Blood pressure
Reading File
Asking for Preferences
All explain in detail
Finding Sources
Searching the Web
blood pressure physiology regulation hypertension overview 2024
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
I now have comprehensive information from multiple authoritative textbooks. Let me compile the full detailed answer.
Blood Pressure: A Comprehensive Overview
1. Definition & Units
Blood pressure (BP) is the force exerted by blood against any unit area of the vessel wall. It is measured in millimeters of mercury (mm Hg) - a standard introduced by Poiseuille in 1846. A pressure of 100 mm Hg means the force is sufficient to push a column of mercury 100 mm high against gravity.
- 1 mm Hg = 1.36 cm H₂O (because mercury's specific gravity is 13.6)
The key pressures are:
| Parameter | Value | Meaning |
|---|---|---|
| Systolic BP (SBP) | ~120 mm Hg | Peak pressure during ventricular contraction |
| Diastolic BP (DBP) | ~80 mm Hg | Minimum pressure during ventricular relaxation |
| Mean Arterial Pressure (MAP) | ~100 mm Hg | Driving force for tissue blood flow |
| Pulse Pressure | ~40 mm Hg | SBP minus DBP |
- Guyton and Hall Textbook of Medical Physiology, p. 2075
2. Fundamental Equation
Mean Arterial Pressure (MAP) = Cardiac Output (CO) × Total Peripheral Resistance (TPR)
This is the single most important equation in cardiovascular physiology:
- CO = Heart rate × Stroke volume
- TPR = Resistance in all systemic vessels combined (mainly arterioles)
MAP can be altered by changing either CO, TPR, or both. Importantly, CO and TPR are not independent - if TPR doubles, CO will simultaneously decrease by nearly half, so MAP rises only modestly.
- Costanzo Physiology 7th Edition, p. 550
3. Regulation of Blood Pressure
The body maintains MAP at approximately 100 mm Hg through three overlapping systems operating at different time scales:
A. Short-Term: Baroreceptor Reflex (seconds)
This is the fastest blood pressure regulator - neurally mediated and active within seconds.
Baroreceptors are stretch-sensitive mechanoreceptors located in:
- The carotid sinus (wall of the internal carotid artery)
- The aortic arch
How it works when BP rises:
- Baroreceptors detect stretch → increased firing rate in CN IX (glossopharyngeal) and CN X (vagus)
- Signals travel to the nucleus tractus solitarius (NTS) in the medulla
- NTS directs:
- Increased parasympathetic outflow → slows SA node → ↓ heart rate
- Decreased sympathetic outflow → ↓ HR, ↓ contractility, arteriolar vasodilation (↓ TPR), venodilation (↑ venous capacitance)
- CO ↓ + TPR ↓ → MAP returns toward 100 mm Hg
How it works when BP falls (e.g., hemorrhage):
- Opposite response: ↑ sympathetic, ↓ parasympathetic → ↑ HR, ↑ contractility, vasoconstriction → ↑ MAP
The baroreceptor reflex can be clinically tested with the Valsalva maneuver (forced expiration against a closed glottis).
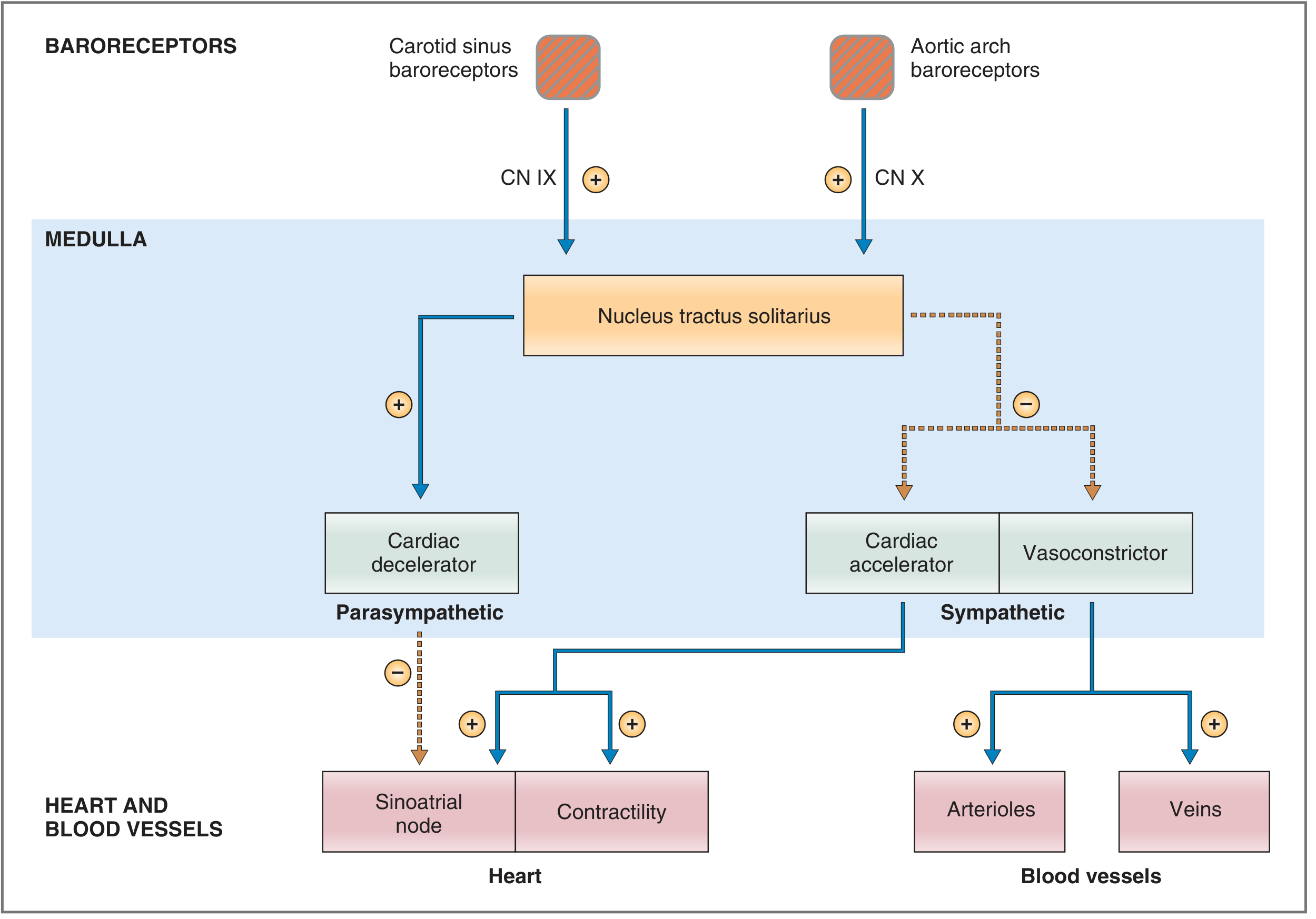
Baroreceptor reflex pathway - Costanzo Physiology 7th Edition
B. Medium-to-Long-Term: Renin-Angiotensin-Aldosterone System (RAAS) (hours-days)
This hormonal system is slower but more sustained than the baroreceptor reflex. Activated when MAP falls:
-
↓ Renal perfusion pressure → mechanoreceptors in afferent arterioles → juxtaglomerular cells convert prorenin to renin
- Also stimulated by: renal sympathetic nerve activity, β₁ agonists
- Inhibited by: β₁ antagonists (e.g., propranolol)
-
Renin cleaves angiotensinogen (from liver) → Angiotensin I (inactive decapeptide)
-
Angiotensin-Converting Enzyme (ACE) in lungs/kidneys converts Angiotensin I → Angiotensin II (active octapeptide)
-
Angiotensin II acts on multiple targets via AT1 receptors:
- Adrenal cortex (zona glomerulosa) → secretes aldosterone → ↑ Na⁺ reabsorption in distal tubule/collecting duct → ↑ ECF volume → ↑ blood volume → ↑ CO → ↑ MAP
- Arterioles (via IP3/Ca²⁺) → vasoconstriction → ↑ TPR → ↑ MAP
- Hypothalamus → ↑ thirst + stimulates ADH → ↑ water reabsorption → ↑ blood volume
- Renal proximal tubule → stimulates Na⁺-H⁺ exchange → ↑ Na⁺ + HCO₃⁻ reabsorption
- Costanzo Physiology 7th Edition, p. 680-700
C. Long-Term: Renal-Body Fluid System (days-weeks)
The most powerful long-term control mechanism. If blood volume rises, arterial pressure rises, which causes:
- Pressure diuresis - kidneys excrete more water
- Pressure natriuresis - kidneys excrete more sodium
An increase in arterial pressure of just a few mm Hg can double renal output of water and salt. This system is fundamental for long-term BP homeostasis and is the primary reason the kidney is central to hypertension.
- Guyton and Hall Textbook of Medical Physiology, p. 3892-3914
D. Other Regulatory Mechanisms
| Mechanism | Effect |
|---|---|
| ANP/BNP (atrial/brain natriuretic peptides) | Released by cardiac stretch → natriuresis, vasodilation → ↓ BP |
| Endothelin | Potent vasoconstrictor from endothelium |
| Nitric oxide (NO) | Vasodilator from endothelium → ↓ TPR |
| ADH (vasopressin) | Water retention + vasoconstriction |
| Local autoregulation | Organs regulate their own blood flow independently |
4. Measurement of Blood Pressure
Clinical Methods
| Method | Details |
|---|---|
| Sphygmomanometer + Korotkoff sounds | Standard indirect method; cuff inflated above SBP, slowly deflated; first sound = SBP, disappearance = DBP |
| Electronic oscillometric | Used in automated/ambulatory devices |
| Intra-arterial catheter | Gold standard; continuous waveform; used in ICU |
High-fidelity electronic transducers convert BP to electrical signals using:
- Capacitance transducers (metal membrane)
- Inductance transducers (iron slug in coil)
- Resistance transducers (strain gauge wire)
These can record up to 500 pressure cycles/sec.
- Guyton and Hall Textbook of Medical Physiology, p. 2079-2104
5. Blood Pressure Classification (ACC/AHA 2017)
| Category | Systolic (mm Hg) | Diastolic (mm Hg) | |
|---|---|---|---|
| Normal | < 120 | AND | < 80 |
| Elevated | 120-129 | AND | < 80 |
| Stage 1 Hypertension | 130-139 | OR | 80-89 |
| Stage 2 Hypertension | ≥ 140 | OR | ≥ 90 |
| Hypertensive Crisis | > 180 | OR | > 120 |
Note: The 2024 ESC Guidelines define hypertension as SBP ≥ 140 and/or DBP ≥ 90 mm Hg - a somewhat higher threshold than ACC/AHA.
6. Hypertension
Types
- Primary (Essential) hypertension (~90-95%): No identifiable cause; involves genetic, environmental (salt intake, obesity, stress), and renal factors
- Secondary hypertension (~5-10%): Identifiable causes including renal artery stenosis, primary hyperaldosteronism, pheochromocytoma, Cushing syndrome, obstructive sleep apnea, medications (NSAIDs, OCP, steroids)
Pathophysiology of Essential Hypertension
- Increased sympathetic nervous system activity
- Dysregulation of RAAS
- Impaired renal sodium excretion (altered pressure-natriuresis curve)
- Endothelial dysfunction (reduced NO)
- Vascular remodeling (increased TPR)
Complications (End-Organ Damage)
| Organ | Complication |
|---|---|
| Heart | LV hypertrophy, heart failure, CAD, MI |
| Brain | Stroke, hypertensive encephalopathy |
| Kidneys | Hypertensive nephrosclerosis, CKD |
| Eyes | Hypertensive retinopathy |
| Peripheral vessels | PAD, aortic aneurysm |
Hypertension carries a 2.5-fold age-adjusted risk for peripheral arterial disease in men and 3.9-fold in women.
7. Treatment of Hypertension
Lifestyle Modifications (First-line for all stages)
- DASH diet (↓ sodium, ↑ potassium)
- Weight loss
- Regular aerobic exercise
- Limiting alcohol
- Smoking cessation
Pharmacological Treatment
Treatment Goals:
- Most patients: target < 130/80 mm Hg (ACC/AHA 2017)
- 2024 ESC Guidelines: target SBP 120-129 mm Hg for patients on medication
- CKD (KDIGO 2020): SBP < 120 mm Hg
First-line Drug Classes:
| Drug Class | Examples | Mechanism |
|---|---|---|
| Thiazide diuretics | Hydrochlorothiazide, chlorthalidone | ↓ Na⁺ reabsorption → ↓ blood volume |
| ACE Inhibitors (ACEi) | Lisinopril, enalapril, captopril | Block ACE → ↓ Angiotensin II → vasodilation + ↓ aldosterone |
| Angiotensin Receptor Blockers (ARBs) | Losartan, valsartan | Block AT1 receptor → same downstream effect as ACEi |
| Calcium Channel Blockers (CCBs) | Amlodipine, nifedipine (DHP), verapamil | Block Ca²⁺ entry in vascular smooth muscle → vasodilation |
| Beta-blockers | Metoprolol, carvedilol | Block β₁ → ↓ HR, ↓ contractility, ↓ CO; also ↓ renin release |
| Alpha-blockers | Doxazosin | Block α₁ → vasodilation |
| Aldosterone antagonists | Spironolactone | Block aldosterone → natriuresis |
Population-Specific First-line Choices:
- Non-Black patients: Thiazide, ACEi, ARB, or CCB
- Black patients: Thiazide or CCB preferred (ACEi less effective as monotherapy)
- Diabetes: ACEi or ARB (renoprotective)
- CKD: ACEi or ARB
- Heart failure with reduced EF: ACEi/ARB + beta-blocker + aldosterone antagonist
- Post-MI: Beta-blocker + ACEi
Combination Therapy:
-
If SBP > 20 mm Hg above goal OR DBP > 10 mm Hg above goal: start two drugs simultaneously
-
Preferred combinations: ACEi/ARB + CCB, or ACEi/ARB + thiazide
-
Avoid: Non-dihydropyridine CCB (e.g., verapamil) + beta-blocker (both cause bradycardia)
-
Avoid: ACEi + ARB combination (risk of hypotension, hyperkalemia, renal failure)
-
Lippincott Illustrated Reviews Pharmacology, p. 4086-4089
8. Hypotension & Low Blood Pressure
Hypotension is generally defined as SBP < 90 mm Hg or MAP < 65 mm Hg.
Common causes:
- Hypovolemia (dehydration, hemorrhage)
- Cardiogenic (MI, heart failure, arrhythmia)
- Distributive (sepsis, anaphylaxis, neurogenic)
- Obstructive (PE, tension pneumothorax, cardiac tamponade)
- Orthostatic (autonomic dysfunction, medications)
The baroreceptor reflex is the first response to acute hypotension: ↑ sympathetic output → ↑ HR + vasoconstriction → attempt to restore BP.
9. Blood Pressure in Special Populations
| Population | Key Consideration |
|---|---|
| Elderly (>65) | Higher SBP targets acceptable if frailty or orthostatic symptoms; SBP > 85 years → individualize |
| Pregnancy | Hypertension in pregnancy = pre-eclampsia risk; severe HTN treated with labetalol, hydralazine, nifedipine; ACEi/ARBs contraindicated |
| Diabetes | ACEi/ARB preferred to slow progression of diabetic nephropathy |
| CKD | ACEi/ARB first-line; target SBP < 120 mm Hg |
| Children/Adolescents | BP classified as percentile-based for age, sex, and height |
10. Summary: The BP Control Network
SECONDS: Baroreceptor reflex → neural adjustments to HR, TPR
↓
HOURS: RAAS → Angiotensin II → aldosterone → Na⁺ retention → ↑ blood volume
↓
DAYS-WEEKS: Renal pressure-natriuresis → long-term volume & pressure equilibrium
All three systems work in concert. Hypertension develops when one or more of these mechanisms is dysregulated - most commonly through impaired renal sodium excretion, overactive RAAS, or excessive sympathetic tone.
Sources:
- Costanzo Physiology 7th Edition - Regulation of Arterial Pressure (baroreceptor reflex, RAAS)
- Guyton and Hall Textbook of Medical Physiology - Nervous regulation, renal-body fluid system
- Lippincott Illustrated Reviews Pharmacology - Antihypertensive treatment strategies
- 2024 ESC Guidelines for Hypertension - Target BP 120-129 mm Hg for medicated patients
This is a shared conversation. Sign in to Orris to start your own chat.