Write a notes on Levels of Sedation and its scals for MD Anaesthesiology exam from Standard books
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Finding Sources
I now have all the information needed to write comprehensive notes. Let me compile the full exam-quality notes.
Levels of Sedation and Sedation Scales
Notes for MD Anaesthesiology Examination
Sources: Barash Clinical Anesthesia 9e, Miller's Anesthesia 10e, Rosen's Emergency Medicine 10e, Cummings Otolaryngology 7e, Fischer's Mastery of Surgery 8e
1. Introduction and Concept of the Sedation Continuum
Sedation is not a binary state but a graded, continuous spectrum from full wakefulness to general anesthesia. As increasing doses of sedative agents are administered, patients move progressively along this continuum, with a corresponding rise in the risk of respiratory and cardiovascular adverse events.
Key principle: The transition from one level to the next is often unpredictable and varies between patients. There is no sharp boundary - a patient intended to be at moderate sedation can inadvertently drift into deep sedation or general anesthesia.
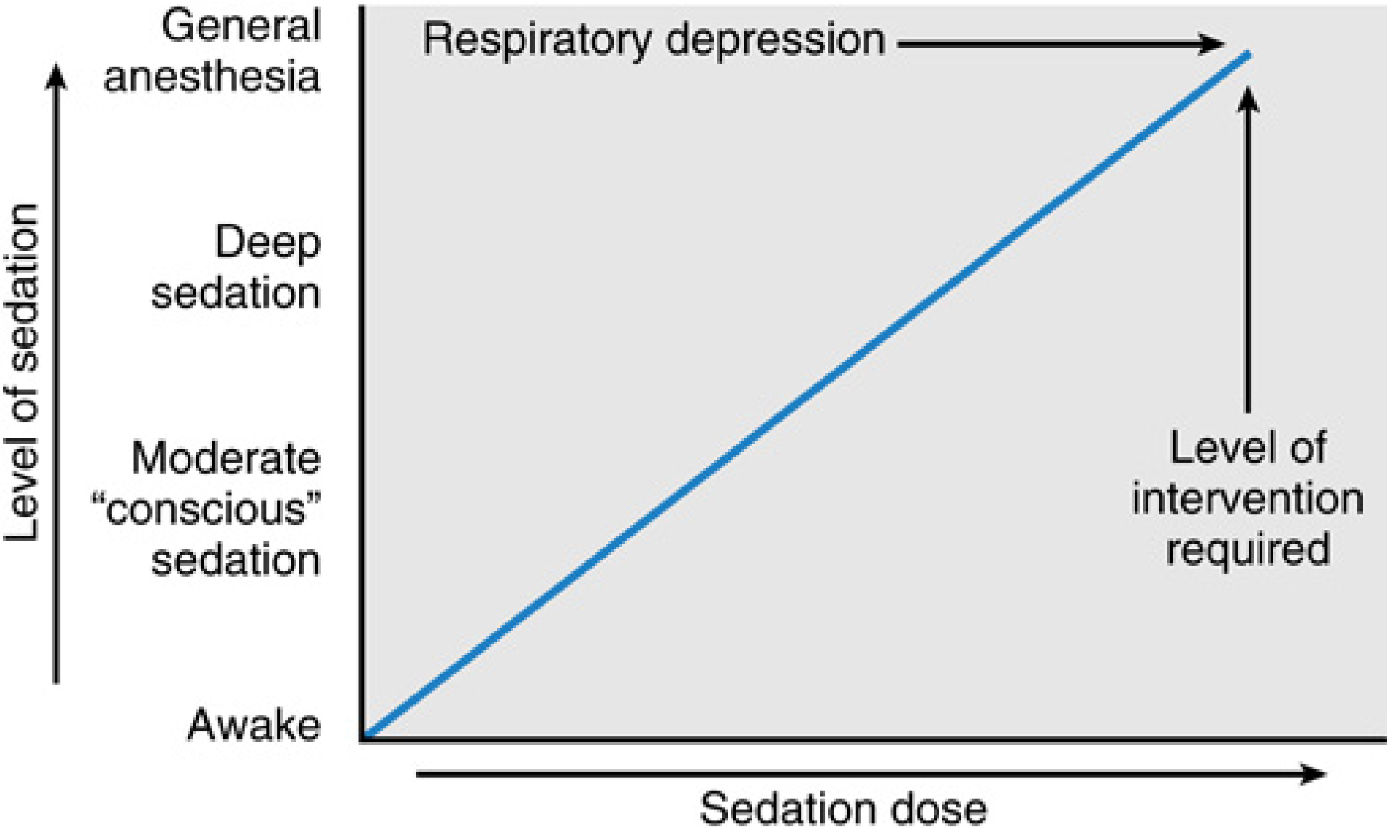
Fig. 68.3 - Miller's Anesthesia 10e: The continuum of sedation and general anesthesia. As sedation dose increases, the level of required intervention rises proportionally.
2. ASA Continuum of Depth of Sedation (2019)
The American Society of Anesthesiologists (ASA) formally defines four levels of sedation based on: responsiveness, airway, spontaneous ventilation, and cardiovascular function.
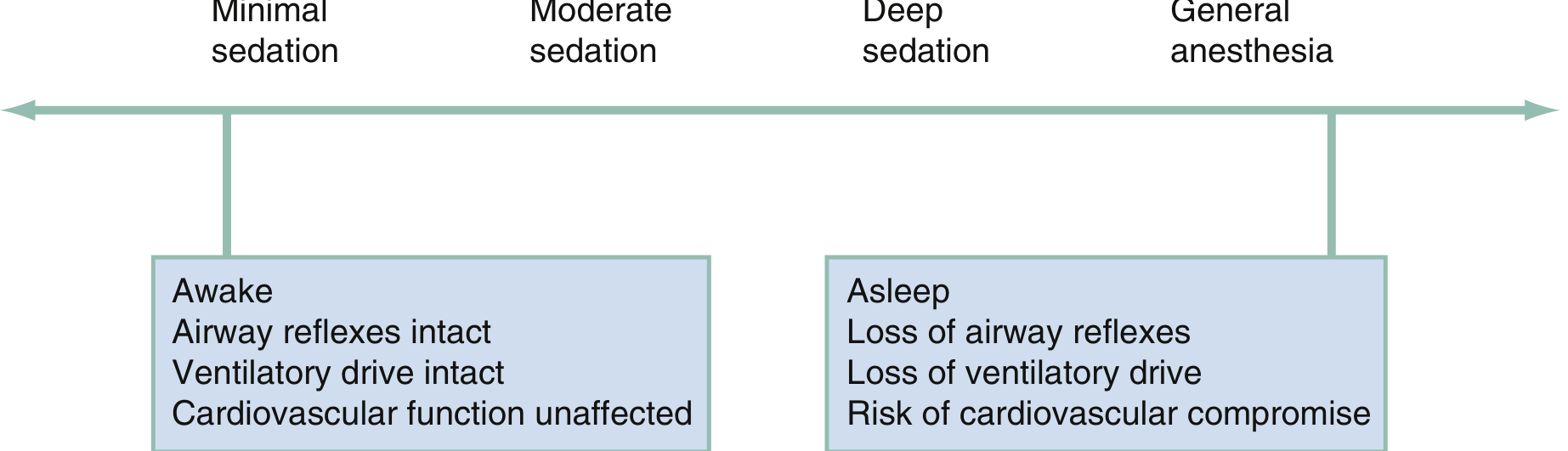
Fig. 7.1 - Rosen's Emergency Medicine: Schematic representation of the sedation continuum from minimal to general anesthesia.
ASA Table: Continuum of Depth of Sedation
| Parameter | Minimal Sedation (Anxiolysis) | Moderate Sedation/Analgesia ("Conscious Sedation") | Deep Sedation/Analgesia | General Anesthesia |
|---|---|---|---|---|
| Responsiveness | Normal response to verbal stimulation | Purposeful* response to verbal or tactile stimulation | Purposeful* response to repeated or painful stimulation | Unarousable, even with painful stimulus |
| Airway | Unaffected | No intervention required | Intervention may be required | Intervention often required |
| Spontaneous Ventilation | Unaffected | Adequate | May be inadequate | Frequently inadequate |
| Cardiovascular Function | Unaffected | Usually maintained | Usually maintained | May be impaired |
*Note: Reflex withdrawal from a painful stimulus is NOT considered a purposeful response.
(Adapted from ASA House of Delegates: Continuum of Depth of Sedation, 2019; as cited in Barash Clinical Anesthesia 9e, Table 30-2)
3. Detailed Description of Each Level
3.1 Minimal Sedation (Anxiolysis)
- Patient responds normally to verbal stimulation
- Cognitive function and coordination may be impaired
- Ventilatory and cardiovascular functions are completely unaffected
- Airway reflexes are fully intact
- Example agents: low-dose oral/IV benzodiazepines, low-dose nitrous oxide
3.2 Moderate Sedation/Analgesia ("Conscious Sedation")
- Patient responds purposefully to verbal commands alone or with light tactile stimulation
- Patient maintains a patent airway independently
- Spontaneous ventilation is adequate - no airway support required
- Cardiovascular function is usually maintained
- Patient can be aroused, can follow commands, and often retains partial memory
- Previously termed "conscious sedation" - this term is now discouraged as it implies a discrete state rather than a continuum
- Clinically used for: colonoscopy, minor procedures, endoscopy, cardioversion, fracture reduction
3.3 Deep Sedation/Analgesia
- Patient cannot be easily aroused but responds purposefully to repeated or painful stimulation
- May be accompanied by partial or complete loss of protective airway reflexes
- Airway assistance may be required
- Spontaneous ventilation may be inadequate
- Cardiovascular function is usually maintained
- Critical clinical point: A practitioner intending moderate sedation must be prepared to rescue a patient who enters deep sedation
3.4 General Anesthesia
- Patient is unarousable even with painful stimuli
- Ability to independently maintain ventilatory function is impaired - requires assisted or controlled ventilation
- Airway intervention is often required (ETT, LMA)
- Cardiovascular function may be impaired
- Loss of all protective airway reflexes
4. Special Category: Dissociative Sedation
Dissociative sedation (produced by ketamine) occupies a unique position outside the standard continuum and is sometimes listed as a fifth category:
| Parameter | Dissociative Sedation |
|---|---|
| Responsiveness | Unarousable to verbal; cataleptic state |
| Airway | Intervention may be required |
| Spontaneous Ventilation | Adequate (preserved) |
| Cardiovascular Function | Elevated (sympathomimetic) |
(Rosen's Emergency Medicine 10e, Table 7.1)
Key features of ketamine dissociative sedation:
- Maintains airway reflexes and spontaneous respiration better than other agents at equivalent depth
- Produces bronchodilation - useful in asthmatic patients
- Increases heart rate, blood pressure, and cardiac output
- Risk of emergence reactions (hallucinations, dysphoria) - mitigated by co-administration of a benzodiazepine
5. Sedation Scales
Multiple scales are used to assess and monitor depth of sedation. They are primarily used in ICU settings and for research. Aside from ASA definitions, most anesthesiologists do not routinely use numeric scales in the operating room.
(Barash Clinical Anesthesia 9e, Chapter 30)
5.1 Ramsay Sedation Scale (RSS) - 1974
Origin: Described by Ramsay et al. in 1974, originally developed for ICU patients receiving alphaxalone-alphadolone sedation.
Structure: 6 levels - 3 awake + 3 asleep
| Score | State | Description |
|---|---|---|
| 1 | Awake | Anxious, agitated, or restless |
| 2 | Awake | Cooperative, oriented, tranquil |
| 3 | Awake | Responds to commands only |
| 4 | Asleep | Brisk response to light glabellar tap or loud auditory stimulus |
| 5 | Asleep | Sluggish response to light glabellar tap or loud auditory stimulus |
| 6 | Asleep | No response to glabellar tap or loud auditory stimulus |
- Target in ICU: Scores 2-3 for awake/cooperative patients; 4-5 for sedated ventilated patients
- Limitation: Does not distinguish agitation subtypes; no level for alertness beyond "cooperative"
5.2 Modified Ramsay Sedation Scale (2003)
Proposed in 2003 to align with The Joint Commission's sedation definitions (based on ASA criteria). Added one extra level to both awake and asleep portions - total 8 levels.
| Score | Description |
|---|---|
| 1 | Awake and alert, minimal or no cognitive impairment |
| 2 | Awake but tranquil, purposeful response to verbal commands at conversational level |
| 3 | Appears asleep, purposeful responses to verbal commands at conversational level |
| 4 | Appears asleep, purposeful responses to verbal commands but requires louder voice or light glabellar tap |
| 5 | Asleep, sluggish purposeful responses only to loud verbal commands, strong glabellar tap, or both |
| 6 | Asleep, sluggish purposeful responses only to painful stimuli |
| 7 | Asleep, reflex withdrawal to painful stimuli only (no purposeful responses) |
| 8 | Unresponsive to all external stimuli, including pain |
(Barash Clinical Anesthesia 9e, Table 30-3)
5.3 Richmond Agitation-Sedation Scale (RASS) - 2002
Origin: Described in 2002. Validated for ICU patients. Now the most widely recommended scale by the Society for Critical Care Medicine (SCCM) guidelines.
Structure: 10-level scale (-5 to +4). Three-step assessment:
- Observation (first 30 seconds)
- Response to auditory stimuli (call patient's name)
- Response to physical stimuli (shoulder shake or sternal rub)
| Score | Label | Description |
|---|---|---|
| +4 | Combative | Overtly combative, violent, immediate danger to staff |
| +3 | Very Agitated | Pulls/removes tubes or catheters, aggressive, requires restraint |
| +2 | Agitated | Frequent non-purposeful movement, fights ventilator |
| +1 | Restless | Anxious, apprehensive, movements not aggressive; follows commands |
| 0 | Alert and Calm | Spontaneously attentive to caregiver; follows commands |
| -1 | Drowsy | Not fully alert, but has sustained awakening (>10 sec) with eye contact to voice |
| -2 | Light Sedation | Brief (<10 sec) awakening with eye contact to voice |
| -3 | Moderate Sedation | Movement or eye opening to voice; no eye contact |
| -4 | Deep Sedation | No response to voice, but movement or eye opening to physical stimulation |
| -5 | Unarousable | No response to voice or physical stimulation |
(Fischer's Mastery of Surgery 8e, Table 10.1; Fishman's Pulmonary Diseases 6e, Table 151-3)
Clinical targets:
- Goal RASS 0 to -2 for most ICU patients (alert/calm to light sedation)
- RASS -4 to -5 reserved for specific indications: status epilepticus (SE), ARDS, refractory intracranial hypertension
- RASS more negative than -2 is associated with: longer ICU stays, longer time to extubation
- RASS more positive than +1 is associated with: self-harm, self-extubation
High inter-rater reliability across physicians, nurses, and pharmacists.
5.4 Riker Sedation-Agitation Scale (SAS)
Companion scale to RASS. 7-point scale (1-7).
| SAS Score | Label | Description |
|---|---|---|
| 7 | Dangerous Agitation | Pulling at ETT, trying to remove catheters, climbing over bed rail, aggressive |
| 6 | Very Agitated | Requiring restraint and frequent reminders; biting ETT |
| 5 | Agitated | Anxious or mildly agitated; calms to verbal instructions |
| 4 | Calm and Cooperative | Calm, easily awakened, follows commands |
| 3 | Sedated | Difficult to arouse; awakens to verbal stimuli; follows simple commands but dozes off |
| 2 | Very Sedated | Arouses to physical stimuli but doesn't communicate or follow commands |
| 1 | Unarousable | Minimal/no response to noxious stimuli; does not communicate |
(Fishman's Pulmonary Diseases 6e, Table 151-3)
5.5 Observer's Assessment of Alertness/Sedation Scale (OAA/S)
Origin: Described in 1990 to assess benzodiazepine reversal with flumazenil in healthy adults.
Structure: Four domains of assessment used to generate a composite score from 0 to 5:
- Responsiveness
- Speech
- Facial expression
- Eyes
| Score | Responsiveness (most correlated item) |
|---|---|
| 5 | Responds readily to name spoken in normal tone |
| 4 | Lethargic response to name spoken in normal tone |
| 3 | Responds only after name called loudly or repeatedly |
| 2 | Responds only after mild prodding or shaking |
| 1 | Responds only to painful stimulation |
| 0 | No response to painful stimulation |
- Demonstrated excellent inter-rater reliability
- The responsiveness component most often correlates with the composite score
- Widely used in procedural sedation studies
- Modified versions have been published to better align with the ASA Continuum of Depth of Sedation
(Barash Clinical Anesthesia 9e, Chapter 30)
5.6 Correlation of Scales with ASA Sedation Levels
| ASA Level | Modified Ramsay | RASS | Modified OAA/S |
|---|---|---|---|
| Minimal Sedation (anxiolysis) | 1 | +1 to +4 (agitation - not anxiolysis) | 5 |
| Moderate Sedation ("conscious sedation") | 2, 3, 4 | 0, -1, -2, -3 | 4, 3, 2 |
| Deep Sedation | 5, 6 | -4 | 1 |
| General Anesthesia | 7, 8 | -5 | 0 |
(Barash Clinical Anesthesia 9e, Table 30-3)
Exam note: The RASS positive scores (+1 to +4) reflect agitation, not anxiolysis/minimal sedation - they do NOT map directly to the ASA minimal sedation category.
6. Processed EEG - Bispectral Index (BIS)
The BIS is a processed EEG parameter for monitoring drug-induced sedation depth. It supplements clinical sedation scales, especially when clinical assessment is limited (paralysis, aphasia, deafness).
| BIS Value | Clinical State |
|---|---|
| 90-100 | Awake |
| 80-90 | Light/minimal sedation |
| 60-80 | Moderate-deep sedation (moderate risk of recall) |
| 40-60 | General anesthesia (adequate depth, low recall) |
| <40 | Very deep anesthesia / burst suppression |
Key study finding: Absence of intraoperative recall is associated with BIS values <80 (Liu et al.; Kearse et al.). However, BIS values can show significant variability - some wide-awake patients can have low BIS scores and vice versa, depending on the drug used.
(Barash Clinical Anesthesia 9e, Chapter 30)
7. Monitoring Standards for Sedation
As per ASA standards, monitoring during sedation should be equivalent to that used during general or regional anesthesia:
| Parameter | Requirement |
|---|---|
| ECG | Continuous display mandatory |
| Blood Pressure | Measured and recorded every 5 minutes minimum |
| Pulse oximetry | Continuous |
| Capnography (ETCO2) | Mandatory during moderate and deep sedation |
| Temperature | When clinically significant changes are intended, anticipated, or suspected |
(Barash Clinical Anesthesia 9e, Chapter 30; Cummings Otolaryngology, Table 104.3)
8. Important Clinical Pearls for the Exam
-
The continuum is non-linear and non-predictable: Any patient receiving sedation may inadvertently progress to the next deeper level; practitioners must be capable of rescue at least one level deeper than intended.
-
Reflex withdrawal is NOT purposeful response: A patient withdrawing a limb from a painful stimulus is NOT in moderate sedation - this is a spinal reflex.
-
MAC (Monitored Anesthesia Care): MAC is a billing/service term, not a level of sedation. It refers to the anesthesia service itself and may include any level of sedation including general anesthesia if needed.
-
"Conscious sedation" terminology: This term is now discouraged. The preferred term is "moderate sedation/analgesia" as it better reflects the continuum concept.
-
RASS is the most recommended scale for ICU sedation monitoring per SCCM guidelines. It has high inter-rater reliability across all healthcare providers.
-
Ramsay Scale (original) has only 6 levels (3 awake + 3 asleep); the modified version has 8 levels.
-
OAA/S: 4 domains (responsiveness, speech, facial expression, eyes); score 0-5; responsiveness item most important.
-
Risk equivalence: ASA closed claims data shows that risk of death or permanent brain damage during procedural sedation is similar to that of general anesthesia - most commonly due to respiratory depression from opioids and sedative-hypnotics.
-
Ketamine (dissociative sedation): Unlike non-dissociative agents, it preserves airway reflexes and spontaneous ventilation while providing profound analgesia. Cardiovascular effects are stimulatory (elevated heart rate and BP).
-
RASS target in ICU: Generally -2 to +1; avoid deep sedation (RASS < -2) unless specifically indicated.
Summary Table: Key Features of Sedation Scales
| Scale | Year | Range | Levels | Setting | Key Feature |
|---|---|---|---|---|---|
| ASA Continuum | 1996/2019 | - | 4 | OR/procedural | Gold standard definition |
| Ramsay (RSS) | 1974 | 1-6 | 6 | ICU | Oldest; awake + asleep |
| Modified Ramsay | 2003 | 1-8 | 8 | Procedural/ICU | Aligned with ASA/TJC |
| RASS | 2002 | -5 to +4 | 10 | ICU | Best inter-rater reliability; SCCM recommended |
| SAS (Riker) | - | 1-7 | 7 | ICU | Used alongside RASS |
| OAA/S | 1990 | 0-5 | 6 | Research/procedural | 4-domain composite |
| BIS | - | 0-100 | Continuous | OR/ICU | Processed EEG; objective |
References:
- Barash, Cullen, and Stoelting's Clinical Anesthesia, 9th Ed., Chapter 30 (MAC and Sedation)
- Miller's Anesthesia, 10th Ed., Chapter 68 (Day Case Surgery)
- Rosen's Emergency Medicine, 10th Ed., Chapter 7 (Procedural Sedation)
- Cummings Otolaryngology Head & Neck Surgery, Chapter 104/184 (Anesthesia)
- Fischer's Mastery of Surgery, 8th Ed., Chapter 10 (ICU Sedation and Analgesia)
- Fishman's Pulmonary Diseases and Disorders, 6th Ed., Chapter 151 (Critical Care Sedation)
This is a shared conversation. Sign in to Orris to start your own chat.