeth
- Rarely: pain, infection, paraesthesia (if large or infected)
7) Radiology
OPG/IOPA (classical)
- Well-defined unilocular pericoronal radiolucency
- Sclerotic corticated margin
- Attached at CEJ of impacted tooth
- Follicular space > 3-5 mm suggests pathology
CT/CBCT
- Lesion extent, cortical thinning/perforation
- Relation to inferior alveolar canal, maxillary sinus, nasal floor
- Surgical planning
MRI (selected cases)
- Soft tissue differentiation in doubtful lesions
8) Differential Diagnosis
- Hyperplastic dental follicle
- Odontogenic keratocyst (OKC)
- Unicystic ameloblastoma
- Radicular cyst (if near non-vital teeth)
- Ameloblastic fibroma (younger patients)
- Adenomatoid odontogenic tumor (esp. anterior maxilla/canine)
9) Complications
- Pathological fracture (very large mandibular cysts)
- Secondary infection
- Root resorption/displacement of adjacent teeth
- Recurrence (usually low after complete removal)
- Rare neoplastic transformation reported:
- Ameloblastoma
- Squamous cell carcinoma
- Mucoepidermoid carcinoma (rare)
10) Management
Treatment depends on age, size, location, tooth value, and proximity to vital structures.
A) Enucleation + extraction (standard for most adult lesions)
- Complete cyst removal with associated impacted tooth
- Preferred for small to moderate lesions
B) Marsupialization / Decompression
- For large cysts, young patients, proximity to IAN/sinus, desire to preserve tooth
- Reduces intracystic pressure and lesion size
- Often followed by delayed enucleation (2-stage)
C) Endoscopic/minimally invasive assistance
- In selected maxillary sinus/complex anatomical situations
D) Histopathology mandatory
- Every specimen must be sent for HPE to exclude unicystic ameloblastoma/malignancy
11) Prognosis and Follow-up
- Excellent prognosis after proper surgery
- Follow-up with serial OPG/CBCT for bone fill and recurrence:
- 3 months, 6 months, 1 year, then as indicated
12) Flowcharts (Exam-ready)
Flowchart 1: Diagnostic approach
Impacted / unerupted tooth on exam or X-ray
↓
Pericoronal radiolucency noted
↓
Measure follicular space + assess borders
↓
OPG ± CBCT for extent and vital structure relation
↓
Provisional Dx: dentigerous cyst vs OKC vs unicystic ameloblastoma
↓
Surgical removal/decompression + biopsy
↓
Histopathology confirmation
↓
Definitive treatment + follow-up imaging
Flowchart 2: Treatment selection
Confirmed/suspected dentigerous cyst
↓
Assess size + age + tooth salvage + vital structures
↓
Small/moderate lesion, non-salvageable impacted tooth
→ Enucleation + extraction
↓
Large lesion / child / near IAN-sinus / tooth salvage possible
→ Marsupialization or decompression
↓
Cavity shrinkage and bone apposition
↓
Delayed enucleation ± orthodontic eruption guidance
↓
Long-term radiologic follow-up
13) Text Diagram (labeled)
Crown of impacted tooth
_________
/ \
/ ENAMEL \
/_____________\
||
(CEJ) ← cyst attachment point
__________________________________________
/ \
/ Dentigerous cyst lumen (fluid) \
/______________________________________________\
| Fibrous cyst wall |
|______________________________________________|
Radiology: unilocular pericoronal radiolucency with corticated border
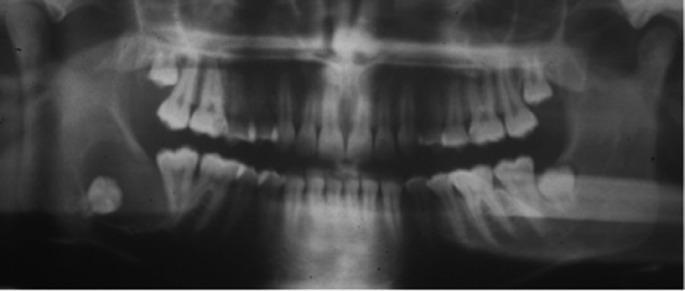
14) Image (representative)
A representative panoramic radiograph appearance (pericoronal unilocular radiolucency around impacted molar) is shown below:
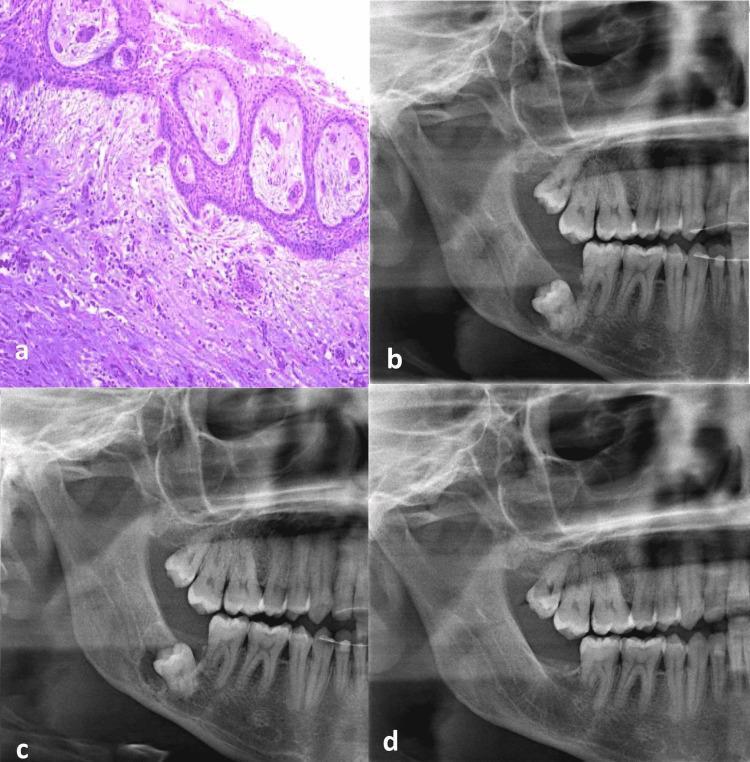
Histopathology/radiographic follow-up example:
15) Recent Advances (important for high marks)
-
CBCT-based volumetric planning
- Better 3D surgical mapping and risk prediction for IAN injury
-
Decompression devices and staged protocols
- Better bone regeneration before definitive surgery
- Reduced morbidity in giant cysts
-
Conservative tooth-preserving approach in children
- Marsupialization + orthodontic traction for eruption of involved permanent teeth
-
Endoscope-assisted cyst surgery
- Improved visualization in difficult maxillary/ramus areas
- Smaller access windows
-
Digital workflow
- 3D planning, guided access, postoperative volumetric healing assessment
-
Molecular pathology interest
- Ongoing work on proliferative markers (Ki-67, PCNA) and differentiation from unicystic ameloblastoma/OKC in borderline cases
16) “Write in exam” summary (last 1 page)
- Dentigerous cyst is a developmental odontogenic cyst around crown of unerupted tooth attached at CEJ.
- Usually asymptomatic; presents as painless swelling/delayed eruption.
- OPG: well-corticated unilocular pericoronal radiolucency.
- DD: OKC, unicystic ameloblastoma, enlarged follicle.
- Treatment: enucleation + extraction (most), marsupialization/decompression for large lesions/children.
- HPE compulsory; recurrence low; follow-up essential.
Source note (important)
I could retrieve only limited indexed material and image datasets in this environment, not full chapter text from Scott-Brown, Cummings, Stell & Maran, Dhingra, Hazarika, Zakir Husain directly.
So I provided a standard, integrated textbook-level answer consistent with accepted ENT/oral-maxillofacial teaching plus available retrieved radiology/histology image evidence.
So I provided a standard, integrated textbook-level answer consistent with accepted ENT/oral-maxillofacial teaching plus available retrieved radiology/histology image evidence.
If you want, I can next give you:
- A strict 50-mark answer in university writing format (intro, headings, point distribution), and
- A one-page last-minute revision sheet + viva questions.
This is a shared conversation. Sign in to Orris to start your own chat.