Give me details of coronary arteries anatomy
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
I now have rich, comprehensive content from multiple authoritative textbooks plus detailed anatomical images. I have enough to write a thorough, well-illustrated answer.
Coronary Artery Anatomy
The coronary arteries are the first branches of the aorta and provide the entire blood supply to the heart muscle. They arise from their respective sinuses of Valsalva, just above the aortic valve cusps, and course along the surface of the heart within the epicardial fat.
Overview - The Two Main Coronary Arteries
CT angiography reconstruction showing RCA, LAD, Circumflex (Cx), and Posterior Descending Artery (PDA):
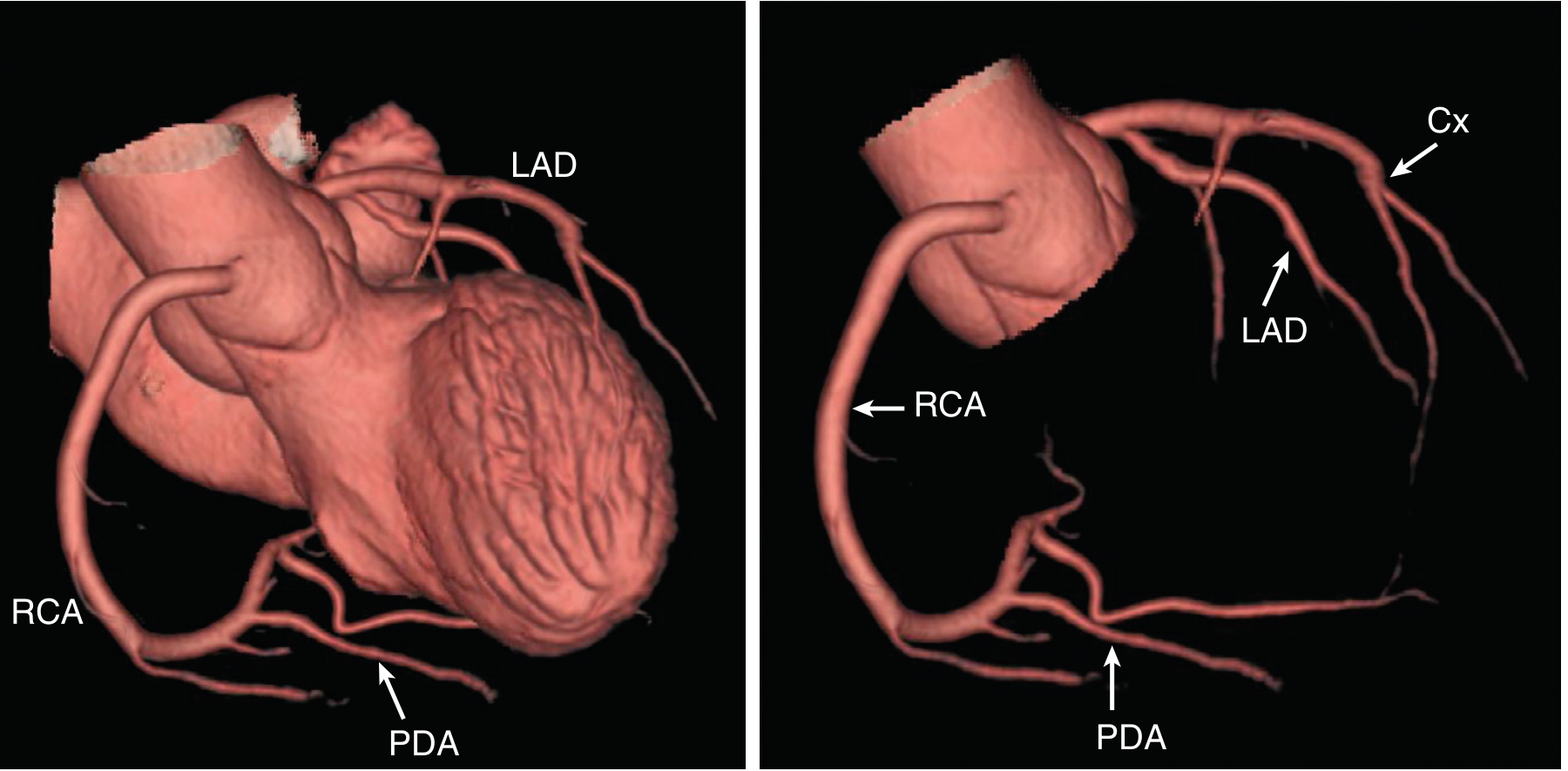
Fig. 8.1 from Textbook of Clinical Echocardiography - CT reconstruction showing normal coronary anatomy
1. Right Coronary Artery (RCA)
Origin: Arises from the right coronary sinus of Valsalva (right aortic sinus) of the ascending aorta. Its ostium averages 2-3 mm in diameter.
Course: Passes rightward and obliquely, entering the right atrioventricular (coronary) sulcus. It courses on the anterior surface of the heart supplying the right atrium and right ventricle, then continues in the coronary sulcus on the posterior surface, ultimately anastomosing with the left coronary artery at or near the crux cordis (junction of the interatrial and interventricular septa).
Main Branches of the RCA:
| Branch | Notes |
|---|---|
| Sinoatrial (SA) nodal branch | Ascending branch given off near the RCA origin; supplies the SA node in ~60% of people |
| Right marginal branch | Supplies the inferior border (acute margin) of the RV; does not typically reach the apex |
| Acute Marginal Artery (AMA) | Traverses the acute margin of the heart; supplies the lateral aspect of the RV; forms anastomoses at the apex with the LAD |
| Posterior Descending Artery (PDA) | Courses in the posterior interventricular groove; supplies both ventricles and the inferior 1/3 of the interventricular septum via septal perforating branches |
| AV Nodal Artery (AVNA) | Arises at the crux; supplies the AV node; originates from RCA in ~80% of people - compromise causes heart block/arrhythmias |
| Right posterolateral branch | Terminal bifurcation branch of the RCA along with the PDA |
2. Left Coronary Artery (LCA / Left Main)
Origin: Arises from the left coronary sinus of Valsalva. The left main trunk (LM) varies in length from a few mm to several cm. It courses posterolateral to the main pulmonary trunk for about 1 cm.
Division: The left main bifurcates (occasionally trifurcates with a ramus intermedius) into two principal branches:
A. Left Anterior Descending (LAD) Artery
- Takes an anterolateral course relative to the pulmonary trunk
- Runs in the anterior interventricular sulcus toward the apex, sometimes wrapping around the apex
- Supplies: Left ventricular free wall and the anterior 2/3 of the interventricular septum via septal perforating branches
- Often forms an anastomosis at the apex with the PDA (branch of RCA)
- Gives off diagonal branches (lateral branches) that course inferiorly on the anterior surface of the heart
B. Circumflex (Cx) Artery
- Follows the coronary sulcus laterally and posteriorly around the left border of the heart
- Terminates before reaching the crux in most people (in left-dominant circulation, it continues to give rise to the PDA)
- Gives off obtuse marginal branches that supply the lateral LV wall
- Gives off the SA nodal branch in ~40% of people (coursing on the posterior surface of the left atrium)
Detailed anatomy diagram showing all branches and the interventricular septum supply:
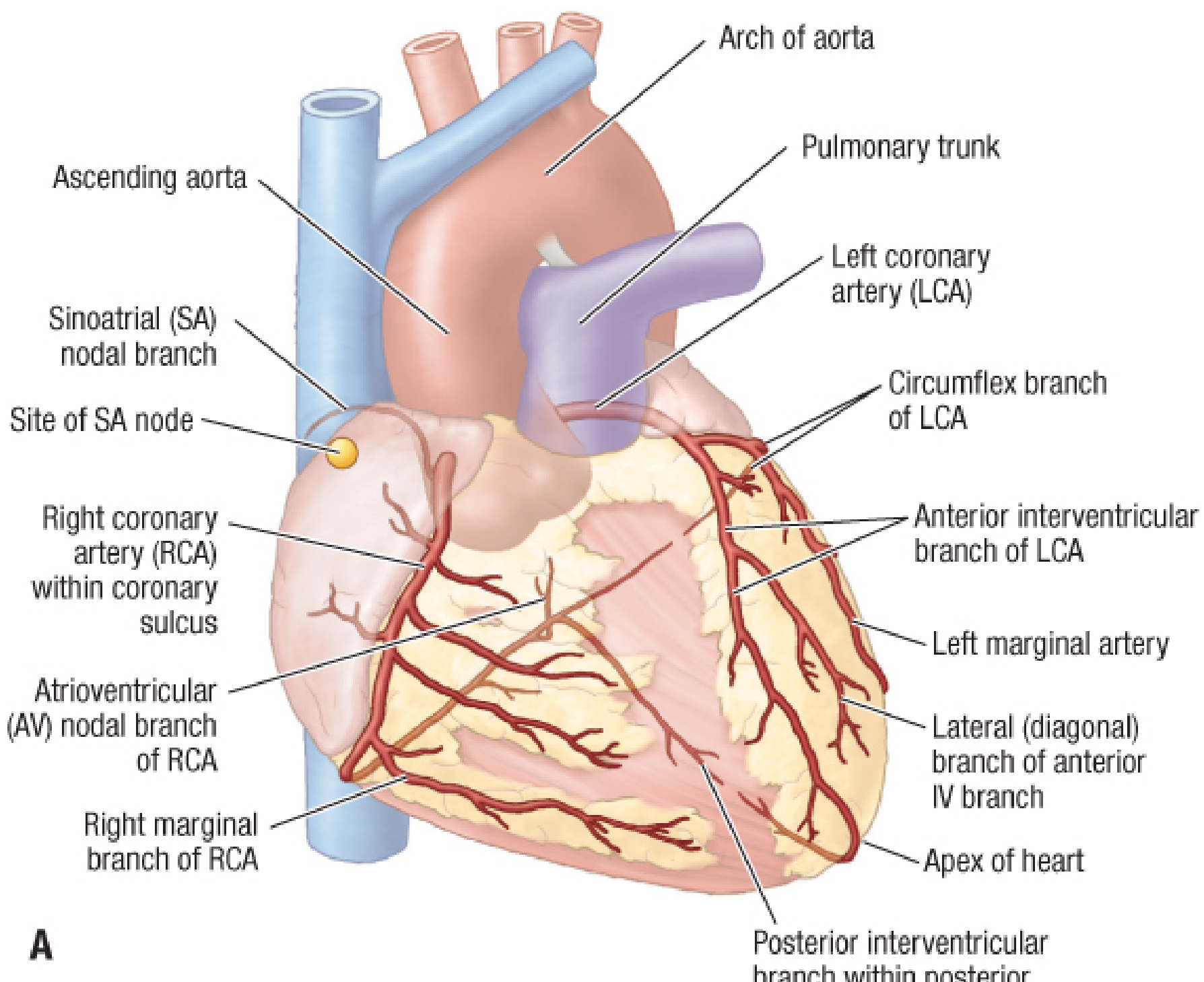
Figure 273.5A - Fischer's Mastery of Surgery: Coronary arteries, most common distribution pattern
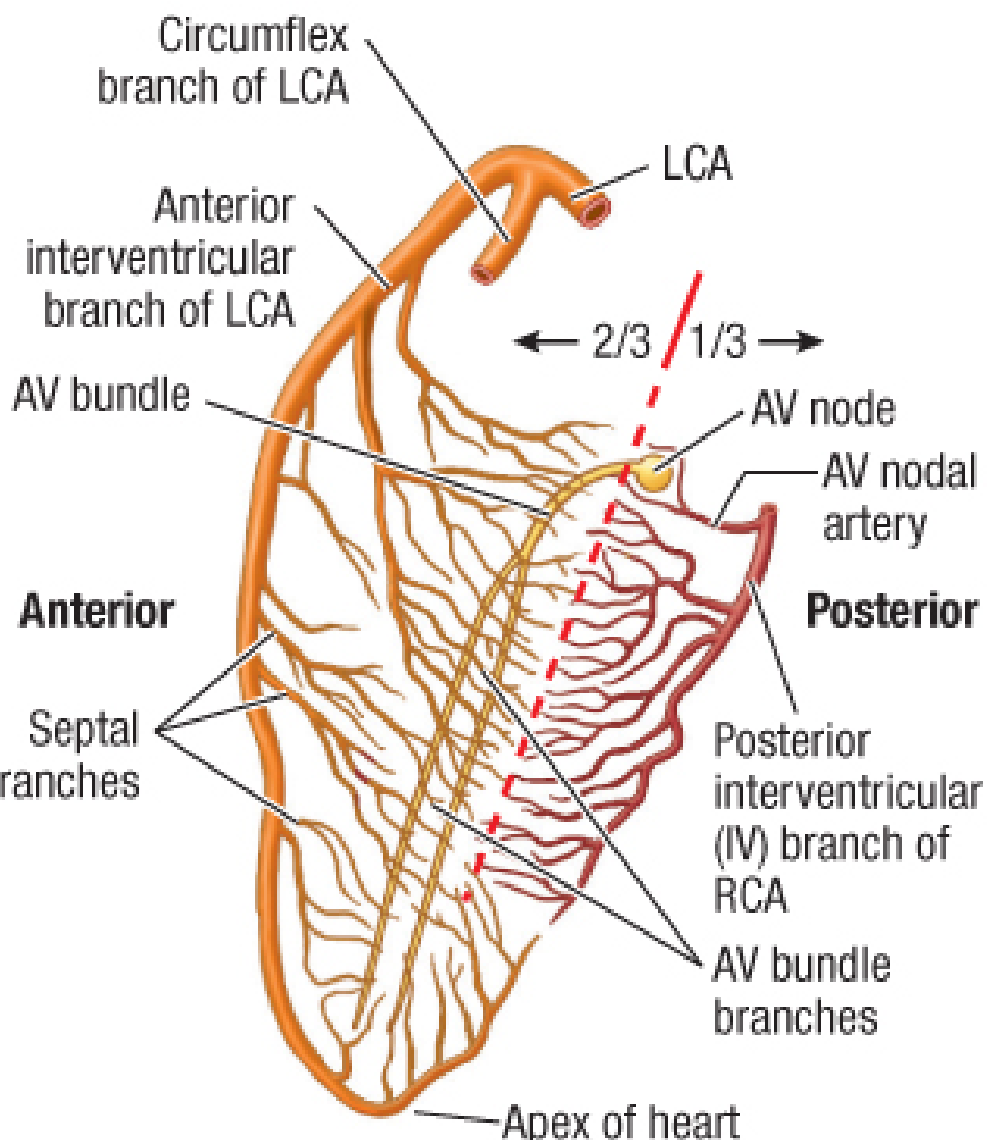
Figure 273.5C - Arteries supplying the interventricular septum: anterior 2/3 from LAD, posterior 1/3 from RCA
3. Coronary Dominance
Dominance is defined by which artery gives rise to the Posterior Descending Artery (PDA):
| Pattern | Frequency | Description |
|---|---|---|
| Right dominant | ~80-85% | RCA gives rise to the PDA |
| Left dominant | ~8-15% | Circumflex artery gives rise to the PDA |
| Co-dominant | ~7% | PDA arises from both RCA and LCA |
Coronary dominance patterns and myocardial supply territories:
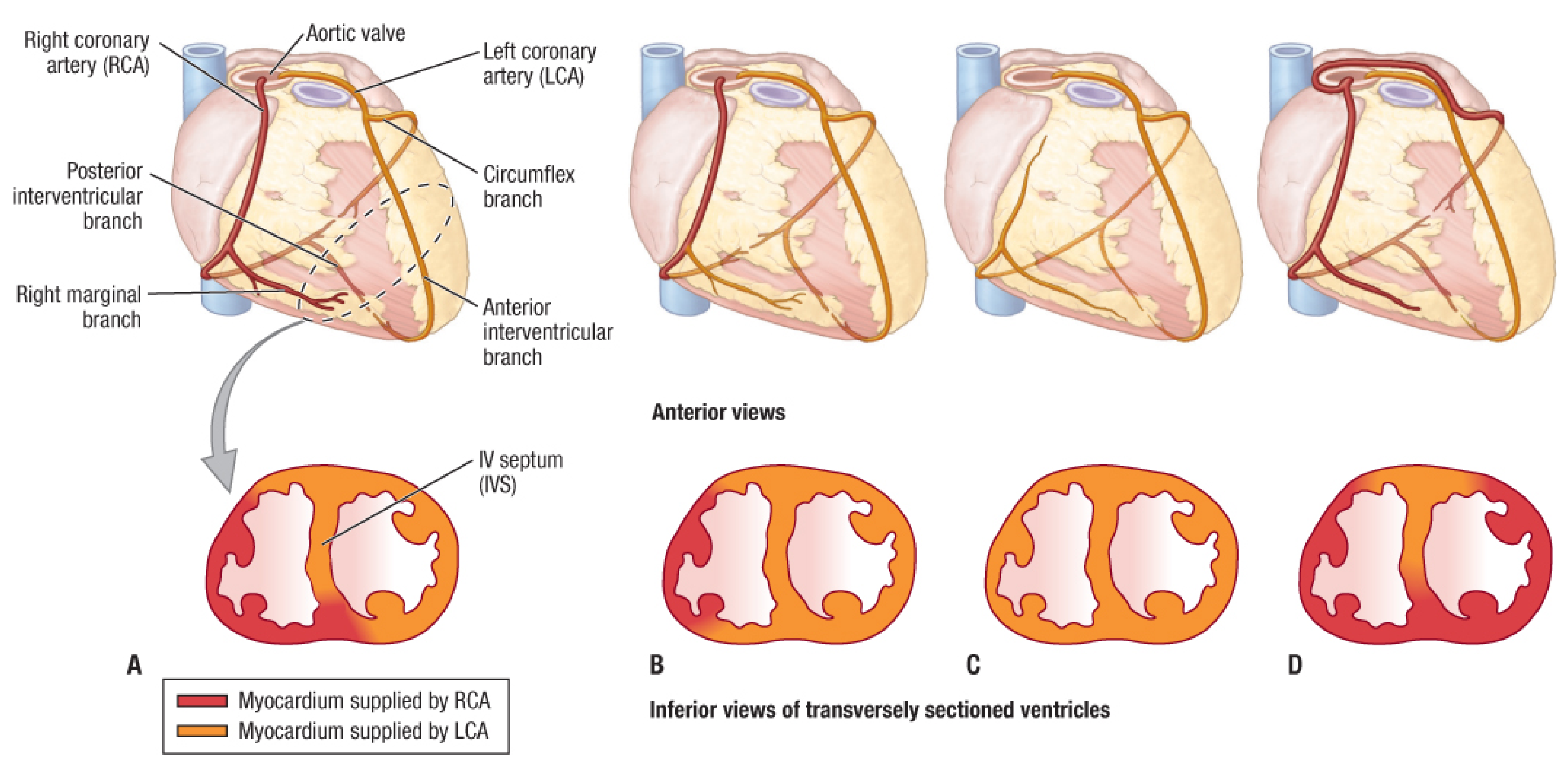
Fischer's Mastery: Variations in coronary distribution. A: Most common (67%), right dominant. B/C: Left coronary gives rise to posterior interventricular branch (15%). D: RCA replacing circumflex branch
4. Myocardial Territory of Each Artery
| Territory | Supplying Artery |
|---|---|
| Anterior LV wall | LAD (diagonal branches) |
| Anterior 2/3 of interventricular septum | LAD (septal perforators) |
| Inferior 1/3 of interventricular septum | PDA (from RCA in right-dominant) |
| Lateral LV wall | Obtuse marginals of Circumflex |
| Inferolateral (posterior) LV wall | Circumflex OM branches or RCA extensions |
| RV free wall | RCA (right marginal/acute marginal) |
| SA node | RCA (~60%), Circumflex (~40%) |
| AV node | RCA (~80%), Circumflex (~20%) |
| LV apex | Variable - LAD, PDA, or both |
5. Conduction System Supply
- SA Node: Supplied by the SA nodal branch of the RCA in ~60% of people and from the circumflex artery in ~40%
- AV Node: Supplied by the AV nodal artery (AVNA), arising from the RCA in ~80% of people at the crux cordis. This is why inferior MI (RCA territory) frequently causes AV block
- Bundle branches: The right bundle branch and anterior fascicle of the left bundle branch are supplied by LAD septal perforators; the posterior fascicle has dual supply from LAD and PDA
6. Key Anatomical Variants
- Ramus intermedius: A third branch of the left main (trifurcation) that runs between the LAD and Cx - occurs in ~20-30% of individuals
- Myocardial bridging: A segment of coronary artery (most often the mid-LAD) runs intramyocardially rather than epicardially; can cause systolic compression
- Single coronary artery: Rare anomaly - entire heart supplied from one ostium
- Anomalous origin from wrong sinus: Clinically significant if artery courses between the aorta and pulmonary trunk (risk of sudden death, especially with exercise)
Sources
- Textbook of Clinical Echocardiography, Ch. 8 (Coronary Artery Anatomy, p. 235)
- Fischer's Mastery of Surgery, 8th ed., Ch. 273 (Right Coronary Artery, Left Coronary Artery, pp. 7362-7364)
- Sabiston Textbook of Surgery, Ch. 26 (Coronary Artery Anatomy and Physiology, pp. 2989-2997)
This is a shared conversation. Sign in to Orris to start your own chat.