Increase Aptt and reduced platelet
Reading File
search_medical_text
elevated aPTT thrombocytopenia causes differential diagnosis
search_medical_text
prolonged aPTT low platelets coagulopathy DIC heparin antiphospholipid
GradeResponse
GradeResponse
Here is a structured overview of conditions that cause both prolonged aPTT and reduced platelets (thrombocytopenia):
Causes of Increased aPTT + Thrombocytopenia
1. Disseminated Intravascular Coagulation (DIC)
The classic combined coagulopathy.
| Lab Finding | Result |
|---|---|
| aPTT | Prolonged |
| PT | Prolonged |
| Platelets | Low |
| Fibrinogen | Low |
| D-dimer / FDP | Elevated |
Mechanism: Systemic activation of coagulation consumes clotting factors (prolonging aPTT) and platelets simultaneously.
Triggers:
- Sepsis (most common)
- Trauma / burns
- Obstetric emergencies (abruption, amniotic fluid embolism, dead fetus syndrome)
- Acute promyelocytic leukemia (APL / AML-M3)
- Malignancy (solid tumors)
- Transfusion reactions
(Harrison's, p. 3481–3482)
2. Heparin Therapy + Heparin-Induced Thrombocytopenia (HIT)
- Heparin directly prolongs aPTT (its intended action)
- HIT (Type II): immune-mediated platelet destruction via anti-PF4/heparin antibodies → thrombocytopenia (typically 50% drop from baseline, days 5–10 of therapy)
- Paradoxically pro-thrombotic despite low platelets
3. Antiphospholipid Syndrome (APS)
- aPTT is paradoxically prolonged in vitro (lupus anticoagulant interferes with phospholipid-dependent clotting assays) — yet the patient is pro-thrombotic
- Thrombocytopenia occurs in ~20–40% of cases (immune-mediated platelet destruction)
- Associated with: SLE, recurrent thrombosis, recurrent miscarriages
- Key test: mixing study (aPTT does NOT correct), confirm with dilute Russell viper venom time (dRVVT)
4. Severe Liver Disease
- Mechanism: Reduced synthesis of all clotting factors (prolonged aPTT) + platelet sequestration from portal hypertension/hypersplenism
- Unlike DIC, lab parameters change slowly (helpful distinguishing feature)
- D-dimer may be mildly elevated
- (Harrison's, p. 3481)
5. Thrombotic Thrombocytopenic Purpura (TTP)
- Thrombocytopenia is prominent (microangiopathic platelet consumption)
- aPTT/PT are usually normal in classic TTP, but can be prolonged in severe cases
- Key features: microangiopathic hemolytic anemia (MAHA), schistocytes on smear, neurological symptoms, renal impairment, fever
- ADAMTS13 activity markedly reduced (<10%)
- (Harrison's, p. 3481)
6. Massive Transfusion / Dilutional Coagulopathy
- Large-volume crystalloid or pRBC transfusion dilutes clotting factors → prolonged aPTT
- Dilutes platelets → thrombocytopenia
- Manage with FFP, cryoprecipitate, and platelet transfusion (1:1:1 protocol in trauma)
7. Factor Deficiencies Affecting the Intrinsic Pathway
Isolated aPTT prolongation with thrombocytopenia in context of:
- Hemophilia A or B + concurrent ITP or bone marrow failure
- Less common; usually context makes it clear
Diagnostic Approach
Prolonged aPTT + Low Platelets
|
├─ Check PT, fibrinogen, D-dimer
| ├─ All abnormal → DIC
| └─ Normal PT → consider APS, HIT, liver disease
|
├─ Mixing study
| ├─ Corrects → factor deficiency
| └─ Does NOT correct → inhibitor (lupus anticoagulant, factor inhibitor)
|
├─ On heparin? → Check anti-PF4 antibody (4T score for HIT)
|
├─ Schistocytes on smear? → TTP / HUS
|
└─ Chronic liver disease? → LFTs, imaging
Quick Reference Table
| Condition | aPTT | PT | Platelets | Fibrinogen | D-dimer | Key Feature |
|---|---|---|---|---|---|---|
| DIC | ↑ | ↑ | ↓ | ↓ | ↑↑ | Consumptive coagulopathy |
| APS / Lupus anticoagulant | ↑ | Normal | ↓ | Normal | Variable | Mixing study doesn't correct |
| HIT | ↑ (if on heparin) | Normal | ↓ | Normal | Normal | Anti-PF4 Ab positive |
| Liver disease | ↑ | ↑ | ↓ | ↓ | Mildly ↑ | Slow progression |
| TTP | Usually normal | Normal | ↓↓ | Normal | Normal | Schistocytes, ADAMTS13 ↓ |
| Massive transfusion | ↑ | ↑ | ↓ | ↓ | Variable | Transfusion history |
The most urgent diagnosis to exclude is DIC — it requires immediate treatment of the underlying cause plus supportive replacement of clotting factors and platelets.
Inr increase in
search_medical_text
elevated INR increased prothrombin time causes differential diagnosis
search_medical_text
prolonged PT INR liver disease vitamin K deficiency warfarin coagulopathy
GradeResponse
GradeResponse
Causes of Increased INR (Prolonged PT)
INR reflects the extrinsic and common coagulation pathways — it measures factors I (fibrinogen), II, V, VII, IX, and X. Factors II, VII, IX, and X are vitamin K-dependent.
Major Categories
1. Liver Disease
The most common cause of elevated INR in clinical practice.
- Mechanism: Hepatocytes synthesize all coagulation factors; hepatocellular dysfunction reduces factor production
- Seen in: hepatitis (acute/chronic), cirrhosis, acute liver failure, fatty liver disease
- PT prolonged >5 s above control that does not correct with parenteral vitamin K = poor prognostic sign in acute hepatitis
- INR is a component of the MELD score (along with bilirubin and creatinine) — used to assess severity of hepatic decompensation and liver transplant allocation
- (Harrison's, p. 9331)
2. Vitamin K Deficiency
- Mechanism: Factors II, VII, IX, X require vitamin K for gamma-carboxylation (activation)
- Causes:
- Malabsorption: fat malabsorption (Crohn's, celiac disease, short bowel syndrome)
- Cholestasis / Obstructive jaundice: bile salts needed for vitamin K (fat-soluble) absorption
- Poor dietary intake (prolonged fasting, malnutrition, ICU patients on antibiotics)
- Broad-spectrum antibiotics eliminating gut flora (which produce vitamin K2)
- Neonates (physiologic vitamin K deficiency → hemorrhagic disease of the newborn)
- Key test: INR corrects after IV/SC vitamin K administration → confirms deficiency
- (Evaluation of Abnormal Liver Chemistries, p. 4)
3. Anticoagulant Therapy
| Drug | Mechanism |
|---|---|
| Warfarin | Vitamin K antagonist → blocks activation of II, VII, IX, X |
| Heparin (bolus) | Potentiates antithrombin III → can prolong PT |
| Direct oral anticoagulants (DOACs) | Rivaroxaban/apixaban (anti-Xa) and dabigatran (anti-IIa) — variable effect on PT |
4. Disseminated Intravascular Coagulation (DIC)
- Consumptive coagulopathy → depletion of multiple clotting factors
- Both PT and aPTT prolonged
- Low fibrinogen, low platelets, elevated D-dimer
- Triggered by sepsis, trauma, malignancy, obstetric emergencies
5. Factor Deficiencies (Inherited or Acquired)
- Factor VII deficiency: isolated PT prolongation (aPTT normal) — factor VII has the shortest half-life (~4–6 hours)
- Factor V deficiency: both PT and aPTT prolonged
- Acquired inhibitors against specific factors (rare)
6. Hypothermia
- Enzymatic activity of clotting factors is temperature-dependent
- Core temperature <35°C impairs coagulation cascade
- Common in major trauma (lethal triad: hypothermia + acidosis + coagulopathy)
- (Evaluation of Abnormal Liver Chemistries, p. 4)
7. Other Causes
- Massive transfusion — dilutional coagulopathy
- Amyloidosis — factor X adsorption onto amyloid fibrils
- Antiphospholipid syndrome — occasionally prolongs PT
- Disseminated malignancy
Diagnostic Algorithm
Elevated INR
|
├─ On warfarin / heparin? → Drug effect (therapeutic or supratherapeutic)
|
├─ Correct with Vitamin K?
| ├─ YES → Vitamin K deficiency (malabsorption, cholestasis, dietary)
| └─ NO → Liver disease (hepatocellular dysfunction) or inhibitor
|
├─ Check aPTT
| ├─ aPTT also prolonged → Common pathway defect, DIC, liver disease
| └─ aPTT normal → Factor VII deficiency (isolated), early warfarin
|
├─ Fibrinogen ↓ + D-dimer ↑ + Platelets ↓ → DIC
|
└─ Liver function tests → Hepatocellular vs. cholestatic pattern
Quick Reference Table
| Cause | PT/INR | aPTT | Platelets | Corrects with Vit K? | Key Clue |
|---|---|---|---|---|---|
| Liver disease | ↑ | ↑ | ↓ | Partial/No | LFTs abnormal, MELD score |
| Vitamin K deficiency | ↑ | ↑ (if severe) | Normal | Yes | Malabsorption, cholestasis, antibiotics |
| Warfarin | ↑ | Normal/↑ | Normal | Yes | Medication history |
| DIC | ↑ | ↑ | ↓ | No | Fibrinogen ↓, D-dimer ↑↑ |
| Factor VII deficiency | ↑ | Normal | Normal | No | Isolated PT prolongation |
| Hypothermia | ↑ | ↑ | ↓ | No | Low core temperature |
The most clinically important distinguishing step is the vitamin K correction test — it separates hepatocellular failure (does not correct) from deficiency/cholestasis (corrects), which fundamentally changes management.
B lines on usg
search_medical_text
B lines lung ultrasound findings causes significance
search_medical_image
B lines lung ultrasound comet tail artifacts
GradeResponse
GradeResponse
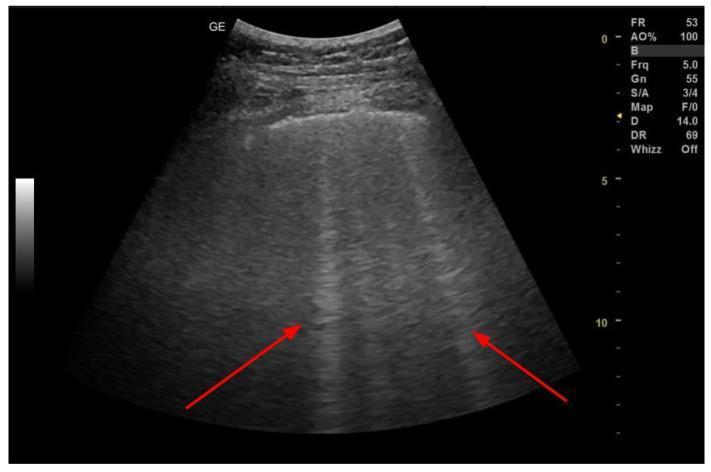
B-Lines on Lung Ultrasound
What Are B-Lines?
B-lines (also called comet-tail artifacts or lung comets) are vertical, hyperechoic, laser-like artifacts that arise from the pleural line and extend to the bottom of the screen without fading. They move synchronously with lung sliding.
Defining Features
| Feature | Description |
|---|---|
| Origin | Arise from the pleural line |
| Direction | Vertical (perpendicular to pleura) |
| Extent | Reach the bottom of the screen without fading |
| Movement | Slide with respiration (move with lung) |
| Acoustic shadow | Obliterate A-lines |
Normal lung: shows horizontal A-lines (reverberation artifacts) — absence of B-lines. ≥3 B-lines in a single intercostal space = interstitial syndrome (pathological)
Mechanism
B-lines are generated by thickened subpleural interlobular septa filled with fluid — they represent extravascular lung water (EVLW).
Causes Based on B-Line Pattern
| Pattern | Spacing | Cause |
|---|---|---|
| Discrete B-lines | ~7 mm apart | Interstitial syndrome (early pulmonary edema, ILD) |
| Irregular / asymmetric B-lines | Variable spacing | Pneumonia, contusion |
| Confluent / coalescent B-lines | <3 mm apart (nearly merged) | Severe pulmonary edema, confluent bronchopneumonia |
(Bedside Ultrasonography in Critically Ill Patients, p. 13)
Clinical Conditions Causing B-Lines
Cardiac / Cardiogenic
- Acute decompensated heart failure (most common) — bilateral, symmetric, diffuse B-lines
- Cardiogenic pulmonary edema
- Fluid overload
Pulmonary / Non-Cardiogenic
- Pneumonia — focal, unilateral, asymmetric B-lines
- ARDS — bilateral but heterogeneous/patchy distribution
- Interstitial lung disease (ILD/UIP/NSIP) — bilateral, predominantly basal, chronic
- Pulmonary contusion — post-trauma, focal
- COVID-19 pneumonitis — bilateral, patchy
Other
- Pleural disease — subpleural consolidation
- Post-radiotherapy fibrosis — localized
B-Lines: Cardiogenic vs. Non-Cardiogenic Differentiation
| Feature | Cardiogenic Pulmonary Edema | Pneumonia / ARDS |
|---|---|---|
| Distribution | Bilateral, symmetric, diffuse | Focal, asymmetric, patchy |
| Pleural line | Smooth | Irregular, thickened |
| Consolidation | Absent or basal | Often present |
| Pleural effusion | Common (bilateral) | Uncommon or unilateral |
| Response to diuresis | B-lines reduce rapidly | Persist |
BLUE Protocol (Bedside Lung Ultrasound in Emergency)
A rapid lung USS protocol using B-line patterns:
Dyspnea / Respiratory failure
|
Anterior zones bilateral
|
B-lines present?
/ \
YES NO (A-lines)
| |
Pulmonary edema Check DVT / PE
(heart failure) or COPD / asthma
|
Focal B-lines / consolidation?
→ Pneumonia
Key Clinical Pearls
- B-lines are dynamic — they decrease with diuresis in heart failure (useful for monitoring treatment response)
- Bilateral diffuse B-lines + reduced LV function on cardiac echo = cardiogenic pulmonary edema until proven otherwise
- B-lines cannot distinguish all causes alone — always correlate with clinical history, cardiac echo (EF, E/e'), and other zones
- Absence of B-lines with presence of A-lines + absent lung sliding = pneumothorax
This is a shared conversation. Sign in to Orris to start your own chat.