define CIN write down management of different types of CIN and precancerous intra epithelial lesion of cervix from berek and novak with diagrams flowcharts with proper and easy explanation 10 mark answer for M.S main exam
CIN (Cervical Intraepithelial Neoplasia) - Comprehensive 10-Mark Answer
Based on Berek & Novak's Gynecology
DEFINITION
- Cellular immaturity
- Cellular disorganization
- Nuclear abnormality (enlargement, hyperchromasia, irregular nuclear membranes)
- Increased mitotic activity
"The extent of the mitotic activity, immature cellular proliferation, and nuclear atypia identifies the degree of neoplasia." - Berek & Novak
CLASSIFICATION / GRADING
┌─────────────────────────────────────────────────────────────────┐
│ EPITHELIAL THICKNESS (Basal → Surface) │
│ │
│ CIN 1 │▓▓░░░░░░░░░░│ Mitoses + immature cells = LOWER 1/3 │
│ (LSIL) │ │ 60-85% SPONTANEOUS REGRESSION │
│─────────────────────────────────────────────────────────────────│
│ CIN 2 │▓▓▓▓▓▓░░░░░│ Mitoses + immature cells = LOWER 2/3 │
│ (HSIL) │ │ 20% progress to CIS; 5% to invasion │
│─────────────────────────────────────────────────────────────────│
│ CIN 3 │▓▓▓▓▓▓▓▓▓▓▓│ Full thickness involvement │
│ (HSIL) │ │ Includes Carcinoma In Situ (CIS) │
│ │ │ 5% CIS → invasion if untreated │
└─────────────────────────────────────────────────────────────────┘
▓ = immature atypical cells with mitoses
░ = maturing cells
| Feature | CIN 1 | CIN 2 | CIN 3 |
|---|---|---|---|
| Bethesda equivalent | LSIL | HSIL | HSIL |
| Cell immaturity | Lower 1/3 | Lower 2/3 | Full thickness |
| Mitoses | Rare, lower 1/3 | Middle 1/3 | Upper 1/3 |
| Nuclear atypia | Mild | Moderate | Severe |
| Malignant potential | Low (HPV effect) | Moderate | High (true precancer) |
| Regression rate | 60-85% | 40% | 30-35% |
SITE OF ORIGIN
CERVIX (CROSS-SECTION VIEW)
─────────────────────────────
Endocervical canal
│
[Original SCJ] ←── Nabothian cysts / cleft openings
│
TRANSFORMATION ZONE ← CIN ORIGINATES HERE
(metaplastic epithelium)
│
[Active/Physiologic SCJ]
│
Exocervix (original squamous epithelium)
- Anterior lip is twice as likely to develop CIN as the posterior lip
- CIN rarely originates in lateral angles
- CIN does not replace original squamous epithelium - has sharp external border
ETIOLOGY - HPV
- Persistent high-risk oncogenic HPV infection is the principal risk factor
- HPV 16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 68 account for ~90% of high-grade lesions
- HPV-16 is the most common in CIN 2, CIN 3, and invasive cancer
- Malignant transformation requires expression of E6 and E7 oncoproteins
- In the majority of cases, HPV clears spontaneously in 9-15 months
CYTOLOGIC CORRELATES (Bethesda System)
CYTOLOGY HISTOLOGY (CIN)
─────────────────────────────────────────────
ASC-US ──────────────→ CIN 1 (10-20%), CIN 2/3 (3-5%)
ASC-H ──────────────→ CIN 2/3 (higher risk; refer to colposcopy)
LSIL ──────────────→ CIN 1 (predominantly)
HSIL ──────────────→ CIN 2/3 (high risk; immediate colposcopy)
AGC / AIS ───────────→ Adenocarcinoma in situ (specialized management)
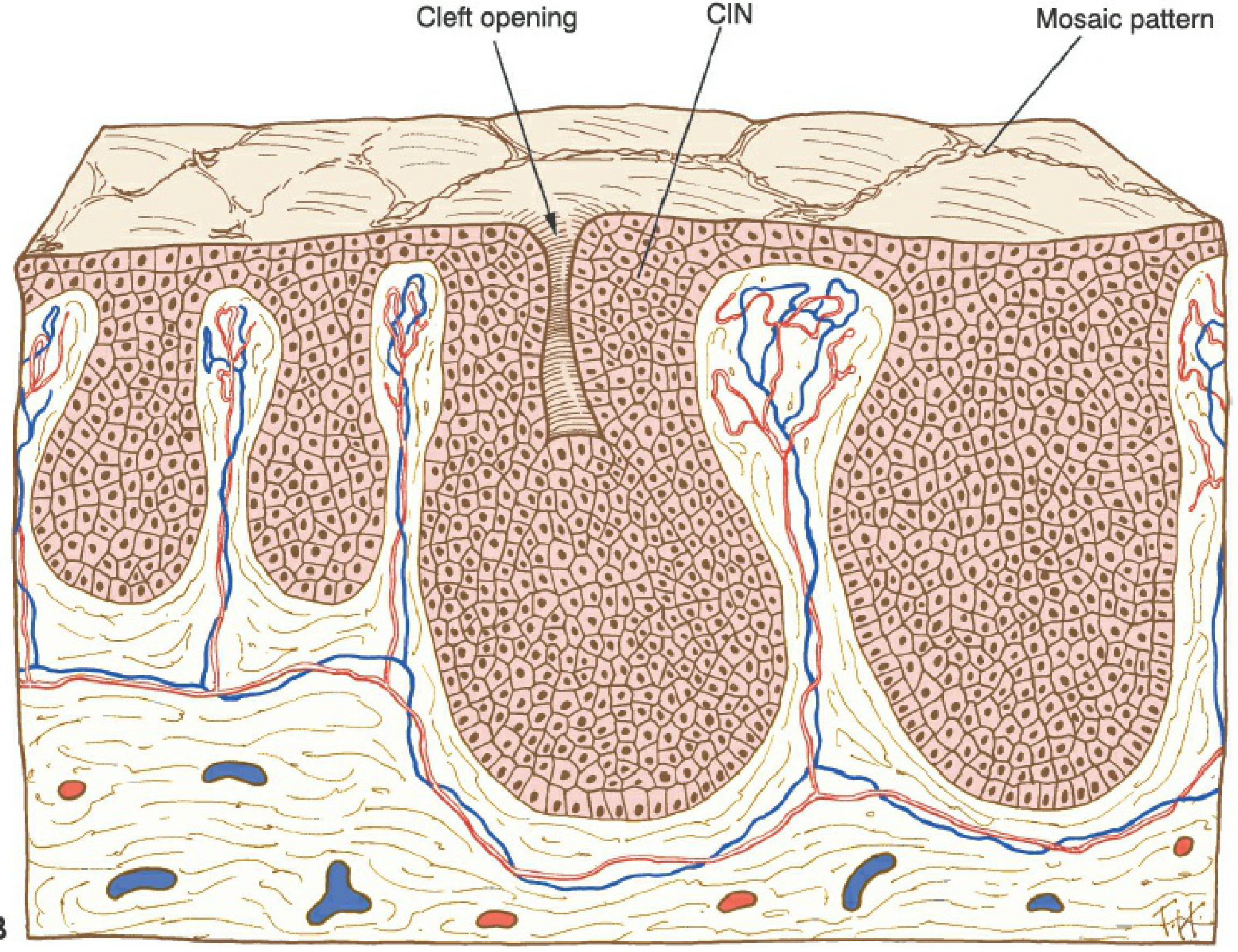
COLPOSCOPIC FINDINGS
| Finding | Description | Grade |
|---|---|---|
| Acetowhite epithelium | White after 3-5% acetic acid | Low to high grade |
| Punctation | End-on capillary loops (dots) | CIN 1-3 |
| Mosaic pattern | Islands of dysplastic epithelium push vessels laterally - looks like mosaic tiles | CIN 2-3 |
| Atypical vessels | Irregular caliber, branching | Suspect invasion |

MANAGEMENT FLOWCHARTS
FLOWCHART 1: CIN 1 Management
BIOPSY-PROVEN CIN 1
│
▼
What was the prior cytology?
┌──────────┴────────────────┐
│ │
ASC-US / LSIL ASC-H / HSIL
│ │
▼ ▼
Satisfactory Higher risk scenario
colposcopy (despite CIN 1 on biopsy)
│ │
▼ ▼
CO-TESTING at 12 months Co-testing at 12 & 24 months
(HPV + cytology) OR
│ Loop Excision (LEEP)
│
┌────┴────────┐
NEGATIVE POSITIVE
(both HPV & (any abnormality)
cytology) │
│ ▼
▼ Return to COLPOSCOPY
Return to
age-appropriate
screening
IF CIN 1 PERSISTS ≥ 24 MONTHS:
┌──────────────────────────────────┐
│ Adequate colposcopy? │
│ YES → Choice of: │
│ a) Continued surveillance │
│ b) Ablation/Excision of TZ │
│ NO → Excision only │
│ (NOT ablation) │
└──────────────────────────────────┘
- CIN 1 is NOT a cancer precursor - it is a manifestation of HPV infection
- Spontaneous regression: 60-85% within 2 years
- Young women (21-24 years): cytology alone at 12 and 24 months (no HPV testing needed)
FLOWCHART 2: CIN 2 and CIN 3 Management
BIOPSY-PROVEN CIN 2 / CIN 3
│
▼
Age and clinical context?
┌────────────────┴────────────────────┐
│ │
Age ≥ 25 years Age < 25 years
(Standard management) OR Pregnant
│ │
▼ ▼
Adequate colposcopy? Intensive observation:
│ - Colposcopy + cytology
┌──┴──┐ at 6 and 12 months
YES NO - If normal at 12 months:
│ │ co-testing at 1 more year
▼ ▼ (Acceptable for CIN 2
LEEP CONIZATION in young women, NOT CIN 3)
(preferred) ──────────────────────────
PREGNANT women:
▼ - Cytology + colposcopy
Post-treatment until 6 weeks postpartum
CO-TESTING at - No treatment during pregnancy
12 and 24 months unless invasive cancer suspected
│
┌──┴──┐
NEG ABNORMAL
│ │
▼ ▼
Return Colposcopy +
to Biopsy ±
routine Retreatment
screening
- CIN 2 progresses to CIS in 20%, to invasion in 5% (meta-analysis)
- CIS progresses to invasion in 5% if untreated
- LEEP is the preferred treatment - allows pathological evaluation to rule out microinvasion
- Persistent/recurrent disease rate post-LEEP: 4-10%
TREATMENT MODALITIES IN DETAIL
1. CRYOTHERAPY
- Uses liquid nitrogen or nitrous oxide (probe temperature: -20 to -30°C)
- Freeze-thaw-freeze technique: 3 minutes freeze, 5 minutes thaw, 3 minutes freeze
- Best for: exocervical, small lesions with fully visible SCJ
- Contraindications: endocervical extension, large lesion (>75% ectocervix), inadequate colposcopy
- Success rate: ~85-90% for CIN 1-2
CRYOTHERAPY CRITERIA ("3 to 2 rule"):
✓ Lesion fits cryoprobe (≤ 3 zones of 5mm, ≤ 2 quadrants)
✓ Entire lesion visible
✓ No endocervical involvement
✓ No adenocarcinoma in situ
✗ NOT if lesion extends into canal
2. LOOP ELECTROSURGICAL EXCISION PROCEDURE (LEEP)
- Uses a thin wire loop carrying electrical current to excise the TZ
- Preferred treatment for CIN 2-3: provides specimen for histopathology
- SCJ visible in >90% of patients after LEEP
- Complications: intraoperative hemorrhage, postoperative hemorrhage, cervical stenosis (low rates)
- Obstetric risk: increased risk of preterm delivery, PROM, low birth weight in future pregnancies
LEEP ADVANTAGES:
✓ Outpatient procedure under local anesthesia
✓ Provides specimen for histology
✓ Can detect occult microinvasive cancer
✓ Can detect adenomatous involvement
✓ SCJ visible after procedure (>90%)
✗ NOT before histologic diagnosis of HSIL confirmed
✗ NOT in pregnancy (unless invasive cancer suspected)
3. CONIZATION (Cold Knife / Laser)
- Diagnostic AND therapeutic procedure
- Provides specimen with accurate surgical margins assessment
- Indicated when:
- Limits of lesion cannot be visualized at colposcopy
- SCJ not evaluable at colposcopy
- ECC positive for CIN 2 or CIN 3
- Substantial discordance between cytology, biopsy, and colposcopy
- Microinvasion suspected
- Colposcopist unable to rule out invasive cancer
- CIN 3 or AGC-AIS requiring diagnostic conization
RECURRENCE RISK AFTER CONIZATION:
- Positive margins → higher recurrence
- Endocervical gland involvement:
With gland involvement: 23.6% recurrence
Without gland involvement: 11.3% recurrence
4. LASER ABLATION
- CO2 laser destroys transformation zone by vaporization
- Precision allows tissue destruction to exact depth needed
- Comparable cure rates to LEEP
5. HYSTERECTOMY
- Treatment of LAST RESORT - only for recurrent high-grade CIN
- Incidence of invasive cancer occurring after hysterectomy for CIN: 0.4% (in 8,998 women)
- Complications (bleeding, infection, death) are higher than with other modalities
- Valid indications for hysterectomy in CIN:
- Recurrent high-grade CIN after excision + patient does not desire fertility
- CIN with other gynecologic pathology requiring hysterectomy
- Patient with inability to comply with surveillance
FLOWCHART 3: Cervical Adenocarcinoma In Situ (AIS) Management
ADENOCARCINOMA IN SITU (AIS)
│
▼
Histologic diagnosis confirmed
│
▼
EXCISION (Cold-knife cone / LEEP)
- Margins critical to assess
- Skip lesions can occur
│
┌─────┴──────┐
NEGATIVE POSITIVE
margins margins
│ │
▼ ▼
Desire future Re-excision
fertility? (repeat cone)
┌────┴──────┐ │
YES NO ▼
│ │ If still positive /
▼ ▼ patient desires no
Surveillance HYSTERECTOMY fertility:
(co-testing) (DEFINITIVE HYSTERECTOMY
TREATMENT)
- Endocervical glandular cells replaced by tall columnar cells with nuclear stratification, hyperchromasia, and atypical mitoses
- Cellular proliferation creates crowded, cribriform glands
- Normal branching pattern of endocervical glands is preserved
- ~50% of women with AIS have concurrent squamous CIN
- Skip lesions make excision critical (not just ablation)
PRECANCEROUS INTRAEPITHELIAL LESIONS - SUMMARY TABLE
| Lesion | Old name | Bethesda | HPV type | Behavior | Primary treatment |
|---|---|---|---|---|---|
| CIN 1 | Mild dysplasia | LSIL | Low/high risk | 60-85% regress | Surveillance |
| CIN 2 | Moderate dysplasia | HSIL | High risk | 40% regress | LEEP |
| CIN 3 / CIS | Severe dysplasia / CIS | HSIL | High risk (HPV 16/18) | 30-35% regress | LEEP / Cone |
| AIS | Adenocarcinoma in situ | AGC/AIS | HPV 18 (mainly) | Uncommon; skip lesions | Cone → Hysterectomy |
| VAIN 1 | - | - | HPV effect | Mostly regress | No treatment |
| VAIN 2-3 | - | - | - | Variable | Excision / laser |
NATURAL HISTORY SUMMARY
HPV Infection (Transient 9-15 months → 90% clear)
│
▼ (persistent high-risk HPV)
CIN 1 (LSIL)
↗ 60-85% REGRESSION
│ 10-15% progression (years)
▼
CIN 2 (HSIL)
↗ 40% REGRESSION
│ 20-25% progression (years)
▼
CIN 3 / CIS (HSIL)
↗ 30-35% REGRESSION
│ 5% invasion over years
▼
Invasive Cervical Carcinoma
- HPV → CIN 1: months
- CIN 1 → CIN 3: 2-10 years
- CIN 3 → Invasion: 5-20 years (provides window for prevention)
KEY POINTS TO REMEMBER (Berek & Novak)
- CIN arises in the TZ at the advancing SCJ - this is where screening and colposcopy focus
- CIN 1 = HPV effect, not a true precancer; 60-85% regress spontaneously
- CIN 2/3 = true precancers requiring treatment in most adults ≥25 years
- LEEP is preferred for CIN 2/3 - gives tissue for histology and rules out invasion
- Ablation is contraindicated when: colposcopy inadequate, lesion in endocervix, microinvasion suspected, AIS present
- Pregnancy: No treatment (only observation); treat only if invasive cancer proven
- Young women (<25): More conservative management; higher spontaneous regression expected
- Positive margins after cone: 23.6% recurrence with gland involvement vs 11.3% without
- HPV 16 and 18 account for most CIN 2/3 and invasive cancer
- Hysterectomy is the last resort - higher complications than conservative treatments
discuss post partum contraception 10 mark answer with easy tables and flow charts from berek and novak for final exam answer without mistake
POSTPARTUM CONTRACEPTION
Comprehensive 10-Mark Answer - Berek & Novak's Gynecology
INTRODUCTION
- Breastfeeding status (lactating vs. non-lactating)
- Time since delivery (immediate / early / delayed)
- Desire for future fertility
WHO Medical Eligibility Criteria (MEC) categories are used to guide safety of each method:
- Category 1: No restriction (use freely)
- Category 2: Advantages outweigh risks
- Category 3: Risks outweigh advantages (use with caution)
- Category 4: Unacceptable health risk (do NOT use)
OVERVIEW TABLE: Methods and Timing
| Method | Start Time (Non-lactating) | Start Time (Lactating) | Efficacy (Pearl Index) | Breastfeeding Impact |
|---|---|---|---|---|
| LAM | - | Immediately (first 6 months) | 98-99% (if criteria met) | Promotes breastfeeding |
| Copper IUD | Immediately postplacental | Immediately postplacental | >99% | None |
| LNG-IUD | Immediately postplacental | Immediately postplacental (caution) | >99% | Minimal |
| Progestin-only pill (POP) | Day 1 postpartum | Day 1 postpartum | 97-99% | No effect on milk |
| DMPA (injectable) | Immediately / within 5 days | After 6 weeks | 99.7% | No effect on milk |
| Implant (etonogestrel) | Immediately | After 4 weeks | >99.9% | No effect on milk |
| COC (estrogen+progestin) | After 21 days | After 6 months (or ≥42 days) | 99% (typical) | May reduce milk quantity |
| Barrier methods | Any time | Any time | 85-97% | None |
| Tubal sterilization | Immediate (within 24-48h) | Immediate or interval | >99.5% | None |
FLOWCHART 1: Initial Decision - Postpartum Contraception
POSTPARTUM WOMAN SEEKING CONTRACEPTION
│
▼
IS SHE BREASTFEEDING?
┌─────────────┴──────────────┐
NO YES
│ │
▼ ▼
Non-lactating path Lactating path
(see Flowchart 2) (see Flowchart 3)
FLOWCHART 2: NON-LACTATING WOMAN
NON-LACTATING POSTPARTUM WOMAN
│
┌─────────┼──────────────────────────────┐
│ │ │
▼ ▼ ▼
WANTS WANTS SPACING WANTS PERMANENT
NOTHING (Reversible method) STERILIZATION
NOW │ │
│ ┌─────┴──────┐ ▼
│ IMMEDIATE DELAYED (>4 wks) TUBAL LIGATION
│ (0-48 hrs) (within 24-48h
│ postpartum OR
▼ interval after 6 wks)
Counsel Immediate:
at 6 wks • Copper IUD (postplacental)
follow-up • LNG-IUD (postplacental)
• Progestin-only implant
• DMPA injection
• Progestin-only pill
After 21 days:
• COC, patch, ring can be started
(VTE risk elevated in first 21 days postpartum)
FLOWCHART 3: LACTATING WOMAN
LACTATING (BREASTFEEDING) POSTPARTUM WOMAN
│
▼
Does she meet ALL 3 LAM criteria?
┌────────────────────────────────────────────┐
│ 1. Exclusively breastfeeding (day & night) │
│ 2. Amenorrhoeic (no menstrual bleed) │
│ 3. < 6 months postpartum │
└────────────────────────────────────────────┘
│
┌────┴────┐
YES NO
│ │
▼ ▼
LAM is Add additional method:
effective • Copper IUD (any time)
(98-99%) • Progestin-only pill (any time)
• Progestin-only implant (any time*)
• DMPA (after 6 weeks)
• LNG-IUD (caution in first 4 wks)
• COC ONLY after 6 months postpartum
(or ≥42 days if not fully breastfeeding)
*Implant: some guidelines say immediate; others advise after 4 wks
INDIVIDUAL METHODS IN DETAIL
1. LACTATIONAL AMENORRHEA METHOD (LAM)
┌──────────────────────────────────────────────────────────┐
│ THE BELLAGIO CONSENSUS (LAM) │
│ │
│ ① EXCLUSIVE BREASTFEEDING │
│ Day AND night feeds; no supplements │
│ │
│ ② AMENORRHEA │
│ No menstrual bleed since delivery │
│ │
│ ③ < 6 MONTHS POSTPARTUM │
│ │
│ All 3 criteria met = 98-99% efficacy │
│ ANY criterion fails → Add backup method │
└──────────────────────────────────────────────────────────┘
- Mechanism: Frequent suckling suppresses GnRH pulsatility → inhibits LH surge → no ovulation
- When LAM fails: First ovulation typically precedes first menstrual period → woman at risk before she realizes LAM has ceased
- Advise: Add contraception immediately when any criterion is no longer met
2. INTRAUTERINE DEVICES (IUDs)
Types Available:
| IUD | Hormone | Approved Duration | Postpartum Use |
|---|---|---|---|
| Copper T380A (ParaGard) | None | 10 years | Excellent - first choice in lactating women |
| Mirena (LNG 52 mg) | 20 µg LNG/day | 5-7 years | Safe; some caution re: breastfeeding |
| Liletta (LNG 52 mg) | Progestin | 4-7 years | Safe |
| Kyleena (LNG 19.5 mg) | Progestin | 5 years | Safe |
| Skyla (LNG 13.5 mg) | Progestin | 3 years | Safe |
Postpartum IUD Insertion Timing:
┌─────────────────────────────────────────────────────────────┐
│ POSTPARTUM IUD TIMING │
├─────────────────────┬───────────────────────────────────────┤
│ POSTPLACENTAL │ Within 10 minutes of placental │
│ (Immediate) │ delivery - vaginal or cesarean │
│ │ Expulsion rate: 24-27% vaginal │
│ │ (lower with C/S) │
├─────────────────────┼───────────────────────────────────────┤
│ EARLY POSTPARTUM │ 48 hrs - 4 weeks: NOT recommended │
│ │ (uterine involution - higher perf. │
│ │ risk, highest expulsion rate) │
├─────────────────────┼───────────────────────────────────────┤
│ INTERVAL INSERTION │ After 4-6 weeks postpartum │
│ │ Standard insertion technique │
│ │ Lower expulsion rate │
└─────────────────────┴───────────────────────────────────────┘
- Copper IUD: "Biologic foam" - fibrin, phagocytic cells, proteolytic enzymes + copper ions → interferes with sperm passage, prevents fertilization
- LNG-IUD: Thickens cervical mucus, causes endometrial atrophy, intrauterine inflammatory response
- Pregnancy, puerperal sepsis, active PID/cervicitis
- Undiagnosed genital bleeding
- Gestational trophoblastic disease (elevated β-hCG)
- Uterine anomalies/fibroids distorting cavity
- Copper IUD: copper allergy, Wilson's disease
3. PROGESTIN-ONLY PILL (POP / "Mini-pill")
- Contains only progestin (no estrogen)
- Safe to start from day 1 postpartum in both lactating and non-lactating women
- Does NOT affect milk quality or quantity (Berek & Novak)
- Must be taken at the same time each day (window: 3 hours)
- Mechanism: Primarily thickens cervical mucus; also suppresses ovulation variably
4. DEPOT MEDROXYPROGESTERONE ACETATE (DMPA / Depo-Provera)
NON-LACTATING: Can start IMMEDIATELY postpartum (within 5 days)
LACTATING: Recommended AFTER 6 weeks postpartum
- 150 mg IM every 12 weeks (or 104 mg SC every 12 weeks)
- Efficacy: 99.7%
- Does NOT affect milk quality or quantity (Berek & Novak)
- Advantages: No daily pill, highly effective, may improve endometriosis/menorrhagia
- Disadvantages: Irregular bleeding, delayed return of fertility (up to 18 months), bone density loss with long-term use
5. SUBDERMAL IMPLANT (Etonogestrel / Nexplanon)
- Single rod implanted in inner upper arm
- Most effective contraceptive available: >99.9% (Pearl Index <0.1)
- Duration: 3 years
- Can be inserted immediately postpartum in non-lactating women
- In lactating women: Generally considered safe immediately; progestin implants do not affect breast milk (blood levels comparable to other progestin-only methods)
- Rapid return of fertility after removal
- Irregular bleeding is the most common complaint
6. COMBINED ORAL CONTRACEPTIVES (COC) / PATCH / RING
┌──────────────────────────────────────────────────────────────┐
│ TIMING FOR COMBINED HORMONAL METHODS │
├──────────────────────────────────────────────────────────────┤
│ NON-LACTATING │ After 21 days postpartum │
│ │ (VTE risk is elevated in first 21 days) │
├──────────────────────────────────────────────────────────────┤
│ LACTATING │ After 6 months postpartum (WHO preferred) │
│ │ OR ≥ 42 days if not exclusively feeding │
│ │ (Estrogen may reduce milk supply) │
└──────────────────────────────────────────────────────────────┘
- VTE risk: Postpartum state is already hypercoagulable; estrogen further increases thrombotic risk
- Milk supply: Estrogen may reduce milk quantity (though evidence is conflicting for modern low-dose pills - Berek & Novak notes combined methods are Category 2 beyond 30 days in breastfeeding women)
7. BARRIER METHODS
- Condoms, diaphragm, cervical cap, spermicides
- Can be started at any time postpartum
- Condoms: Only method that also protects against STIs
- Diaphragm/cap: Fit should be re-assessed after delivery (uterine involution changes anatomy)
- Spermicides: Safe in breastfeeding, but lower efficacy alone (typical use 72%)
- No effect on breastfeeding
8. POSTPARTUM TUBAL STERILIZATION
┌──────────────────────────────────────────────────────────────┐
│ TUBAL STERILIZATION TIMING │
├──────────────────────────────────────────────────────────────┤
│ POSTPARTUM │ Within 24-48 hours of vaginal delivery │
│ (Minilaparotomy)│ At time of cesarean section (concurrent) │
│ │ Uterus still enlarged → fundus near umbilicus│
│ │ Simple subumbilical incision │
├──────────────────────────────────────────────────────────────┤
│ INTERVAL │ At least 6 weeks after delivery │
│ (Laparoscopy) │ Standard technique │
└──────────────────────────────────────────────────────────────┘
| Method | Technique | Reversibility |
|---|---|---|
| Bipolar coagulation | Electrical burn, 3 sites | Poor |
| Falope ring (Silastic band) | Ischemic necrosis of loop | Fair |
| Filshie clip | Mechanical occlusion at isthmus | Fair |
| Hulka clip | Mechanical occlusion at midisthmus | Good |
| Salpingectomy (partial/complete) | Surgical excision | None; also reduces ovarian cancer risk |
MASTER SUMMARY FLOWCHART: Complete Postpartum Contraception Algorithm
POSTPARTUM WOMAN
│
┌───────────────┴────────────────┐
BREASTFEEDING? NOT BREASTFEEDING
│ │
┌─────┴──────┐ ┌──────────┼──────────────┐
EXCLUSIVE PARTIAL/ 0-21 21 days - PERMANENT
(all 3 LAM NOT BF days 6 weeks DECISION?
criteria) │ │ │
│ │ ▼ ▼ ▼
LAM Need Progestin- ALL methods Tubal
+ method only only available sterilization/
backup when now: (IUD, (COC/patch/ Vasectomy
criteria ↓ POP, ring can
break Copper DMPA, now start)
IUD or implant,
POP or barriers)
Implant
──────
AVOID
COC until
6 months
KEY RULE: AVOID ESTROGEN (COC/patch/ring) in:
• First 21 days (VTE risk ALL women)
• Lactating women < 6 months (reduces milk)
• Lactating women < 42 days (WHO Cat 4)
EFFICACY COMPARISON TABLE
| Method | Perfect Use | Typical Use | Category |
|---|---|---|---|
| Tubal sterilization | 0.5% | 0.5% | Permanent |
| Implant (etonogestrel) | 0.05% | 0.05% | LARC |
| LNG-IUD | 0.1-0.2% | 0.1-0.2% | LARC |
| Copper IUD | 0.6% | 0.8% | LARC |
| DMPA injection | 0.2% | 6% | Short-acting hormonal |
| COC | 0.3% | 9% | Short-acting hormonal |
| POP | 0.3% | 9% | Short-acting hormonal |
| LAM | <2% | - | Natural |
| Male condom | 2% | 18% | Barrier |
| Diaphragm + spermicide | 6% | 12% | Barrier |
| No method | - | 85% | - |
KEY POINTS TO REMEMBER FOR EXAM (Berek & Novak)
- LAM is 98-99% effective only when ALL 3 Bellagio criteria are met simultaneously
- Progestin-only methods (POP, implant, DMPA) do NOT affect breast milk - safe at any postpartum time
- Copper IUD is the best non-hormonal option; also works as emergency contraception within 5 days
- Postplacental IUD has higher expulsion (24-27%) but better overall use at 6 months vs. interval insertion
- COC/estrogen-containing methods: Avoid for 21 days in ALL women (VTE); avoid until 6 months in breastfeeding women (milk supply)
- DMPA in breastfeeding: Delay until 6 weeks (concerns about neonatal progestin exposure in first days)
- Immediate postpartum sterilization: Within 24-48 hours via minilaparotomy - uterine fundus near umbilicus makes it simple
- Salpingectomy is now preferred over tubal ligation - reduces ovarian cancer risk with similar safety
- HIV-positive women: IUDs are NOT contraindicated - no increase in HIV transmission or disease progression
- The "gap" in postpartum care: Women scheduled for interval IUD insertion often do not return - immediate postplacental insertion is preferred despite higher expulsion rate
Make a visual flowchart poster about timing of each method for clinic walls with 2 living children diagnosed with stage 1 carcinoma cervix at 20 weeks of pregnancy from berek and novak and williams 10 mark main m.s exam answer with flow chart diagrams easy explanation
Professional medical clinic wall poster titled "CARCINOMA CERVIX DIAGNOSED IN PREGNANCY - MANAGEMENT FLOWCHART" with clean white background, teal and dark blue color scheme. The poster shows a vertical decision flowchart with clear boxes and arrows: TOP SECTION - Header box: "CARCINOMA CERVIX IN PREGNANCY" with subtitle "Multidisciplinary Team: Gynecologic Oncologist + Perinatologist + Neonatologist + Radiation Oncologist" First diamond decision box: "WHAT IS THE FIGO STAGE?" with 4 arrow paths going down and sideways: LEFT PATH - "STAGE IA1 (invasion <3mm, no LVSI)": Box 1: "Conization with negative margins (2nd trimester preferred)" → Box 2: "Follow-up colposcopy every trimester" → Box 3: "Continue pregnancy to term" → Box 4: "CESAREAN SECTION preferred" → Box 5: "Definitive treatment 6 weeks postpartum (Hysterectomy or surveillance)" CENTER-LEFT PATH - "STAGE IA1 with LVSI / STAGE IA2 (3-5mm)": Box 1: "Does patient want to continue pregnancy?" → YES branch: "Delay therapy to fetal maturity → Cesarean + Radical Hysterectomy + Pelvic Lymphadenectomy" → NO branch: "Immediate Radical Hysterectomy with fetus in situ (1st/2nd trimester)" CENTER-RIGHT PATH - "STAGE IB1/IB2 (AT 20 WEEKS)" with RED highlight border: Box 1: "PATIENT CHOICE - Thorough counseling required": → "TERMINATE PREGNANCY: Immediate Radical Hysterectomy + Bilateral Pelvic Lymphadenectomy (Werner type III)" → "CONTINUE PREGNANCY: Neoadjuvant Chemotherapy (Cisplatin-based, after 14 wks) + Review every 4 weeks + Deliver at 32-35 weeks by CLASSIC CESAREAN → Radical Hysterectomy + LND same sitting OR postoperative Chemoradiation" RIGHT PATH - "STAGE IIB-IV": Box: "DO NOT DELAY THERAPY" → "Terminate pregnancy + Chemoradiation (Cisplatin + RT)" → "OR if viable fetus: Classical Cesarean → Start chemoradiation" BOTTOM SECTION - Yellow warning box: "KEY RULES: ① Vaginal delivery CONTRAINDICATED in cervical cancer ② Classic (vertical) Cesarean incision preferred ③ No treatment delay >4 weeks without clear benefit ④ MRI preferred imaging (avoid CT/PET in pregnancy)" Bottom footer: "Source: Berek & Novak's Gynecology + Creasy & Resnik's MFM" with small red cross icon. Clean medical poster style, sans-serif fonts, color-coded boxes (green for conservative, orange for intermediate, red for urgent treatment).
400, message: Got more than 4194304 bytes when reading: b'data: {"candidates": [{"content": {"role": "model","parts": [{"inlineData": {"mimeType": "image/png"...'.
We encountered an error while processing your request. Please try again or reach out to us for help.
discuss the management of lady with 3rd gravida with 2 living children diagnosed with stage 1 carcinoma cervix at 20 weeks of pregnancy from berek and novak and williams 10 mark main m.s exam answer with flow chart diagrams easy explanation
MANAGEMENT OF STAGE I CARCINOMA CERVIX IN PREGNANCY
(G3P2L2 diagnosed at 20 weeks gestation)
10-Mark MS Main Exam Answer - Based on Berek & Novak's Gynecology + Creasy & Resnik's MFM (Williams equivalent)
INTRODUCTION
- Family is complete (2 living children) → fertility preservation is NOT a priority
- The oncologic interest of the mother takes precedence once this is established
- This is an invasive cancer in a previable/borderline viable fetus - the most challenging management window
Incidence: 1.2 in 10,000 pregnancies (Berek & Novak) Diagnosis is often delayed because bleeding is attributed to pregnancy complications
STEP 1 - CONFIRM DIAGNOSIS AND STAGING
SUSPICIOUS PAP / CERVICAL LESION IN PREGNANCY
│
▼
COLPOSCOPY + DIRECTED BIOPSY
(safe in pregnancy at any gestation)
│
┌─────┴──────┐
BIOPSY COLPOSCOPY
CONFIRMS CANNOT RULE
INVASION OUT INVASION
│ │
▼ ▼
CLINICAL CONIZATION
STAGING (NOT before 2nd trimester;
abort risk 33% in 1st trimester;
perform only if essential)
FIGO 2018 STAGING (applies in pregnancy too):
| Stage | Description |
|---|---|
| IA1 | Invasion ≤3 mm depth, no LVSI |
| IA2 | Invasion 3-5 mm depth |
| IB1 | Clinically visible lesion ≤2 cm |
| IB2 | Clinically visible lesion 2-4 cm |
| IB3 | Clinically visible lesion >4 cm |
IMAGING IN PREGNANCY:
- MRI = PREFERRED - safe in pregnancy, best for defining tumor extent and parametrial spread
- Chest X-ray = acceptable (abdominal shielding)
- CT scan - avoid if possible (ionizing radiation); use if MRI unavailable
- PET scan - avoid (safety data in pregnancy lacking)
STEP 2 - THE KEY DECISION FRAMEWORK
"Management of cervical cancer in pregnancy must be individualized. A multidisciplinary team - perinatologist, neonatologist, radiation oncologist, and gynecologic oncologist - should be recruited." (Creasy & Resnik)
Three pivotal questions that determine management:
┌────────────────────────────────────────────────────────────┐
│ QUESTION 1: What is the FIGO STAGE? │
│ → IA1 / IA2 / IB1 / IB2 / IB3 │
├────────────────────────────────────────────────────────────┤
│ QUESTION 2: What is the GESTATIONAL AGE? │
│ → <20 wks / 20-28 wks / 28-34 wks / >34 wks │
├────────────────────────────────────────────────────────────┤
│ QUESTION 3: Does the PATIENT WISH TO CONTINUE PREGNANCY? │
│ → Yes (delay treatment) / No (immediate treatment) │
│ → In this case: G3P2L2 - family complete │
│ → Counseling should lean toward definitive Rx │
└────────────────────────────────────────────────────────────┘
MASTER MANAGEMENT FLOWCHART
G3P2L2, 20 WEEKS, STAGE I CARCINOMA CERVIX
│
▼
┌────────────────────────────────────┐
│ MULTIDISCIPLINARY TEAM COUNSELING │
│ Explain: prognosis, treatment │
│ options, fetal outcomes at 20 wks │
│ (fetus currently NOT viable - │
│ viability begins ~24 weeks) │
└────────────────┬───────────────────┘
│
┌──────────┴──────────┐
STAGE IA1/IA2 STAGE IB1/IB2/IB3
│ │
(see Flowchart A) (see Flowchart B)
FLOWCHART A: STAGE IA1 AND IA2 AT 20 WEEKS
STAGE IA1 (invasion ≤3mm, NO LVSI)
│
▼
Conization with NEGATIVE MARGINS
(performed in 2nd trimester, in OT)
│
┌────────┴────────┐
NEGATIVE POSITIVE
MARGINS MARGINS
│ │
▼ ▼
Follow-up Counsel for
colposcopy RISK OF RESIDUAL
every trimester INVASIVE DISEASE
│ → Repeat cone OR
▼ → Definitive therapy
Continue pregnancy
to 32-35 weeks
(fetal lung maturity by amniocentesis)
│
▼
CLASSICAL CESAREAN SECTION
(NOT vaginal delivery - see note*)
│
▼
Postpartum (6 weeks):
EXTRAFASCIAL HYSTERECTOMY
(if no desire for fertility -
as in this G3P2L2 patient)
──────────────────────────────────────────
STAGE IA1 with LVSI OR STAGE IA2
(invasion 3-5 mm)
│
▼
Does patient want to continue
pregnancy? (G3P2L2 = family complete
→ may opt to terminate)
│
┌────────┴──────────┐
CONTINUE TERMINATE / DELIVER
PREGNANCY IMMEDIATELY
│ │
▼ ▼
Follow to fetal GRAVID RADICAL
maturity (32-35 wks) HYSTERECTOMY
│ + PELVIC LND
▼ (feasible in 1st/2nd
CLASSICAL C/S trimester)
│
▼
MODIFIED RADICAL
HYSTERECTOMY
+ PELVIC LND
(same sitting after C/S)
FLOWCHART B: STAGE IB AT 20 WEEKS (THE MAIN SCENARIO)
STAGE IB1 / IB2 / IB3 AT 20 WEEKS
│
▼
┌──────────────────────────────────────────────┐
│ PATIENT COUNSELING │
│ • Fetus currently NOT viable (20 wks) │
│ • Family complete (G3P2L2) │
│ • Delay of therapy = risk to mother │
│ • Immediate therapy = loss of pregnancy │
│ • Neoadjuvant chemo option if delay desired │
└──────────────────┬───────────────────────────┘
│
┌─────────────┴──────────────────────┐
OPTION 1 OPTION 2
TERMINATE PREGNANCY CONTINUE PREGNANCY
+ IMMEDIATE TREATMENT (delay definitive Rx)
│ │
▼ ▼
STAGE IB1 (small): NEOADJUVANT CHEMOTHERAPY
RADICAL HYSTERECTOMY (cisplatin-based, after 14 wks)
Type III (Wertheim's) + Review EVERY 4 WEEKS
+ BILATERAL PELVIC LND + MRI at 4-6 week intervals
(preferred if operable) + Aim for delivery 32-34 weeks
│ (when fetal lungs mature)
▼ │
STAGE IB2/IB3 (bulky): ▼
CONCURRENT CLASSICAL CESAREAN
CHEMORADIATION + RADICAL HYSTERECTOMY
(Cisplatin + EBRT + PELVIC LND
+ Brachytherapy) (same sitting or staged)
THE CRITICAL POINTS AT 20 WEEKS (G3P2L2)
┌─────────────────────────────────────────────────────────────────┐
│ RECOMMENDED PATH FOR THIS PATIENT │
│ │
│ Stage IA1 (no LVSI): Can reasonably wait until viability │
│ ────────────────────────────────────────────────────────── │
│ Stage IA1 (+ LVSI) / IA2: │
│ → Option to terminate and immediate radical hysterectomy + LND │
│ │
│ Stage IB1: │
│ → STRONGLY RECOMMENDED: Terminate pregnancy + │
│ WERTHEIM'S RADICAL HYSTERECTOMY + PELVIC LND │
│ → If patient refuses termination: │
│ NEOADJUVANT CHEMO + deliver at 32-34 wks + │
│ Classical C/S + Radical Hysterectomy same sitting │
│ │
│ Stage IB2/IB3: │
│ → Terminate pregnancy IMMEDIATELY + │
│ CONCURRENT CHEMORADIATION │
│ (Cisplatin 40 mg/m² weekly + EBRT + Brachytherapy) │
└─────────────────────────────────────────────────────────────────┘
Berek & Novak: "Although timing is controversial, it is probably unwise to delay therapy for longer than 4 weeks."
Creasy & Resnik: "Intentional delays in treatment have been reported from 6 to 32 weeks for women with Stage I-II disease without significant compromise in outcome - but careful counseling and documentation are imperative."
MODE OF DELIVERY
┌──────────────────────────────────────────────────────────┐
│ VAGINAL DELIVERY - CONTRAINDICATED │
│ │
│ Berek & Novak (multivariate analysis of 56 women): │
│ "Vaginal delivery was the MOST SIGNIFICANT │
│ PREDICTOR OF RECURRENCE in women with cervical │
│ cancer diagnosed during pregnancy." │
│ │
│ Most recurrences after vaginal delivery = DISTANT SITES │
│ (including episiotomy site metastasis - rare but real) │
└──────────────────────────────────────────────────────────┘
CESAREAN SECTION: CLASSICAL (VERTICAL UTERINE) INCISION
• Avoids cervical trauma
• Avoids tumor dissemination
• Allows immediate access for radical hysterectomy
• Classical = vertical fundal incision (NOT lower segment)
→ lower segment is in close proximity to the tumor
SURGICAL PROCEDURE: WERTHEIM'S RADICAL HYSTERECTOMY
CLASSICAL CESAREAN SECTION (vertical incision)
│
▼ (immediate, same anesthesia)
WERTHEIM'S RADICAL HYSTERECTOMY (TYPE III)
│
┌─────────┼──────────────────────────────┐
│ │ │
▼ ▼ ▼
UTERUS BILATERAL UPPER 1/3 VAGINA
CERVIX PARAMETRIA (2-3 cm cuff)
+ (medial, middle
TUBES parametrium
+ resected to
OVARIES lateral pelvic
(may be wall)
conserved
in young
patients)
│
▼
BILATERAL PELVIC LYMPHADENECTOMY
(external iliac, internal iliac,
obturator nodes)
│
▼
Specimen sent for frozen section
→ If nodes POSITIVE: Add adjuvant
CHEMORADIATION postoperatively
→ If margins POSITIVE: Add
adjuvant CHEMORADIATION
NEOADJUVANT CHEMOTHERAPY (If Patient Opts to Continue Pregnancy)
Berek & Novak: "Neoadjuvant chemotherapy has been administered to women during pregnancy with cervical cancer after 13 weeks gestation, without clear short-term harm to the fetus."
Creasy & Resnik: "Neoadjuvant chemotherapy can be used for women electing to continue pregnancy who may be deemed high risk for adverse outcomes with delay in therapy."
NEOADJUVANT CHEMOTHERAPY PROTOCOL:
─────────────────────────────────────────────────────
Drug: CISPLATIN (± Paclitaxel or Vinblastine)
Timing: ONLY after 14 weeks (organogenesis complete)
Route: Intravenous
Monitoring: Fetal ultrasound + growth surveillance
Maternal CBC, renal function each cycle
Goal: Tumor stabilization/downsizing until fetal maturity
─────────────────────────────────────────────────────
FETAL DELIVERY TARGET:
• 32 weeks: 75% neonatal survival (modern NICU care)
• 34 weeks: ~90% neonatal survival
• Fetal lung maturity: Confirmed by AMNIOCENTESIS
before delivery
POSTPARTUM MANAGEMENT SUMMARY
| Timing | Action |
|---|---|
| Immediate (0-48h) | Classical Cesarean + Radical Hysterectomy (if surgery chosen) |
| OR at 6 weeks postpartum | Definitive surgery/chemoradiation (if delivery first strategy) |
| 3 months post-treatment | Surveillance imaging (CT/PET) |
| Every 3 months × 2 years | Clinical examination, Pap vault, tumor markers |
| After 2 years: every 6 months | Surveillance continues up to 5 years |
PROGNOSIS (Berek & Novak)
PROGNOSIS IN CERVICAL CANCER IN PREGNANCY:
────────────────────────────────────────────
• Stage is the MOST IMPORTANT prognostic factor
• OS is SLIGHTLY BETTER than non-pregnant patients
(because higher proportion have Stage I disease)
• ADVANCED DISEASE: Pregnancy IMPAIRS prognosis
• POSTPARTUM DIAGNOSIS: Associated with more
advanced stage + DECREASED SURVIVAL
(diagnosis often delayed)
────────────────────────────────────────────
5-Year Survival by Stage (approximate):
IA1: >95%
IA2: 85-95%
IB1: 80-90%
IB2: 75-85%
IB3: 70-80%
SUMMARY TABLE: STAGE I CERVIX IN PREGNANCY AT 20 WEEKS (G3P2L2)
| Stage | Fetus NOT Viable (20 wks) | If Pt Wants to Continue |
|---|---|---|
| IA1 (no LVSI) | Cone biopsy → follow to term → classical C/S → extrafascial hysterectomy 6 wks postpartum | Continue; follow colposcopy each trimester |
| IA1 + LVSI / IA2 | Gravid radical hysterectomy + pelvic LND (terminate first) | Modified radical hysterectomy + LND after classical C/S at 32-34 weeks |
| IB1 | Terminate + Wertheim's radical hysterectomy Type III + bilateral pelvic LND | NACT (cisplatin-based) → Classical C/S + radical hysterectomy at 32-34 wks |
| IB2 | Terminate + Concurrent chemoradiation (Cisplatin + EBRT + BRT) | NACT + classical C/S + chemoradiation postoperatively |
| IB3 | Terminate + Chemoradiation immediately | NOT recommended to delay; terminate + chemoradiation |
KEY EXAM POINTS - DO NOT MISS
- Vaginal delivery is CONTRAINDICATED in any stage cervical cancer - it is the single most significant predictor of recurrence (Berek & Novak)
- Classical (vertical) cesarean incision is used - NOT lower segment (tumor proximity)
- At 20 weeks the fetus is NOT viable - this strongly influences toward immediate definitive treatment
- G3P2L2 = family complete - fertility preservation (trachelectomy) is NOT indicated
- Radical trachelectomy in pregnancy is NOT recommended - up to 20% pregnancy loss (Creasy & Resnik)
- Delay of therapy >4 weeks is unwise (Berek & Novak) - however up to 16-32 weeks delay has been reported in select Stage I-II cases with similar outcomes
- MRI is the imaging of choice in pregnancy for staging
- Neoadjuvant chemotherapy only after 14 weeks (organogenesis complete) - cisplatin-based
- If surgery done, frozen section of nodes - positive nodes → add adjuvant chemoradiation
- Multidisciplinary team is mandatory: Gynecologic oncologist + Perinatologist + Neonatologist + Radiation oncologist
no i want only answer from williams and berek and novak
- Berek & Novak's Gynecology - available ✓
- Creasy & Resnik's Maternal-Fetal Medicine - available ✓
- Berek & Novak only (strictly attributed)
- Berek & Novak + Creasy & Resnik (same content, clearly labeled)