Stomach surgery
Reading File
Asking for Preferences
Asking for Preferences
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have rich, authoritative content from multiple surgical textbooks. Let me compile the comprehensive overview.
Stomach Surgery: Anatomy, Procedures & Surgical Technique
Gastric Anatomy Relevant to Surgery
The stomach is derived from the embryonic foregut and is one of the most well-vascularized organs in the body, protected by numerous extramural and intramural collateral vessels. It is divided into four anatomic regions:
| Region | Location |
|---|---|
| Cardia | Just distal to the gastroesophageal junction (GEJ) |
| Fundus | Above and to the left of the GEJ |
| Corpus (Body) | Between fundus and antrum |
| Antrum | Distal stomach, bounded by the pylorus |
The boundary between corpus and antrum is defined by a line from the incisura angularis (lesser curvature) to a point one-fourth the distance from the pylorus to the esophagus along the greater curvature.
Gastric Cell Types
| Cell Type | Location | Function |
|---|---|---|
| Parietal | Body | HCl secretion + intrinsic factor |
| Chief | Body | Pepsinogen |
| G cells | Antrum | Gastrin secretion |
| D cells | Antrum | Somatostatin |
| ECL cells | Body | Histamine |
| Surface epithelial | Diffuse | Mucus, bicarbonate, prostaglandins |
| Endocrine | Body | Ghrelin |
Vascular Anatomy
- Left gastric artery - arises from celiac trunk; supplies lesser curvature (ligated at its origin during gastrectomy)
- Right gastric artery - from hepatic artery; divides at hepatic artery origin during lymphadenectomy
- Short gastric arteries - from splenic artery; supply fundus (blood supply of proximal remnant after subtotal gastrectomy)
- Left gastroepiploic - from splenic artery
- Right gastroepiploic - from gastroduodenal artery
Major Gastric Surgical Procedures
1. Total Gastrectomy
Indication: Gastric cancer (especially proximal or diffuse), or tumors requiring >50% gastric removal.
Technique (Bailey & Love's, 28th Ed.):
- Long upper midline incision
- Stomach removed en bloc with entire greater and lesser omentum
- Duodenum divided with surgical stapler just distal to pylorus
- Hepatic, subpyloric, suprapyloric, left gastric, and splenic artery nodal chains dissected
- Esophagus divided with >5 cm clearance from tumor (frozen section of margins)
Reconstruction - Roux-en-Y esophagojejunostomy:
- Roux (alimentary) limb must be at least 50 cm to prevent bile reflux esophagitis
- Esophagojejunostomy performed with circular stapler (purse-string suture in esophageal stump, introduced through blind end of Roux loop)
- End-to-side jejunojejunostomy created distally
- Roux loop placed antecolic or retrocolic
Lymphadenectomy extent:
- D1: Perigastric nodes only
- D2: Clearance of major arterial trunks (standard in specialist centers); spleen and pancreas conserved where possible; station 10 nodes often spared
Bailey and Love's Short Practice of Surgery, 28th Ed.
2. Subtotal (Distal) Gastrectomy
Indication: Distal gastric tumors; peptic ulcer disease not responding to medical management.
Technique:
- Similar to total gastrectomy distally, but proximal stomach is preserved
- Blood supply to remnant derived from short gastric arteries
- Preferred reconstruction: Roux-en-Y gastrojejunostomy (reduces bile reflux vs. Billroth II/Polya)
- Billroth II is still used but associated with enterogastric reflux and bile reflux esophagitis
3. Proximal Gastrectomy
Indication: Smaller tumors near the GEJ; patients with less physiologic reserve; T1 tumors of upper stomach.
Key considerations (Current Surgical Therapy, 14th Ed.):
- Oncologic outcomes equivalent to total gastrectomy for appropriately selected cases
- Preferred only if >50% of stomach can be preserved; if <50% remains, total gastrectomy is preferred (bile reflux negates benefit)
- Diaphragm divided by electrocautery in midline, crura retracted laterally to mobilize distal esophagus
- Primary esophagogastrostomy end-to-side over a nasogastric tube, left overnight
- Anastomosis lies in the low mediastinum after diaphragm reapproximation
4. Pylorus-Preserving Gastrectomy
Indication: Early gastric cancer (T1N0M0) in the middle-third of the stomach, located at least 4 cm from the pylorus.
- Primarily performed in Japan and Korea
- Balance between quality-of-life preservation and adequate oncologic resection
- Ongoing trials to define ideal patient selection
5. Sleeve Gastrectomy (Bariatric)
Indication: Morbid obesity (BMI ≥40, or ≥35 with comorbidities).
Technique (Bailey & Love's, 28th Ed.):
- Lesser curve-based gastric tube created over a size 32-36 Fr bougie (some surgeons use larger to reduce leak risk)
- Linear stapling devices used to resect the fundus and lateral body
- Variations exist in stapler width and use of reinforcement strips
- Critical risk point: Staple line leak at the angle of His (high-pressure system due to intact pylorus; can take months to heal)
Mechanism of action:
- Initially thought purely restrictive; now known that gastric emptying is accelerated (not delayed) after sleeve
- Changes in satiety gut hormones (PYY, GLP-1) and bile salt metabolism play major roles
- Long-term: risk of symptomatic GERD and de novo Barrett's esophagus; weight regain may require revisional surgery
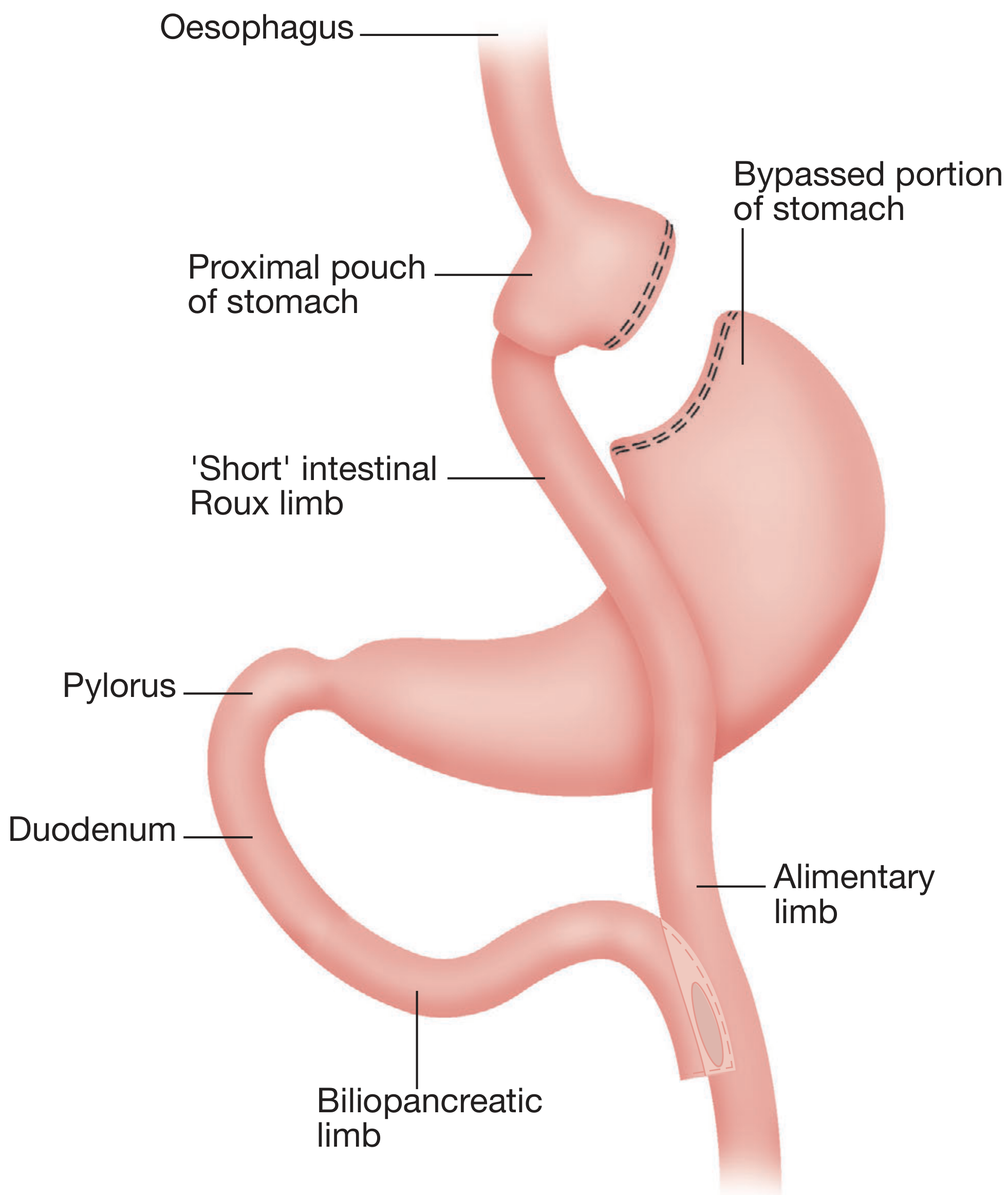
6. Roux-en-Y Gastric Bypass (RYGB)
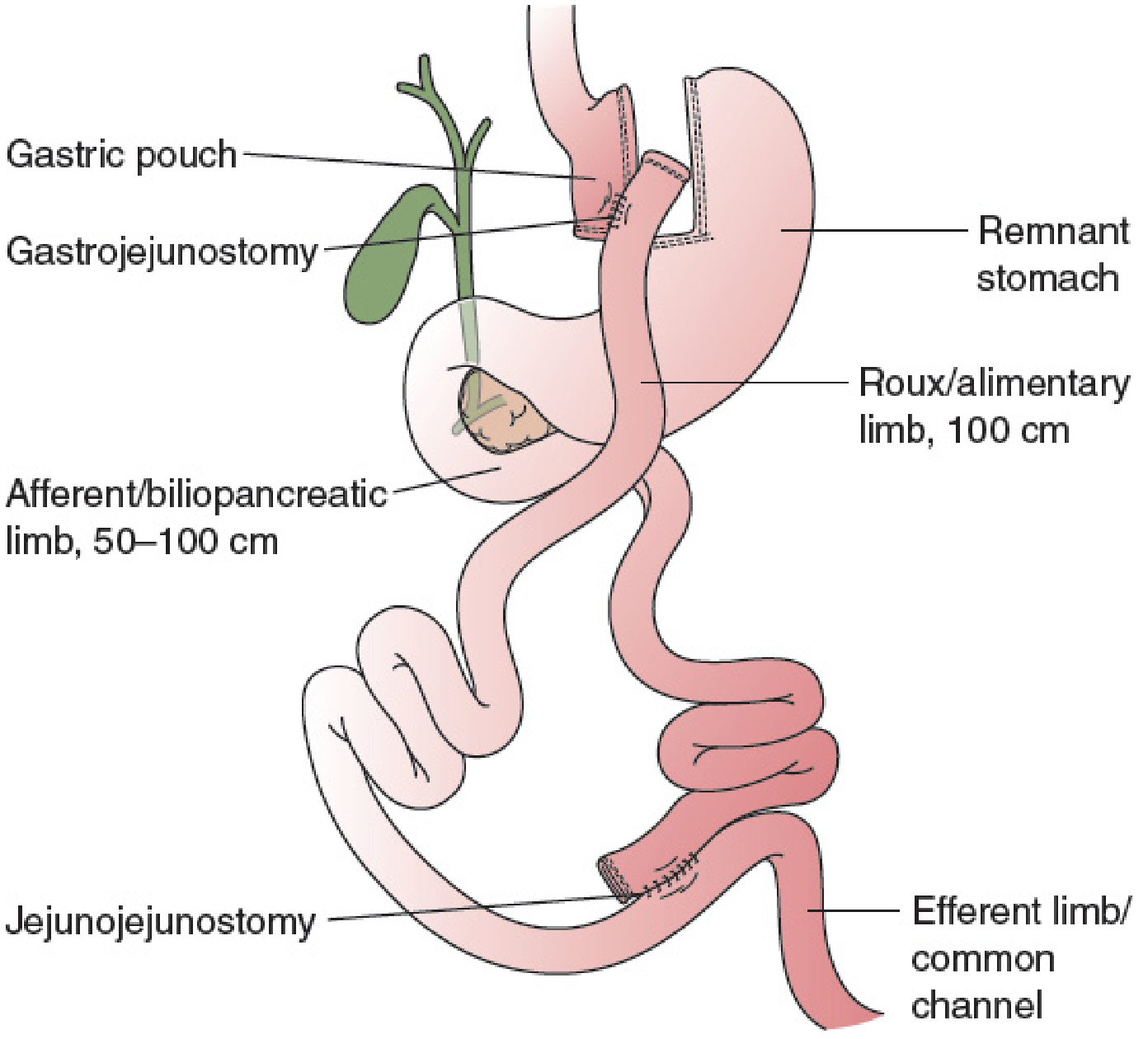
Technique:
- Short vertical lesser curvature-based gastric pouch created
- Pouch-jejunostomy options: linear stapler with suture closure, circular stapler, or hand-sewn
- Leak test is routine
- Roux (alimentary) limb: 100-150 cm (antecolic or retrocolic)
- Biliopancreatic (afferent) limb: Kept short (50-100 cm) to reduce vitamin/mineral deficiencies
- Bowel continuity restored by Y-jejunojejunostomy (stapled or hand-sewn)
- Remnant stomach left in place but bypassed (not removed)
Mechanism: Complex - appetite reduction via changes in satiety hormones, altered energy expenditure, and changed food preferences. Roux-en-Y reconstruction prevents bile reflux compared to loop reconstruction.
7. One-Anastomosis Gastric Bypass (OAGB / "Mini-Gastric Bypass")
First described by Rutledge.
- Single anastomosis (antecolic loop gastrojejunostomy) - no Roux-en-Y configuration
- Longer gastric pouch than standard RYGB
- Technically less demanding with similar weight loss outcomes
- Concerns: Symptomatic biliary reflux causing gastritis/esophagitis, marginal ulcers, possible increased risk of Barrett's esophagus and gastric/esophageal cancer with long-term biliary reflux - outcomes still under investigation
8. Adjustable Gastric Banding (AGB)
- Band placed just below the GEJ via pars flaccida technique (through lesser omentum window)
- Creates a small "virtual" gastric pouch
- Sutured anteriorly with gastrogastric tunnelling sutures to prevent slippage
- Access port fixed to rectus sheath (upper abdomen) for band adjustments via Huber needle
- Declining in use due to long-term complications and inferior weight loss vs. RYGB and sleeve
9. Biliopancreatic Diversion / Duodenal Switch (BPD-DS)
Technique:
- Sleeve gastrectomy + division of duodenum distal to pylorus
- Duodenojejunostomy (maintains pylorus in alimentary stream)
- Distal Roux-en-Y jejunoileostomy with 100 cm common channel
- Greatest weight loss of all bariatric procedures
Limitations: Higher perioperative mortality (at least 2x vs. RYGB by meta-analysis), significant malabsorptive complications (2-20%), technically demanding duodenojejunal anastomosis. Currently comprises <2% of bariatric operations; often reserved as a revisional option after failed sleeve gastrectomy.
Advanced & Multivisceral Resection
For locally advanced gastric adenocarcinoma invading adjacent organs, en bloc multivisceral resection is required (may include distal pancreatectomy-splenectomy or pancreaticoduodenectomy). Despite higher morbidity, achieving an R0 resection provides significant survival benefit over palliative approaches.
In highly selected patients with low peritoneal disease (peritoneal cancer index ≤7), cytoreductive surgery (CRS) + HIPEC (hyperthermic intraperitoneal chemotherapy with mitomycin C) combined with gastrectomy and lymphadenectomy has shown a median overall survival of 2.1 years from diagnosis in phase II trials.
Summary Comparison
| Procedure | Primary Indication | Reconstruction | Key Technical Point |
|---|---|---|---|
| Total gastrectomy | Proximal/diffuse gastric Ca | Roux-en-Y esophagojejunostomy | ≥50 cm Roux limb; D2 lymphadenectomy |
| Subtotal gastrectomy | Distal gastric Ca / PUD | Roux-en-Y gastrojejunostomy | Preferred over Billroth II |
| Proximal gastrectomy | Small GEJ tumors | Esophagogastrostomy | Only if >50% stomach preserved |
| Sleeve gastrectomy | Obesity | None (no anastomosis) | 32-36 Fr bougie; leak at angle of His |
| RYGB | Obesity | Roux-en-Y gastrojejunostomy | Roux limb 100-150 cm |
| OAGB | Obesity | Loop gastrojejunostomy | Simpler but biliary reflux risk |
| BPD-DS | Severe obesity / revision | Duodenojejunostomy + Roux | Highest weight loss; highest morbidity |
| Gastric banding | Obesity | None | Declining use |
Sources: Bailey and Love's Short Practice of Surgery 28th Ed. | Current Surgical Therapy 14th Ed. | Mulholland and Greenfield's Surgery 7th Ed. | Sabiston Textbook of Surgery | Yamada's Textbook of Gastroenterology 7th Ed.
Abg
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
I now have comprehensive, authoritative content from multiple textbooks. Here is the full guide:
Arterial Blood Gas (ABG) - Complete Guide
What is an ABG?
An arterial blood gas is a sample of blood drawn from an artery (usually the radial artery) that measures the body's acid-base status, ventilation, and oxygenation simultaneously. The pH of blood summarizes systemic acid-base balance and is the negative logarithm of hydrogen-ion concentration ([H+]).
The relationship between the key parameters is described by the Henderson-Hasselbalch equation:
pH = pK + log₁₀ ([HCO₃⁻] / [0.03 × PaCO₂])
The kidneys regulate plasma bicarbonate (HCO₃⁻), and the lungs regulate PaCO₂. Together they maintain a normal pH of 7.35-7.45.
Normal ABG Values
| Parameter | Normal Value | Normal Range |
|---|---|---|
| pH | 7.40 | 7.35 - 7.45 |
| PaCO₂ | 40 mmHg | 38 - 42 mmHg |
| PaO₂ | 100 mmHg | 75 - 100 mmHg |
| HCO₃⁻ | 24 mEq/L | 22 - 26 mEq/L |
| Base Excess | 0 | -4 to +4 |
| SaO₂ | >95% | - |
Key: Calculated HCO₃⁻ on the ABG and measured serum HCO₃⁻ (from electrolytes) should be within 2-3 mEq/L of each other. A larger discrepancy suggests a lab error or non-simultaneous sampling.
Step-by-Step ABG Interpretation
Step 1 - Assess pH
| pH | Interpretation |
|---|---|
| < 7.35 | Acidemia |
| 7.35 - 7.45 | Normal |
| > 7.45 | Alkalemia |
Step 2 - Identify the Primary Process
| pH | PaCO₂ | HCO₃⁻ | Disorder |
|---|---|---|---|
| ↓ | ↑ | Normal/↑ | Respiratory acidosis |
| ↓ | ↓ | ↓ | Metabolic acidosis |
| ↑ | ↓ | Normal/↓ | Respiratory alkalosis |
| ↑ | ↑ | ↑ | Metabolic alkalosis |
Rule: In respiratory disorders, PaCO₂ and pH move in opposite directions. In metabolic disorders, PaCO₂ moves in the same direction as pH (as compensation).
Step 3 - Check for Appropriate Compensation
Use the compensation formulas to decide if the secondary change is appropriate (simple disorder) or excessive/inadequate (mixed disorder):
| Primary Disorder | Expected Compensation Formula |
|---|---|
| Metabolic acidosis | PaCO₂ = 1.5 × [HCO₃⁻] + 8 ± 2 (Winter's Formula) |
| Metabolic alkalosis | PaCO₂ = 0.7 × [HCO₃⁻] + 20 ± 5 |
| Acute respiratory acidosis | ↑ HCO₃⁻ = ΔPaCO₂ / 10 |
| Chronic respiratory acidosis | ↑ HCO₃⁻ = 4 × (ΔPaCO₂ / 10) |
| Acute respiratory alkalosis | ↓ HCO₃⁻ = 2 × (ΔPaCO₂ / 10) |
| Chronic respiratory alkalosis | ↓ HCO₃⁻ = 5 × (ΔPaCO₂ / 10) |
If the measured value differs from the expected, a secondary (mixed) acid-base disorder is present.
Step 4 - Calculate the Anion Gap (AG)
AG = [Na⁺] - ([Cl⁻] + [HCO₃⁻]) Normal AG < 12-13 mEq/L
Always calculate the AG even if a metabolic acidosis is not obvious - it can unmask a hidden mixed disorder.
Albumin correction: Because albumin is a major unmeasured anion, the AG must be corrected when albumin is low:
Corrected AG = Observed AG + 2.5 × (4.0 - [measured albumin])
Step 5 - If Normal AG Acidosis, Check Urine Anion Gap
Urine AG = Urine [Na⁺] + [K⁺] - [Cl⁻]
- Negative urine AG → GI loss of bicarbonate (e.g., diarrhea)
- Positive urine AG → Renal loss (e.g., RTA)
Step 6 - If High AG Acidosis, Calculate Delta-Delta Ratio (Δ/Δ)
Δ/Δ = (AG - 12) / (24 - HCO₃⁻)
| Ratio | Interpretation |
|---|---|
| 1 - 2 | Pure high AG metabolic acidosis |
| < 1 | Concurrent non-AG metabolic acidosis |
| > 2 | Concurrent metabolic alkalosis OR compensated chronic respiratory acidosis |
Step 7 - Assess Oxygenation
Check PaO₂ and calculate the A-a gradient:
A-a gradient = PAO₂ - PaO₂ where PAO₂ = (FiO₂ × 713) - (PaCO₂ / 0.8)
Normal A-a gradient (on room air) ≈ Age/4 mmHg
| A-a Gradient | Implication |
|---|---|
| Normal | Hypoventilation is the cause of hypoxemia |
| Elevated | V/Q mismatch, diffusion impairment, or shunt |
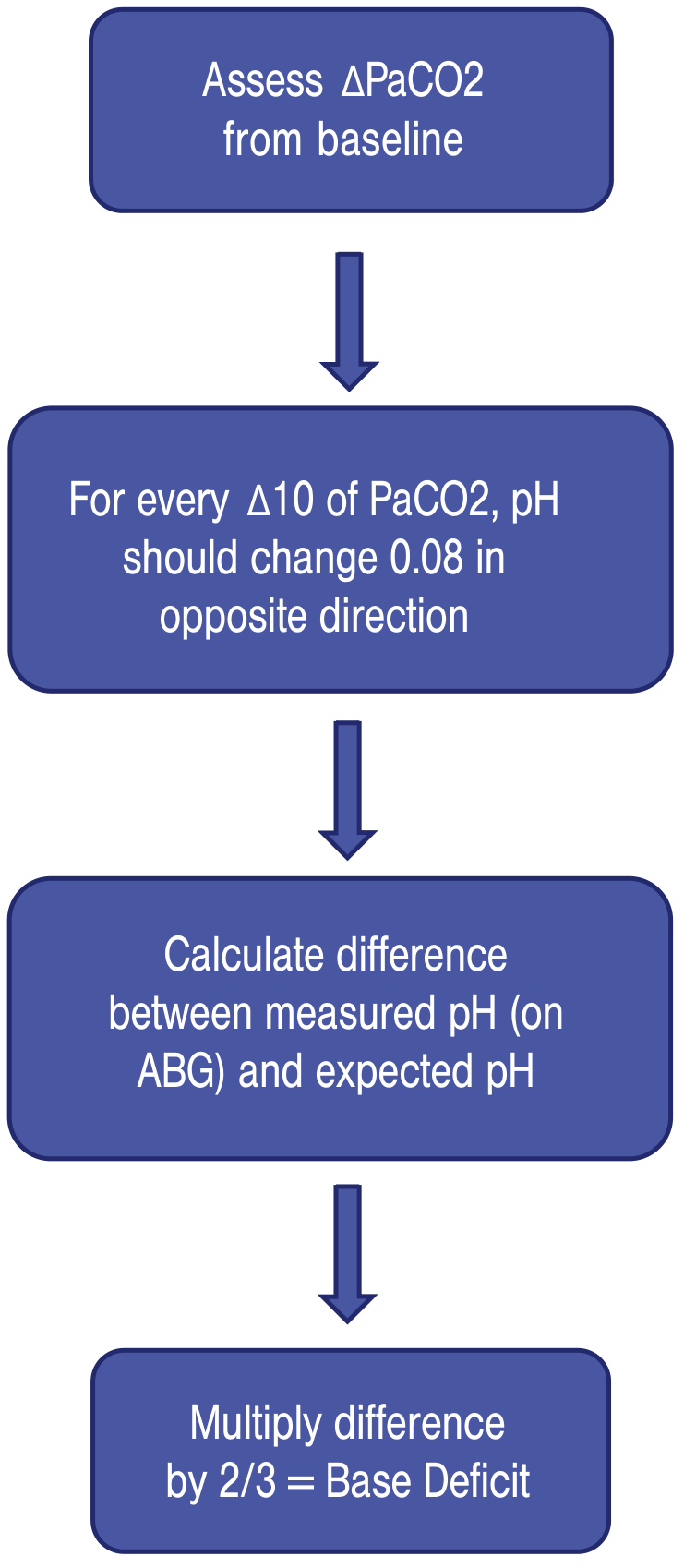
Base Deficit/Excess
Base excess = amount of base needed to titrate 1 L of blood to pH 7.4 at 37°C.
- > +4 = metabolic alkalosis
- < -4 = metabolic acidosis (base deficit)
The Four Primary Disorders
1. Metabolic Acidosis
Definition: pH ↓, HCO₃⁻ ↓, PaCO₂ ↓ (compensation)
High Anion Gap Metabolic Acidosis - Mnemonic: MUDPILES
| Letter | Cause |
|---|---|
| M | Methanol |
| U | Uremia |
| D | Diabetic ketoacidosis (DKA) |
| P | Paraldehyde / Propylene glycol / Paracetamol (acetaminophen) |
| I | Iron / Isoniazid |
| L | Lactic acidosis (most common cause of high AG metabolic acidosis) |
| E | Ethylene glycol |
| S | Salicylates |
Normal Anion Gap Metabolic Acidosis - Mnemonic: HARDUP
| Letter | Cause |
|---|---|
| H | Hyperalimentation / Hospital-acquired saline |
| A | Acid infusion / Addison's disease / Acetazolamide |
| R | Renal tubular acidosis (RTA) |
| D | Diarrhea |
| U | Ureterosigmoidostomy |
| P | Pancreatic drainage / fistula |
Treatment: Target underlying cause. NaHCO₃ is given to raise pH >7.10 in severe acidosis, or >7.20 in severe metabolic acidosis with concurrent AKI.
2. Metabolic Alkalosis
Definition: pH ↑, HCO₃⁻ ↑, PaCO₂ ↑ (compensation)
Chloride-Responsive (urine Cl⁻ < 25 mmol/L - corrects with saline)
- Nasogastric suction
- Vomiting
- Chloride-wasting diarrhea
- Villous adenoma
- Diuretic use
Chloride-Unresponsive (urine Cl⁻ > 40 mmol/L - does NOT correct with saline)
- Primary hyperaldosteronism
- Secondary hyperaldosteronism (Bartter syndrome, Gitelman syndrome, CHF, liver failure)
- Cushing disease / exogenous steroids
- Severe hypercalcemia or hypomagnesemia
- Bicarbonate ingestion
- Licorice overdose (glycyrrhizic acid)
Treatment: Chloride-responsive: IV normal saline. Chloride-unresponsive: treat the underlying hormone/electrolyte disorder.
3. Respiratory Acidosis
Definition: pH ↓, PaCO₂ ↑ (>40 mmHg), HCO₃⁻ ↑ (compensation)
Mechanism: Inadequate CO₂ clearance or CO₂ overproduction.
Causes:
- Lung/airway disease: Airway obstruction, COPD, pneumothorax, pleural effusion, pulmonary edema, pneumonia
- Chest wall disease: Flail chest, obesity hypoventilation syndrome
- Respiratory muscle weakness: Myopathies, Guillain-Barré, hypokalemia, hypophosphatemia
- Decreased respiratory drive: Intracranial mass/hemorrhage, sedatives, narcotics, anesthesia
Treatment:
- Increase minute ventilation (↑ tidal volume × respiratory rate on ventilator)
- Noninvasive ventilation (BiPAP) for COPD exacerbation or heart failure
- If no improvement in 2 hours: proceed to invasive ventilation
- Severe cases: VV-ECMO as salvage modality
- Caution: Do not overcorrect a patient with chronically elevated baseline PaCO₂ - can cause cerebral ischemia and ventilator weaning difficulty
4. Respiratory Alkalosis
Definition: pH ↑, PaCO₂ ↓ (<40 mmHg), HCO₃⁻ ↓ (compensation)
Mechanism: Rate of CO₂ elimination exceeds production (hyperventilation).
Causes:
- Anxiety / pain / agitation
- Fever, sepsis
- Salicylate toxicity (classically causes respiratory alkalosis FIRST, then anion gap metabolic acidosis)
- Pulmonary embolism, pneumothorax, pneumonia
- Brain tumor / intracranial lesion
- Pregnancy, liver failure, heart failure
- High altitude
- Drugs: salicylates, catecholamines, progesterone
Symptoms of acute respiratory alkalosis (from hypocalcemia due to increased Ca²⁺-albumin binding):
- Lip and extremity paresthesias
- Carpal-pedal spasm
- Muscle cramps, syncope
Treatment: Treat the underlying cause. On a ventilator, inducing mild respiratory alkalosis can be used temporarily as an adjunct for refractory acidosis or traumatic brain injury.
Mixed Acid-Base Disorders
Mixed disorders occur when two or more primary disorders are present simultaneously. Clues:
- pH is normal but AG is elevated
- Compensation is greater or lesser than expected by the formulas
- Clinical context (e.g., patient on diuretics with poor perfusion = metabolic alkalosis + metabolic acidosis from lactic acidosis)
Oxygenation Assessment from ABG
| Condition | PaO₂ | A-a Gradient | Cause |
|---|---|---|---|
| Normal | 75-100 | Normal | - |
| Hypoventilation | ↓ | Normal | Neuromuscular, CNS, sedation |
| V/Q mismatch | ↓ | Elevated | COPD, PE, interstitial lung disease |
| Diffusion impairment | ↓ | Elevated | Pulmonary edema, ILD |
| Shunt | ↓ | Elevated | Does NOT correct with O₂ |
V/Q mismatch responds to supplemental O₂. True shunt (intracardiac, consolidated lung) does not correct with oxygen.
Quick Reference Summary
pH < 7.35 → Acidemia
PaCO₂ ↑ → Respiratory acidosis
HCO₃⁻ ↓ → Metabolic acidosis → Check AG
AG ↑ → MUDPILES
AG normal → HARDUP → Check urine AG
pH > 7.45 → Alkalemia
PaCO₂ ↓ → Respiratory alkalosis
HCO₃⁻ ↑ → Metabolic alkalosis → Check urine Cl⁻
Cl⁻ < 25 → Chloride-responsive (give saline)
Cl⁻ > 40 → Chloride-unresponsive (treat cause)
Always check compensation with formulas - mismatch = mixed disorder
Always calculate AG - even with normal pH
Sources: Current Surgical Therapy 14th Ed. | Barash Clinical Anesthesia 9th Ed. | Rosen's Emergency Medicine | Mulholland & Greenfield's Surgery 7th Ed. | Washington Manual of Medical Therapeutics
This is a shared conversation. Sign in to Orris to start your own chat.