ARMD
Reading File
Finding Sources
Searching PubMed
"age-related macular degeneration"[MeSH Terms] AND treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Loading Image
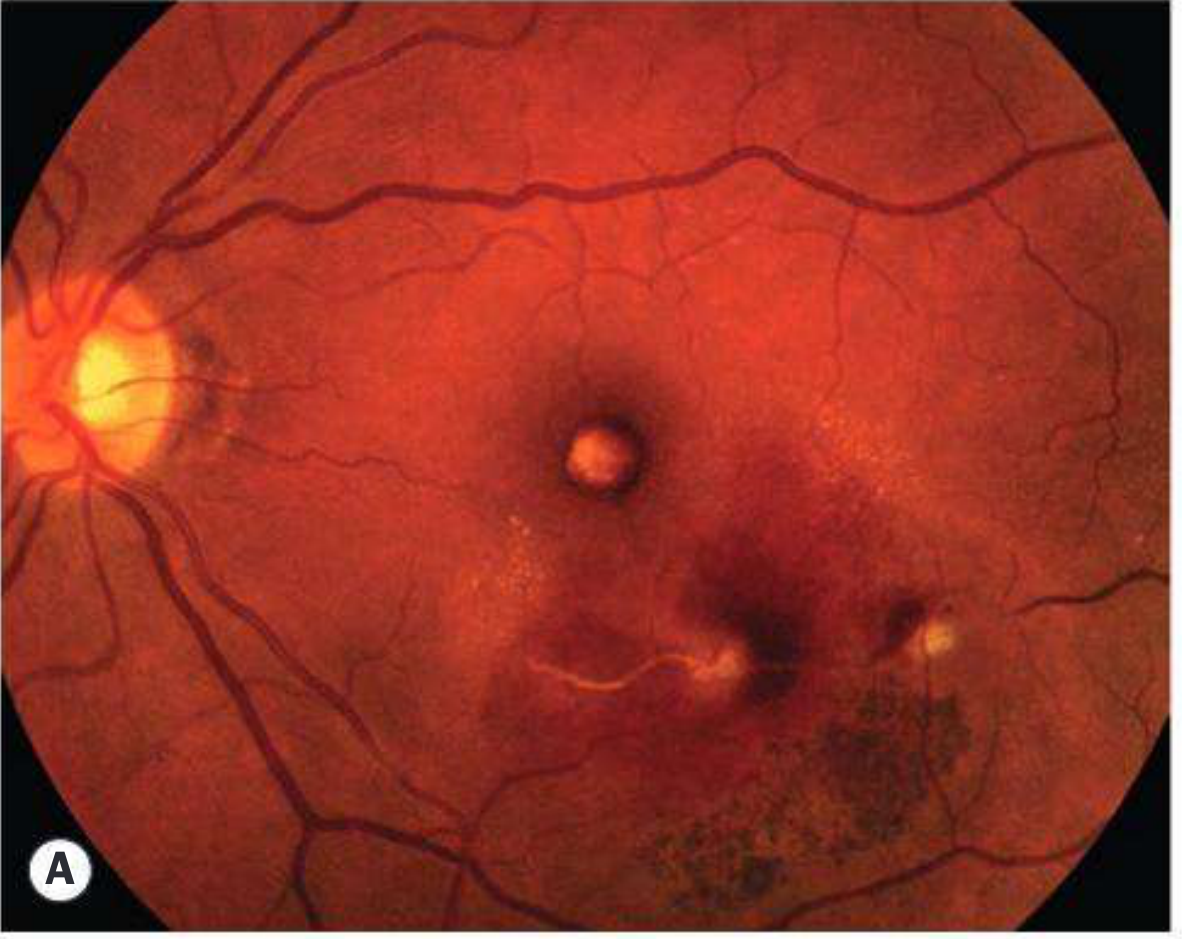
Age-Related Macular Degeneration (ARMD)
Definition & Epidemiology
ARMD is a neurodegenerative disease primarily affecting the retinal pigment epithelium (RPE) of the macula, predominantly in the 6th–9th decades of life. It accounts for ~8.5% of global blindness, mainly in industrialized countries. In the US, it affects >1.75 million persons; prevalence rises with each decade after age 55.
Pathogenesis
The key structural unit involved is the RPE–Bruch membrane–choriocapillaris complex. Disturbance in any component leads to photoreceptor loss.
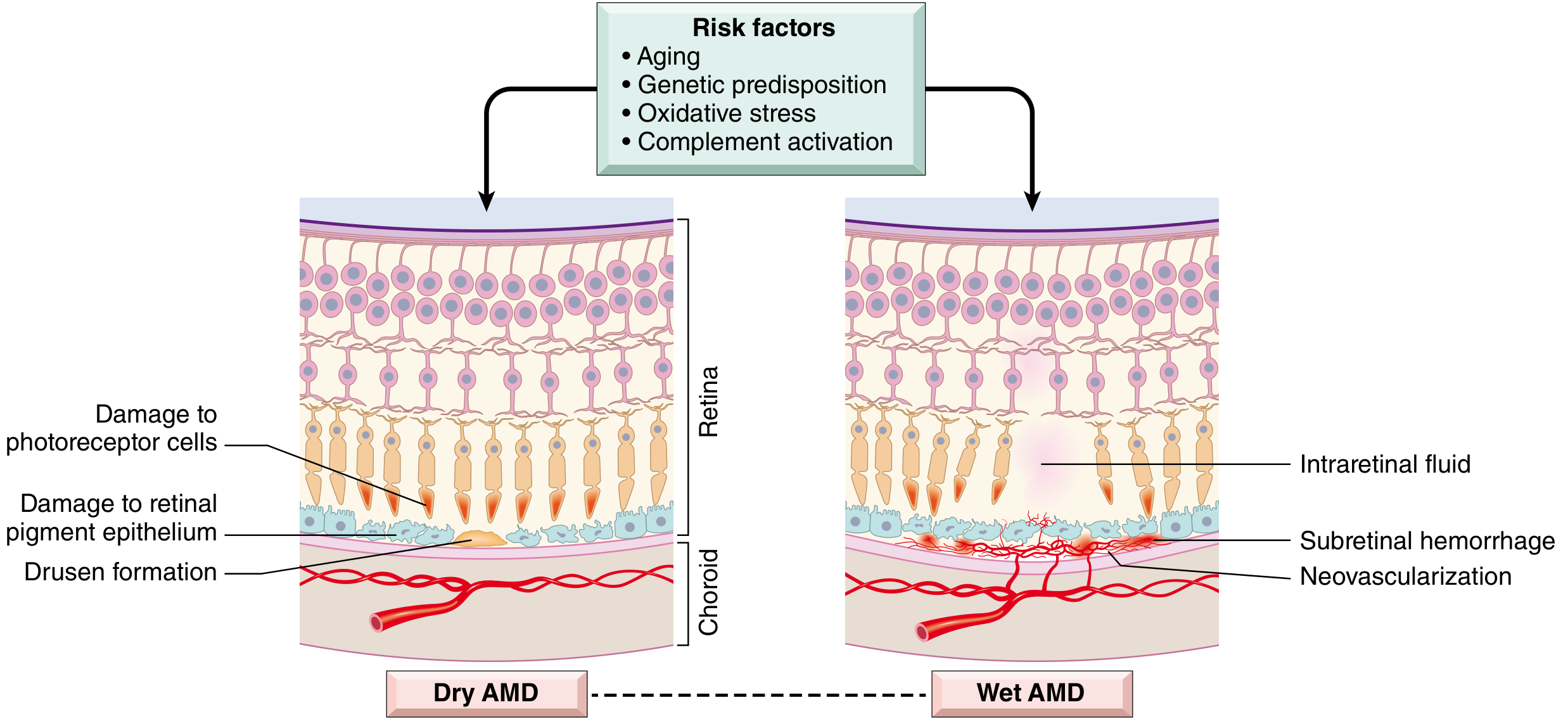
Risk factors: Aging, genetic predisposition (CFH, CFI complement gene polymorphisms — excess complement activity), oxidative stress, smoking, hypertension, dyslipidemia, family history, hyperopia, blue eyes.
Two Major Forms
Dry (Nonexudative / Atrophic) ARMD
- More common (~85–90%); usually precedes wet form
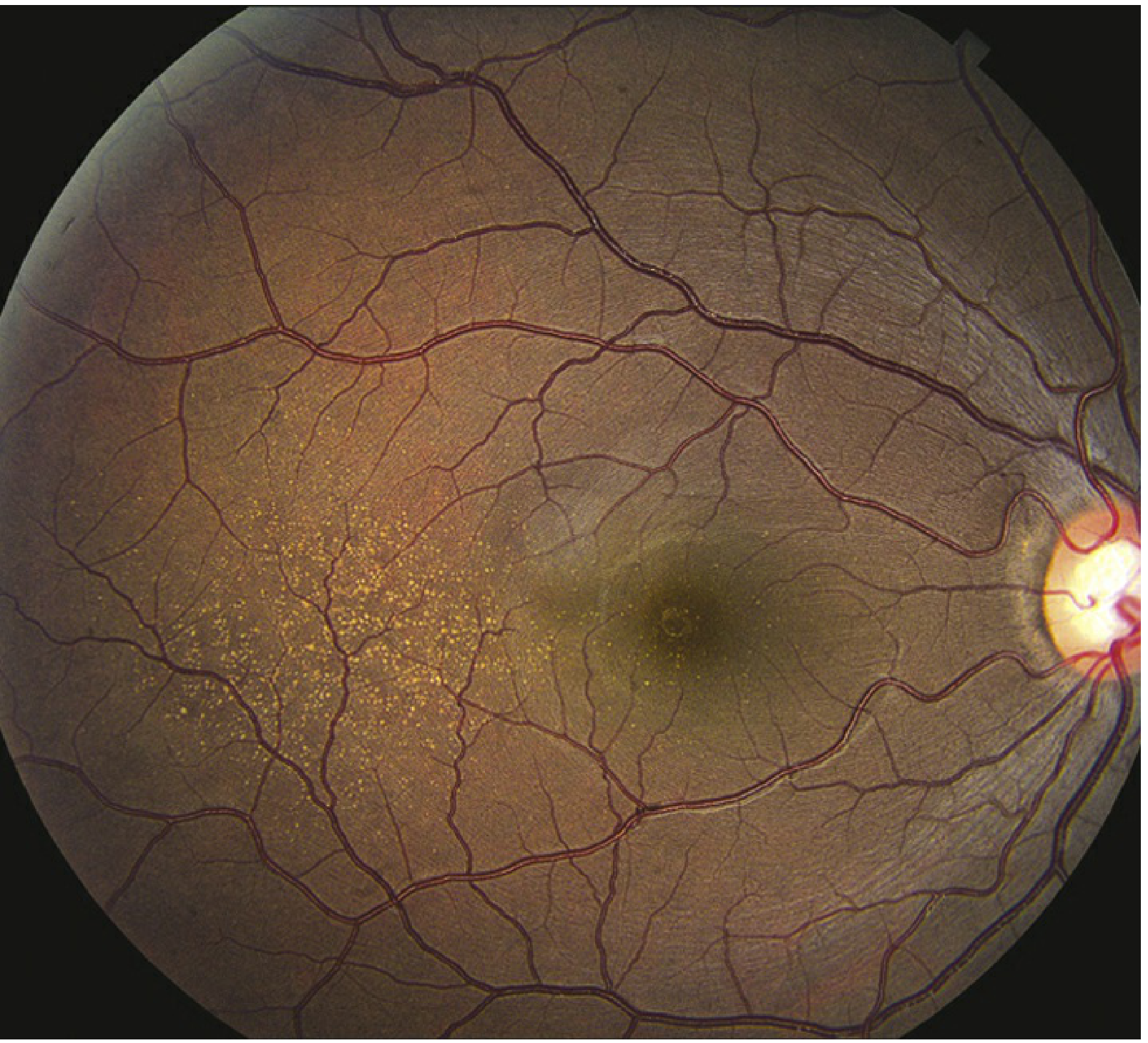
- Characterized by drusen — abnormal lipoprotein deposits within the RPE basement membrane (Bruch membrane), and geographic atrophy of the RPE
- Drusen types:
- Hard drusen: small, well-defined (less significant)
- Soft drusen: >60 μm, hypopigmented spots — higher risk of progression
- Lipofuscin accumulates in stressed RPE cells
- Symptoms: gradual, painless central vision loss; may be asymptomatic for years
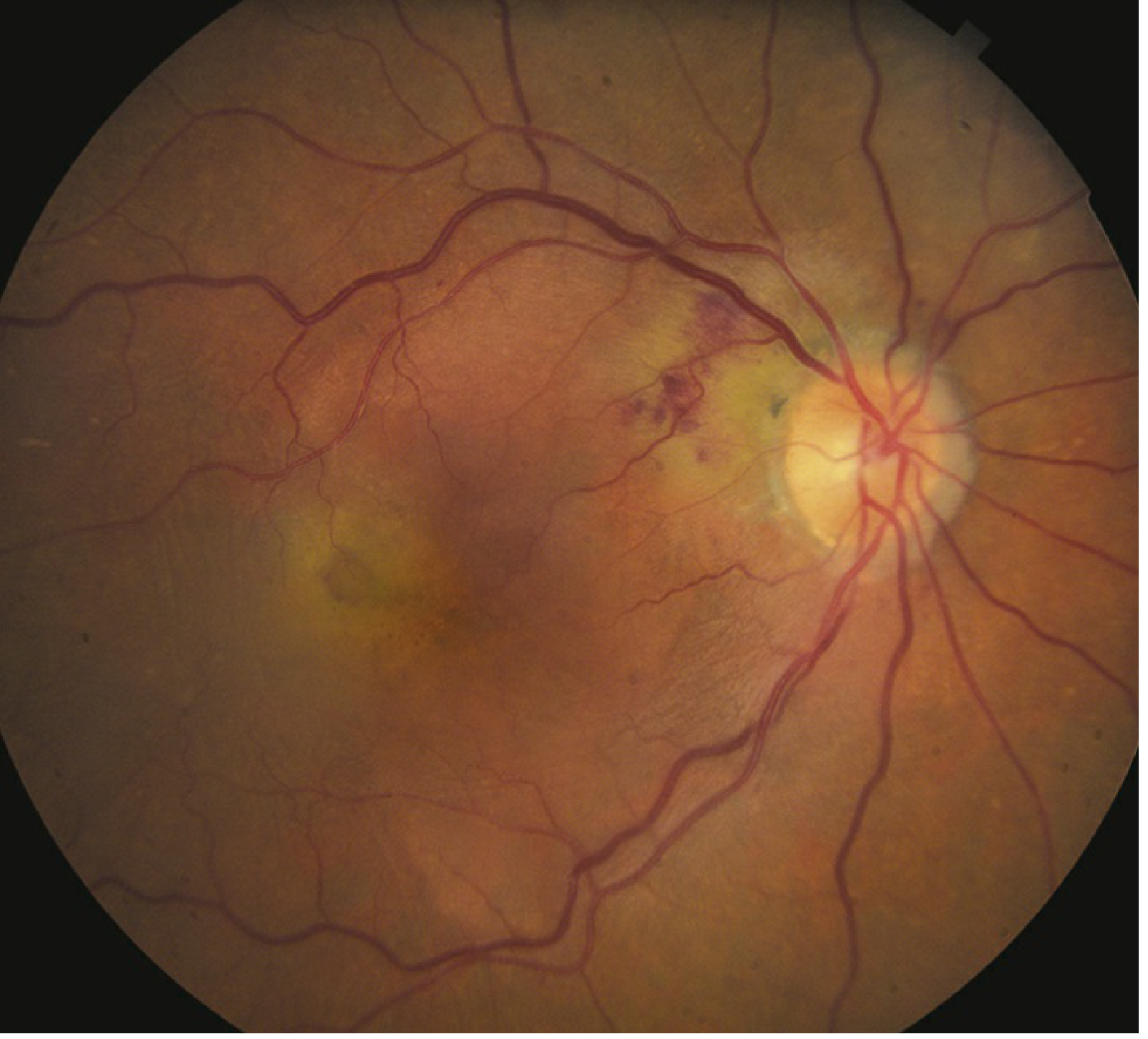
Wet (Neovascular / Exudative) ARMD
- Less common but causes the most profound vision loss
- Frail choroidal neovascular channels (CNV) breach Bruch membrane → grow into subretinal space beneath the RPE → leak fluid, blood, lipids
- Subretinal hemorrhage → acute, often permanent central visual acuity loss
- Both eyes typically affected to similar degree
Key point: Dry and wet AMD are not simply sequential — they can coexist and each develops through distinct pathways. However, dry AMD can convert to wet AMD, especially with soft drusen + RPE clumping.
Types of CNV Lesions (Wet ARMD)
| Type | Description |
|---|---|
| Occult CNV (Type 1) | Under RPE; ill-defined hyperfluorescence on FA |
| Classic CNV (Type 2) | Sub-neurosensory; well-defined lacy hyperfluorescence on early FA with late leakage |
| RAP (Type 3) | Retinal Angiomatous Proliferation — intraretinal; focal telangiectatic vessels, hair-pin loop on ICGA |
| IPCV | Idiopathic Polypoidal Choroidal Vasculopathy — polyp-like aneurysms; more common in Asian and African descent |
Symptoms
- Dry: Gradual central vision loss, Amsler grid changes; peripheral vision preserved
- Wet: Acute/subacute central/paracentral scotoma, metamorphopsia (distorted vision), photopsias; sudden vision loss with hemorrhage
Patients with advanced disease can walk down a street (peripheral retinal function intact) but cannot recognize facial features (macular function lost).
Investigations / Workup
- Amsler grid / preferential hyperacuity perimetry (PHP): Detects central scotoma or metamorphopsia; key for monitoring conversion to wet form
- Fundus biomicroscopy (60/90 D or fundus contact lens): Assess drusen type, geographic atrophy, signs of CNV
- Fluorescein angiography (IVFA): Confirms CNV size, type, location; classic vs. occult lesions
- OCT (optical coherence tomography): Primary modality for follow-up; assesses retinal thickness, SRF, ME, RPE detachment, CNV extent
- OCTA: Non-invasive alternative to IVFA; useful if FA contraindicated (pregnancy, fluorescein allergy)
- ICGA (Indocyanine green angiography): Better delineates occult CNV borders, RAP, and IPCV lesions
Management
Dry ARMD
- No curative treatment currently available
- AREDS2 formula supplements (Vitamins C & E + lutein + zeaxanthin + zinc + copper): Shown to retard progression from moderate → advanced AMD
- ⚠️ β-carotene NOT recommended in smokers (increased lung cancer risk)
- Lifestyle modifications: Smoking cessation (most important modifiable risk factor), control of BP, blood sugar, and lipids
- Monitoring: Regular Amsler grid home testing; urgently seek evaluation if new metamorphopsia develops
- Complement inhibitors (e.g., pegcetacoplan): Emerging therapy targeting geographic atrophy progression
Wet ARMD — Anti-VEGF Therapy (Mainstay)
All injected intravitreally:
| Drug | Class | Notes |
|---|---|---|
| Ranibizumab (Lucentis) | Anti-VEGF Fab fragment | FDA-approved; MARINA/ANCHOR trials: ~40% gained ≥3 lines vision at 1 year |
| Bevacizumab (Avastin) | Full-length anti-VEGF | Off-label; non-inferior to ranibizumab (CATT trial); highly cost-effective |
| Aflibercept (Eylea) | VEGF-A + PlGF fusion protein | FDA-approved; VIEW trials: q8 weeks non-inferior to monthly ranibizumab |
| Brolucizumab (Beovu) | Single-chain anti-VEGF fragment | FDA-approved; HAWK/HARRIER: q8–12 weeks; non-inferior to aflibercept |
| Faricimab (Vabysmo) | Dual inhibitor (Ang-2 + VEGF-A) | Newest; allows extended dosing intervals |
- Dosing regimens: PRN (treat and observe), treat-and-extend (TAE), or fixed interval — individualized based on disease activity
- Risk with wet AMD in one eye: 10–12% per year risk of CNV in the fellow eye
Additional Treatments
- Photodynamic therapy (PDT) with verteporfin: IV photosensitizing dye + cold laser; FDA-approved; given q3 months PRN; now mainly used in IPCV
- Vitrectomy: For massive subretinal hemorrhage in advanced cases
- Low vision aids: Special glasses, video-based magnification — help maintain independence
Key Differentials
| Condition | Key Distinguishing Features |
|---|---|
| Myopic degeneration | Peripapillary changes, lacquer cracks, high myopia, no drusen |
| CSCR | Age <50, serous elevation, no drusen/hemorrhage |
| Stargardt disease | Age <50, lipofuscin deposits, familial, no drusen |
| Chloroquine toxicity | Bull's-eye maculopathy, drug history |
| Ocular histoplasmosis | White-yellow chorioretinal scars + peripapillary atrophy |
| Angioid streaks | Bilateral subretinal bands radiating from disc |
Summary
ARMD is the leading cause of irreversible central vision loss in the elderly in developed countries. The key to management is:
- Dry: AREDS2 supplements + lifestyle modification + monitoring
- Wet: Prompt intravitreal anti-VEGF therapy — time-sensitive; delays lead to irreversible photoreceptor loss
Sources: Goldman-Cecil Medicine; Robbins, Cotran & Kumar Pathologic Basis of Disease; Wills Eye Manual — Goldman-Cecil Medicine International Edition, p. 4133; Robbins Pathologic Basis of Disease, p. 1221–1222; Wills Eye Manual, pp. 832–842
Vitreous substitutes
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Now I have comprehensive information from multiple authoritative sources. Here is a complete review:
Vitreous Substitutes
Vitreous substitutes are agents used to replace the vitreous humor (normally a transparent gel of water, collagen, and hyaluronic acid) following vitrectomy. Their primary role is retinal tamponade — holding the retina in contact with the RPE to allow healing, particularly in complicated retinal detachments, proliferative vitreoretinopathy (PVR), and traction detachments.
Classification
| Category | Agents |
|---|---|
| Gases | Air, Sulfur hexafluoride (SF₆), Perfluoropropane (C₃F₈) |
| Perfluorocarbon liquids (PFCL) | Perfluoro-n-octane, perfluorodecalin (intraoperative only) |
| Silicone oils | Polydimethylsiloxane 1000 cs, 5000 cs |
| Combination agents | Silicone oil + partially fluorinated alkanes (SO-PFA) |
1. Gases
Gases work via buoyancy — they float and press against the superior retina when the patient is positioned appropriately (face-down / specific posturing).
Air
- Duration of tamponade: 3–7 days
- Absorbed fastest; used for straightforward cases or short-term tamponade (e.g., after macular hole surgery)
- Non-expansile
Sulfur Hexafluoride (SF₆)
- Duration: 10–14 days
- Expansile — expands to ~2× original volume as it equilibrates with body gases; must be used at appropriate concentrations to avoid overfill
- Also used in anterior segment:
- Non-expansile concentration after endothelial keratoplasty (DSAEK/DMEK) — helps graft adherence; patient lies face-up 3–5 days
- Treats Descemet's membrane detachments post-cataract surgery
Perfluoropropane (C₃F₈)
- Duration: 55–65 days — longest-lasting gas
- Most expansile (~4× volume); highest risk of IOP elevation if over-concentrated
- Preferred for complex cases requiring prolonged tamponade (e.g., giant retinal tears, inferior breaks)
Key Points for Gases
- Patient posturing is mandatory to position the gas bubble over the retinal break
- ⚠️ Flying contraindicated while gas is in the eye — cabin pressure changes cause dangerous expansion → acute angle-closure glaucoma
- ⚠️ Nitrous oxide (N₂O) anaesthesia contraindicated — N₂O diffuses into gas bubble causing massive expansion
- Complications: elevated IOP, corneal edema, cataract (feathering of posterior subcapsular lens — usually transient), subretinal gas migration, pupillary block
2. Perfluorocarbon Liquids (PFCL)
- Examples: Perfluoro-n-octane, perfluorodecalin
- Specific gravity: 1.76–1.94 — much denser than vitreous and water; sink to the bottom of the eye
- Therefore tamponade the inferior retina (opposite to gases)
- Intraoperative use only — used to:
- Flatten and stabilize the detached retina during surgery
- Unroll giant retinal tears
- Float and displace subretinal blood anteriorly
- Stabilize the retina during membrane peeling in PVR
- After achieving retinal reattachment intraoperatively, PFCL is replaced by gas or silicone oil before wound closure
- Long-term retention is toxic to the retina — cannot be left in permanently
3. Silicone Oil (SO)
Silicone oil = polydimethylsiloxane (PDMS); available in viscosities of 1000 cs and 5000 cs (centistokes).
Properties
- Lighter than water (floats) → tamponades superior retina
- Clear, transparent — allows good visual acuity and fundus visualization
- Permanent/semi-permanent — remains until surgically removed
- Does not require strict posturing (unlike gas)
Indications
- Complex retinal detachments with PVR (grade C or worse)
- Giant retinal tears
- Trauma cases
- Retinal detachments with poor visual potential requiring longer tamponade
- Patients who cannot comply with face-down posturing
- CMV retinitis–related detachments (success rate ~75% with vitrectomy + SO + endolaser)
- Where air travel is required post-operatively (SO is not affected by altitude)
Viscosity Comparison
| Viscosity | Properties |
|---|---|
| 1000 cs | Lower viscosity, easier to inject/remove, more likely to emulsify |
| 5000 cs | Higher viscosity, more resistant to emulsification, longer stability |
SO-PFA Combinations (Heavy Silicone Oil)
- Silicone oil combined with partially fluorinated alkanes (e.g., RMN-3, Oxane HD)
- Specific gravity close to 1 — sits at bottom → tamponades inferior retina
- Useful for inferior retinal breaks and PVR where conventional SO cannot reach
- FDA-approved for clinical use
Complications of Silicone Oil
| Complication | Mechanism/Notes |
|---|---|
| Glaucoma (early) | Pupillary block — especially in aphakic eyes; prevented by inferior (Ando) iridectomy |
| Glaucoma (late) | Emulsified SO droplets migrate to anterior chamber → trabecular obstruction and scarring |
| Cataract | Almost universal in phakic eyes with prolonged SO; silicone-induced nuclear sclerosis |
| Corneal band keratopathy | With extended SO tamponade |
| Corneal edema | Direct SO contact with corneal endothelium |
| Retinal toxicity | With emulsified oil in prolonged contact |
| Emulsification | Breakdown of oil into tiny droplets over time; increased with lower viscosity, eye movements, and inflammation |
Silicone Oil Removal
- Generally removed after 3–6 months once retinal reattachment is stable
- Early removal reduces risk of emulsification-related complications (glaucoma, cataract)
- Some eyes require permanent tamponade (one-eyed patients, poor surgical access)
Comparison Summary
| Feature | Gas (SF₆/C₃F₈) | PFCL | Silicone Oil |
|---|---|---|---|
| Density | Less dense (floats) | Denser than water (sinks) | Less dense (floats) |
| Tamponades | Superior retina | Inferior retina (intraop) | Superior retina |
| Duration | Days–weeks | Intraoperative only | Months–permanent |
| Posturing required | Yes (face-down) | N/A | Less strict |
| Visual acuity | Clear (once absorbed) | Intraop only | Good (myopic shift) |
| Long-term use | No | No (toxic) | Yes |
| Flying | Contraindicated | N/A | Safe |
| N₂O anaesthesia | Contraindicated | Safe | Safe |
| Main complications | IOP ↑, cataract, pupil block | Retinal toxicity if retained | Glaucoma, cataract, emulsification |
Clinical Use: Tamponade Selection Guide
Uncomplicated posterior break (macular hole) → Air or SF₆
Superior breaks → SF₆ or C₃F₈ (gas)
Inferior breaks → Heavy SO (SO-PFA) or PFCL intraop then inferior gas
Complex PVR / cannot posture / needs to fly → Silicone oil
Giant retinal tear → PFCL intraop → C₃F₈ or SO
CMV retinitis detachment → SO + endolaser
Sources: Goodman & Gilman's Pharmacological Basis of Therapeutics, p. 1090–1104; Kanski's Clinical Ophthalmology 10th ed., pp. 699, 681–694
Coats disease
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Coats Disease
Definition
Coats disease is an idiopathic retinal telangiectasia characterized by anomalous retinal vessel development leading to intraretinal and subretinal exudation, and frequently exudative retinal detachment, without any signs of vitreoretinal traction. It is also described as a congenital vascular malformation of the retina with telangiectasis and aneurysm formation.
Epidemiology
- Age: Predominantly presents in the first decade of life (early childhood); may present at any age
- Sex: ~75% male
- Laterality: ~95% unilateral
- Inheritance: Not obviously inherited; idiopathic — but a genetic predisposition may exist. At least some patients have a somatic mutation in the NDP gene (the same gene mutated in Norrie disease)
- Leber miliary aneurysms: Previously considered a separate entity; now regarded as a milder, later-presenting form of the same disease with a better visual prognosis
- Younger children tend to have a more aggressive clinical course
Pathogenesis
Endothelial damage in anomalous retinal vessels → leakage of exudative lipoproteinaceous fluid and blood products into the subretinal space → progressive retinal thickening → exudative retinal detachment (no tractional component).
VEGF is thought to play a role in the exudative process, explaining why anti-VEGF agents show promise as adjunctive therapy.
Clinical Features
Symptoms
- Leukocoria (white pupillary reflex) — most common presenting feature
- Unilateral visual loss
- Strabismus (often first noticed by parents)
- Pain (with secondary glaucoma)

Fundus Signs
- Retinal telangiectasia and fusiform focal aneurysmal arteriolar dilatations — often initially in the inferior and temporal quadrants between the equator and ora serrata
- Intra- and subretinal exudates — characteristically affecting areas remote from the vascular abnormalities (lipid migrates to the macula = circinate exudation)
- Progression to extensive exudative retinal detachment
Complications (End-Stage Disease)
- Rubeosis iridis (iris neovascularization)
- Neovascular glaucoma
- Uveitis
- Cataract
- Phthisis bulbi (end-stage atrophy of the globe)
Investigations
Fluorescein Angiography (FA)
- Early (venous) phase: Hyperfluorescence of telangiectasis and aneurysmal dilatations
- Late phase: Extensive hyperfluorescence from leakage and staining
OCT
- Useful for macular assessment in cooperative older children
- Demonstrates intraretinal and subretinal fluid
Ultrasound (B-scan)
- Shows exudative retinal detachment without mass (helps exclude retinoblastoma)
- No calcification (contrast with retinoblastoma)
CT/MRI (Imaging)
- CT: Increased attenuation along the subretinal space or filling the entire vitreous cavity
- MRI: Increased T1 and T2 signal due to lipoproteinaceous material
- No contrast enhancement (distinguishes from retinoblastoma, which enhances)
Differential Diagnosis
The most critical differential — and the most dangerous to miss — is retinoblastoma.
| Condition | Key Distinguishing Features |
|---|---|
| Retinoblastoma | Calcification on CT/US; contrast enhancement on MRI; leukocoria; may be bilateral; family history; urgent referral mandatory |
| Familial exudative vitreoretinopathy (FEVR) | Bilateral; family history; peripheral retinal avascularity; no aneurysms |
| Retinopathy of prematurity (ROP) | History of prematurity; bilateral; temporal dragging of vessels |
| von Hippel–Lindau (retinal haemangioma) | Large feeding/draining vessels; systemic associations; bilateral |
| Persistent Hypertrophic Primary Vitreous (PHPV) | Microphthalmia; lens-to-retina fibrovascular band; no telangiectasia |
| Norrie disease | Bilateral; X-linked; associated with deafness and intellectual disability |
Key clinical rule: Any child with leukocoria or suspected Coats disease must have retinoblastoma excluded — this is a potentially life-threatening diagnosis.
Staging (Shields Classification)
| Stage | Description |
|---|---|
| 1 | Retinal telangiectasia only |
| 2A | Telangiectasia + exudation, extrafoveal |
| 2B | Telangiectasia + exudation, foveal involvement |
| 3A | Exudative retinal detachment, subtotal (3A1: extrafoveal; 3A2: foveal) |
| 3B | Total exudative retinal detachment |
| 4 | Total retinal detachment + glaucoma |
| 5 | Advanced end-stage disease (phthisis bulbi) |
Management
Treatment is tailored to stage and visual potential:
Observation
- Mild, non-vision-threatening disease
- Comfortable blind eye with total retinal detachment where no useful vision is recoverable
Laser Photocoagulation (Preferred)
- Ablation of telangiectatic/leaking vessels
- Indicated when progressive exudation is documented
- Multiple repeated treatments over extended time are commonly required
- Still preferred over cryotherapy when accessible
Anti-VEGF Therapy
- Limited studies but initial results promising — both as monotherapy and adjunct to laser
- Long-term safety in childhood not yet established
Intravitreal Triamcinolone (2–4 mg)
- Used with good effect in eyes with total exudative retinal detachment
- Reduces exudation and promotes retinal reattachment
Cryotherapy
- Double freeze-thaw method
- Used in eyes with extensive exudation or subtotal retinal detachment
- ⚠️ May cause marked inflammatory reaction with increased leakage — laser preferred if possible
Vitreoretinal Surgery
- For eyes with significant tractional preretinal fibrosis or total exudative detachment
- Poor visual prognosis but retinal reattachment may prevent neovascular glaucoma
Enucleation
- Reserved for painful eyes with neovascular glaucoma where no visual potential remains
Prognosis
- Highly variable — depends on severity at presentation and age
- Younger children → more aggressive course
- Vision is frequently severely compromised in advanced cases, particularly when the macula is involved with exudate at first presentation
- Treatment can stabilize the disease but rarely restores significantly reduced vision
Sources: Kanski's Clinical Ophthalmology 10th ed., pp. 566–570; Grainger & Allison's Diagnostic Radiology, p. 1554
Proliferative vitreoretinopathy
Finding Sources
Finding Sources
Reading File
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.