Pictorial representation of patau and edward for neet pg
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
I now have all the images I need. I can see that the two Robbins diagrams showing labeled Edwards syndrome features are very similar (from Robbins Basic Pathology and Robbins Cotran). Let me now compile a comprehensive, well-illustrated answer for NEET PG.
Patau Syndrome (Trisomy 13) & Edwards Syndrome (Trisomy 18) - NEET PG
EDWARDS SYNDROME - Trisomy 18
Karyotype: 47,XX,+18 (trisomy type) | 46,XX/47,XX,+18 (mosaic)
Incidence: 1 in 8,000 births | Prognosis: 85% lost between 10 weeks and term; born-alive babies usually die by 2 months; ~5% live beyond 1 year
Annotated Diagram (Robbins Pathology)
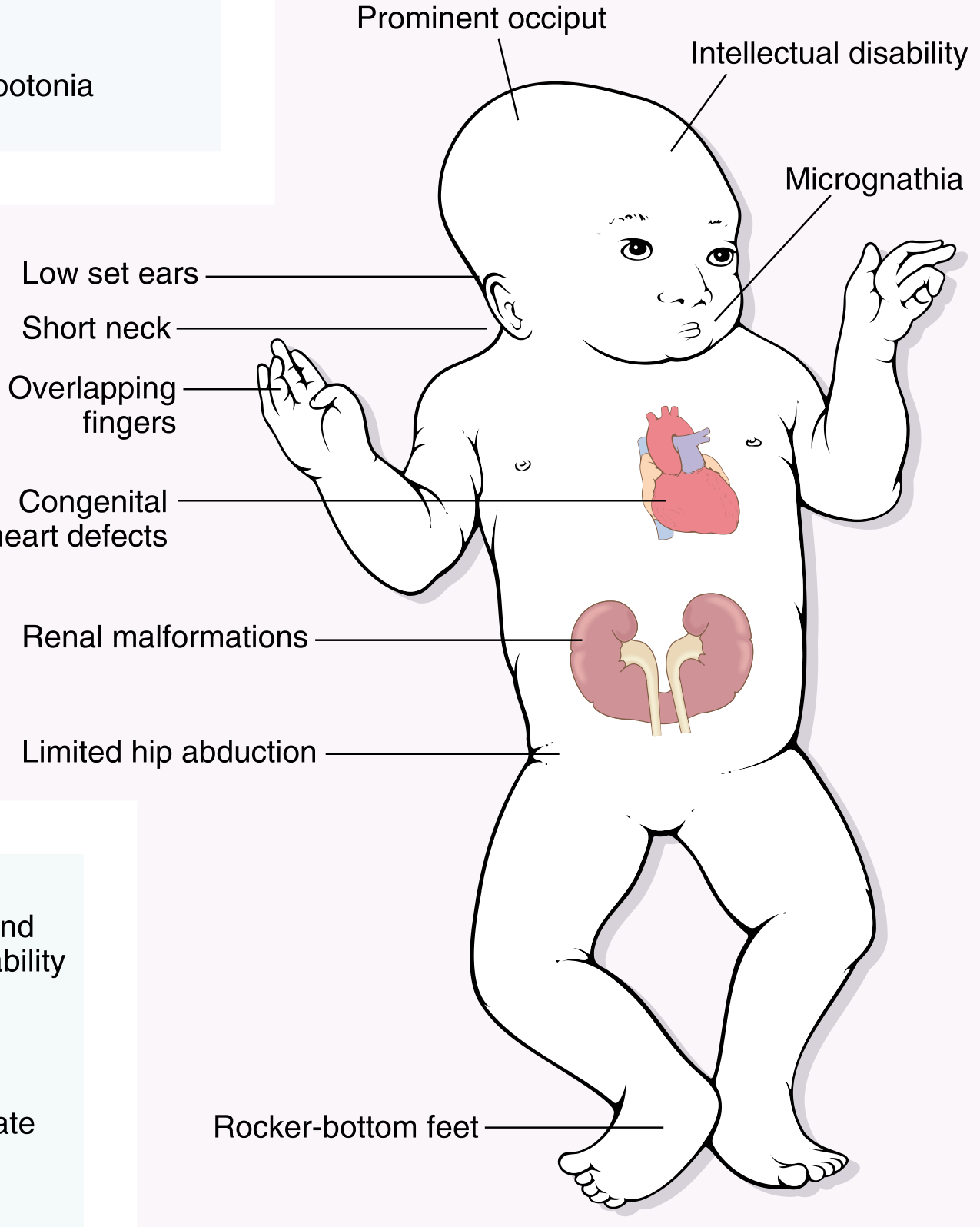
Fig. 4.19 - Robbins & Kumar Basic Pathology: Clinical features of Trisomy 18 (Edwards Syndrome)
Clinical Photo (Langman's Medical Embryology)

FIGURE 2.10 - Langman's: Child with trisomy 18. Note low-set ears, small mouth, micrognathia, flexion of the hands.
Key Features to Remember (NEET PG High-Yield)
| Feature | Detail |
|---|---|
| Head | Microcephaly, prominent occiput |
| Face | Micrognathia, low-set ears |
| Hands | Clenched fists with overlapping fingers (index over 3rd, 5th over 4th) - classic! |
| Feet | Rocker-bottom feet |
| Heart | Congenital heart defects (>90%) - VSD most common |
| Renal | Renal malformations, horseshoe kidney |
| Other | Limited hip abduction, hypotonia |
NEET PG Mnemonic for Trisomy 18: "18-Wheeler (truck) ROCKS on rocker-bottom feet with CLENCHED fists" - Rocker-bottom feet + overlapping/clenched fingers are the two most tested features.
PATAU SYNDROME - Trisomy 13
Karyotype: 47,XX,+13 (trisomy) | 46,XX,+13,der(13;14)(q10;q10) (Robertsonian translocation - ~10% of cases) | 46,XX/47,XX,+13 (mosaic)
Incidence: 1 in 15,000-20,000 live births | Prognosis: >90% die within the first month; ~5% live beyond 1 year
Annotated Diagram (Robbins Pathology)
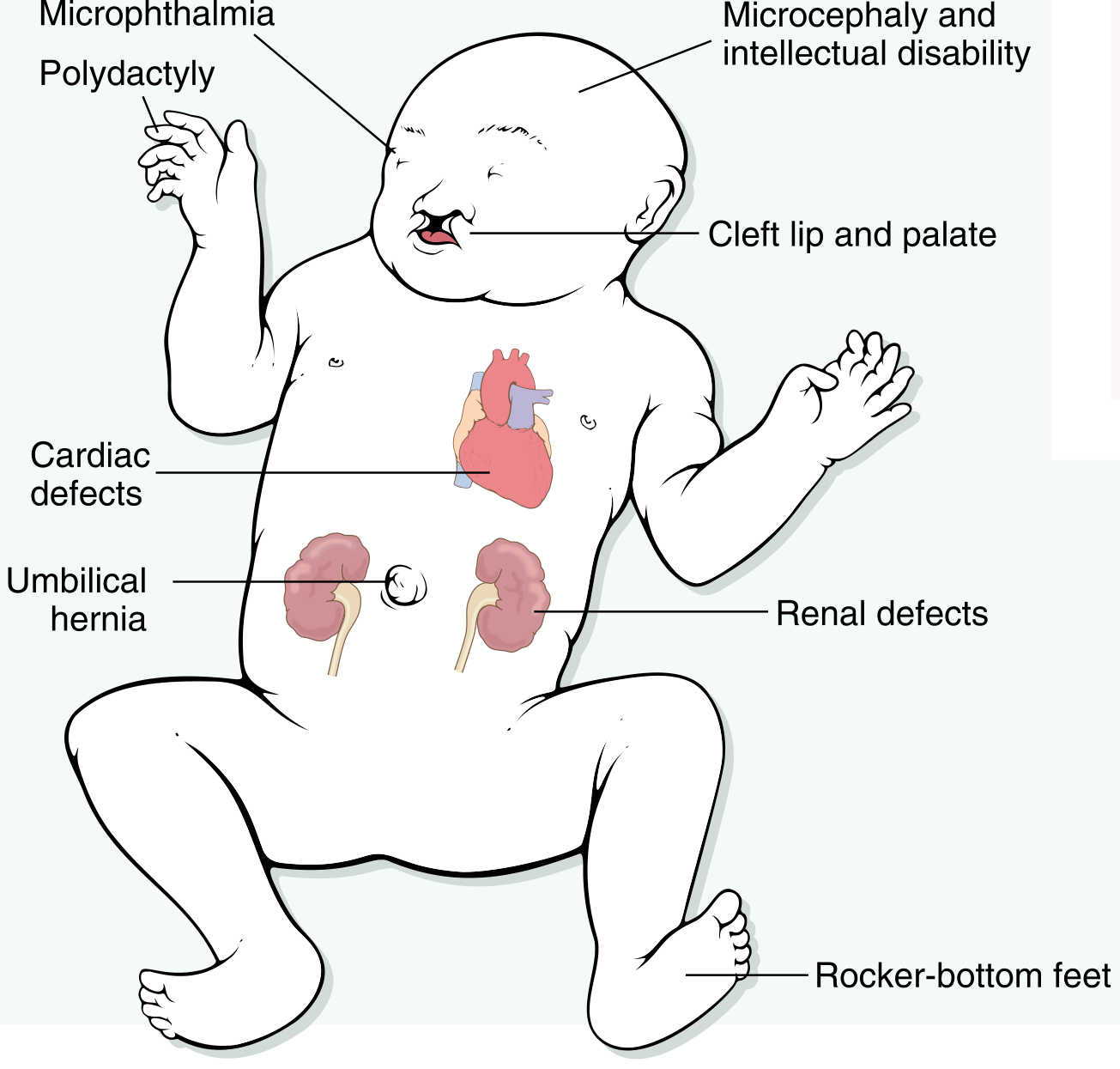
Fig. 5.22 - Robbins Cotran Pathologic Basis of Disease: Clinical features of Trisomy 13 (Patau Syndrome)
Clinical Photo - Facial Features (Langman's Medical Embryology)
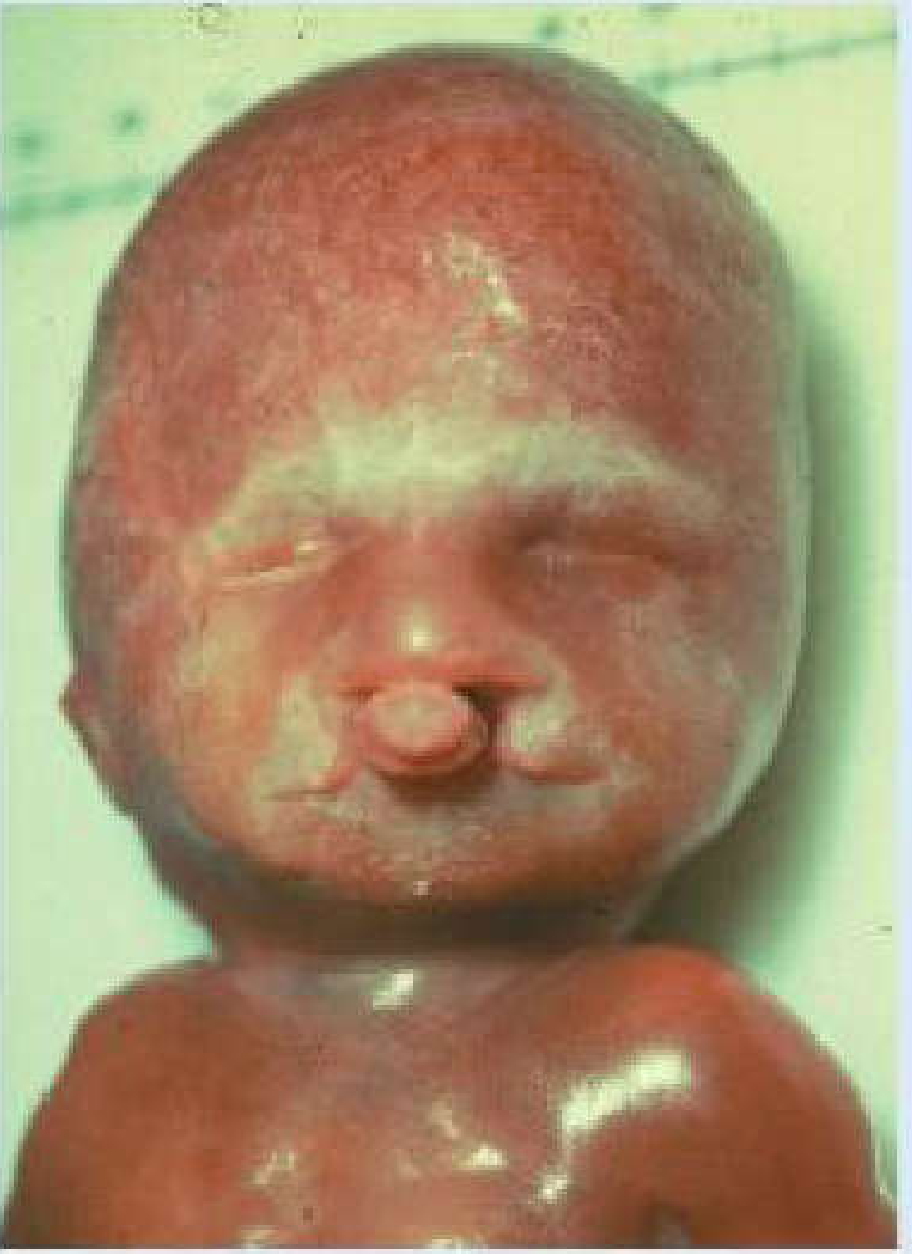
FIGURE 2.11 - Langman's: Child with trisomy 13 showing bilateral cleft lip, sloping forehead, and anophthalmia.
Key Features to Remember (NEET PG High-Yield)
| Feature | Detail |
|---|---|
| Brain | Holoprosencephaly (failure of forebrain to divide) - pathognomonic |
| Eyes | Microphthalmia / anophthalmia / coloboma |
| Face | Cleft lip + palate (bilateral, severe), broad/flat nose, sloping forehead |
| Hands | Postaxial polydactyly (extra fingers on ulnar/little finger side) |
| Scalp | Cutis aplasia (scalp defect) - unique to Patau |
| Heart | Cardiac defects (>90%) |
| Abdomen | Umbilical hernia / exomphalos |
| Renal | Renal defects (polycystic kidneys) |
| Hearing | Deafness |
NEET PG Mnemonic for Trisomy 13: "13 is unlucky - POLYDACTYLY, HOLOPROSENCEPHALY, CLEFT LIP" - The triad of holoprosencephaly + cleft lip/palate + postaxial polydactyly is classic for Trisomy 13.
Quick Comparison Table - NEET PG High-Yield
| Feature | Trisomy 18 (Edwards) | Trisomy 13 (Patau) |
|---|---|---|
| Chromosome | +18 | +13 |
| Incidence | 1 in 8,000 | 1 in 15,000-20,000 |
| Brain defect | Microcephaly | Holoprosencephaly |
| Eye defect | - | Micro/anophthalmia, coloboma |
| Face | Micrognathia, low-set ears | Cleft lip + palate, broad nose |
| Hands | Clenched/overlapping fingers | Postaxial polydactyly |
| Feet | Rocker-bottom feet | Rocker-bottom feet (both) |
| Scalp | - | Cutis aplasia |
| Cardiac | >90% | >90% |
| Renal | Horseshoe/malformed | Polycystic |
| Prognosis | Die by 2 months (mostly) | Die within 1 month (mostly) |
| Robertsonian translocation | No | Yes (10% of cases, chr 13;14) |
| Maternal age effect | Yes | Yes |
Sources: Robbins & Kumar Basic Pathology (Fig. 4.19), Robbins Cotran Pathologic Basis of Disease (Fig. 5.22), Langman's Medical Embryology (Figs. 2.10, 2.11), Emery's Elements of Medical Genetics and Genomics.
This is a shared conversation. Sign in to Orris to start your own chat.