enthovins traingle for 5 marks
Reading File
Finding Sources
Searching Images
Einthoven's triangle ECG leads
Finding Sources
Loading Image
Reading File
Reading File
Loading Image
Reading File
Loading Image
Here is a comprehensive 5-mark answer on Einthoven's Triangle:
Einthoven's Triangle
Definition & Concept
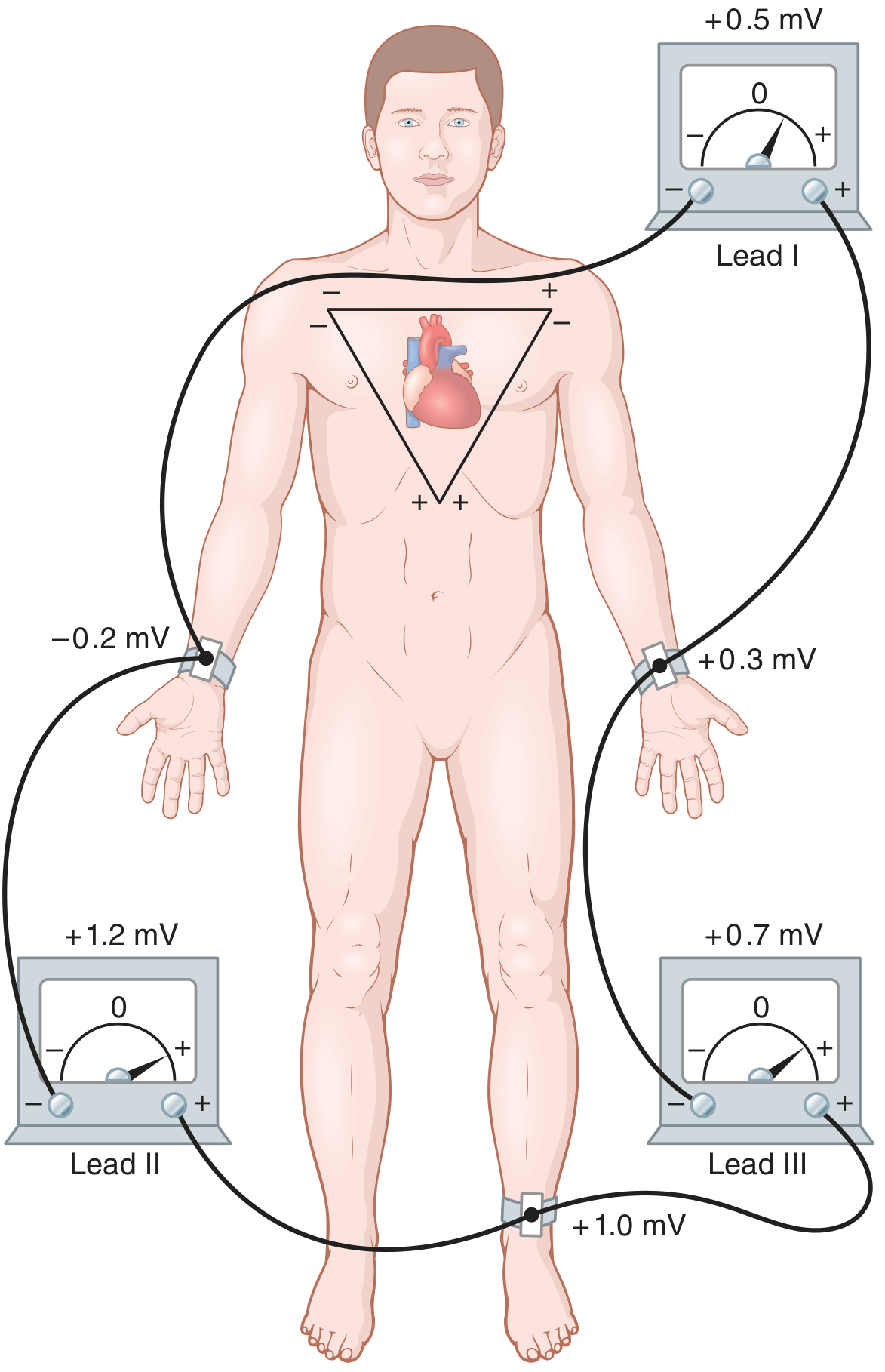
Einthoven's triangle is an equilateral triangle formed by the three standard bipolar limb leads (I, II, III) of the ECG, with the heart positioned at its centre. It is based on the assumption that the human body is a volume conductor, and that the two arms and left leg form the three apices of this equilateral triangle surrounding the heart.
The Three Sides (Leads)
| Lead | Negative Pole | Positive Pole | Side of Triangle |
|---|---|---|---|
| Lead I | Right Arm (RA) | Left Arm (LA) | Top (horizontal) |
| Lead II | Right Arm (RA) | Left Leg (LL) | Left side |
| Lead III | Left Arm (LA) | Left Leg (LL) | Right side |
Each side of the triangle represents one bipolar lead. The positive poles lie inferiorly and to the left, which is why deflections are predominantly upright in the normal ECG.
Key Assumptions
- The body acts as a homogeneous volume conductor
- The heart is located at the geometric centre of the triangle
- The triangle is equilateral — though this is an approximation, it gives clinically useful results
- In a volume conductor, the sum of potentials at the three points of an equilateral triangle with a current source at its center equals zero at all times
Einthoven's Law
A critical mathematical consequence of the triangle is Einthoven's Law:
Lead I + Lead III = Lead II
(Note: polarity signs must be respected)
Example: If RA = −0.2 mV, LA = +0.3 mV, LL = +1.0 mV:
- Lead I = (+0.3) − (−0.2) = +0.5 mV
- Lead III = (+1.0) − (+0.3) = +0.7 mV
- Lead II = (+1.0) − (−0.2) = +1.2 mV ✓ (= Lead I + Lead III = 0.5 + 0.7)
Clinical Significance — Determining the Cardiac Vector/Axis
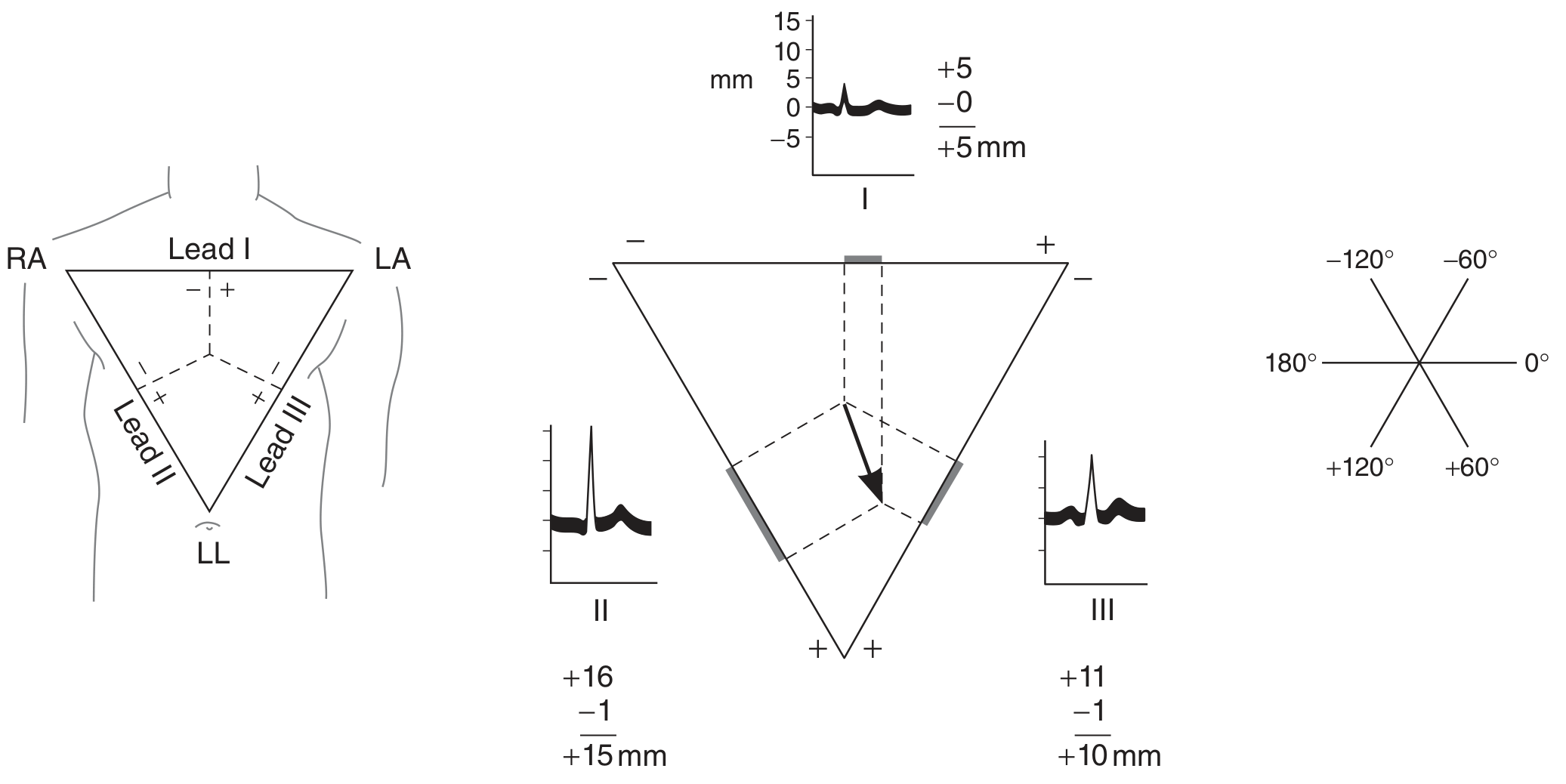
The triangle is used to calculate the mean electrical axis of the heart (e.g., mean QRS vector):
- Measure the net amplitude of the QRS complex in any two leads (e.g., I and II or II and III)
- Plot these values as distances along the respective sides of the triangle from their midpoints
- Drop perpendiculars from these points inward
- The intersection of the perpendiculars gives the tip of the mean QRS vector
- An arrow from the electrical centre to this point = magnitude and direction of the cardiac axis
Normal QRS axis = −30° to +90° in the frontal plane.
Summary Points (for 5 marks)
- Einthoven's triangle = equilateral triangle formed by the 3 standard limb leads (I, II, III) with the heart at the centre
- Three apices = Right arm, Left arm, Left leg
- Einthoven's Law: Lead I + Lead III = Lead II (potentials are algebraically interdependent)
- Basis: Body is a volume conductor; sum of potentials at three equilateral points around a central source = zero
- Clinical use: Determination of the mean electrical axis of the heart (cardiac vector) in the frontal plane
Sources: Guyton & Hall Textbook of Medical Physiology; Ganong's Review of Medical Physiology, 26th ed.
axis deviation
Finding Sources
Searching Images
ECG axis deviation left right determination
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Here is a comprehensive note on Axis Deviation:
Axis Deviation
Normal QRS Axis
The mean electrical axis of the ventricles in the frontal plane normally lies between −30° and +90° (average ~59°). Even in healthy individuals, it can swing from about 20° to 100° due to anatomical variations in the Purkinje system and ventricular musculature.
Classification of Axis
| Axis Range | Classification |
|---|---|
| −30° to +90° | Normal |
| More negative than −30° | Left Axis Deviation (LAD) |
| More than +90° | Right Axis Deviation (RAD) |
| −90° to ±180° | Extreme/Northwest axis (indeterminate) |
Note: Mild RAD beyond +90° is a normal variant in children and adolescents.
Quick ECG Recognition
| Lead I | Lead aVF | Axis |
|---|---|---|
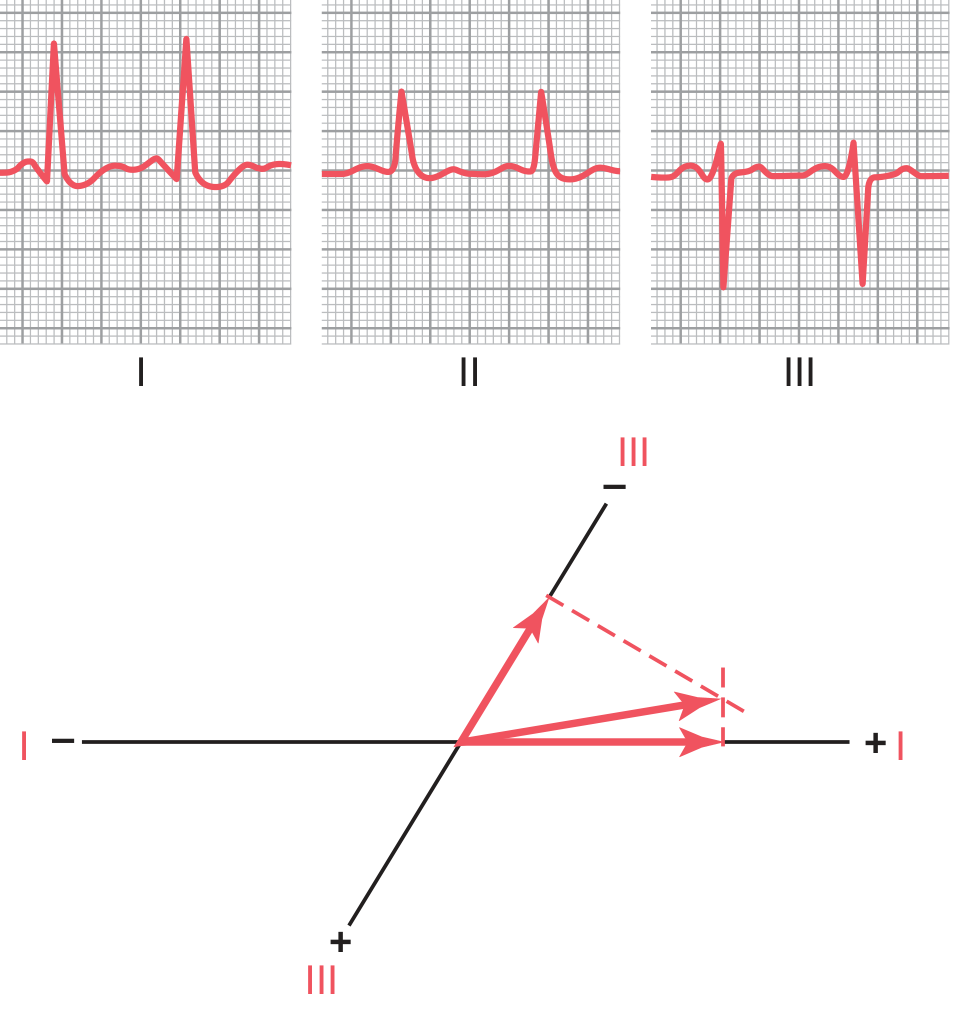
| + | + | Normal |
| + | − | LAD |
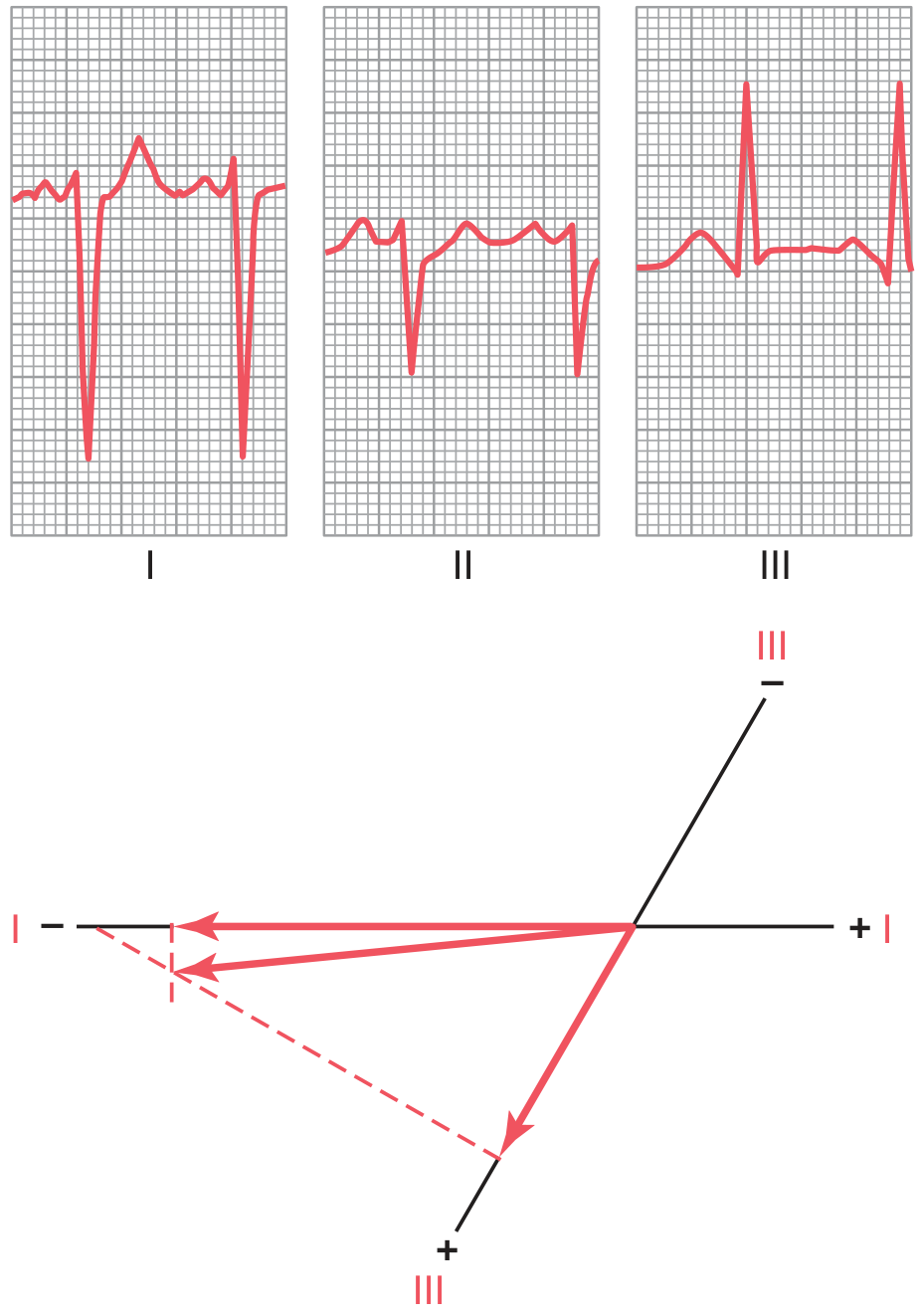
| − | + | RAD |
| − | − | Extreme (NW) axis |
A more precise method: find the lead where the QRS is most isoelectric → the axis is perpendicular to that lead.
Causes of Left Axis Deviation (LAD)
1. Change in Heart Position
- End of deep expiration
- Lying down (abdominal contents push diaphragm up)
- Obesity (elevated diaphragm chronically)
2. Ventricular Hypertrophy
- Left ventricular hypertrophy (LVH) — more muscle mass on the left generates a dominant leftward vector
Causes of LVH → LAD:
- Systemic hypertension
- Aortic valve stenosis / regurgitation
- Congenital conditions with left ventricular dominance
3. Bundle Branch Block
- Left bundle branch block (LBBB) → intense LAD (~−50°)
- Left ventricle depolarizes 2–3× more slowly than the right
- Right ventricle becomes electronegative first; vector points toward the electropositive left ventricle
- QRS complex is significantly widened (>0.12 s)
4. Hemiblock (Fascicular Block)
- Left anterior fascicular block (LAFB) → abnormal LAD (most common cause of LAD on ECG)
Causes of Right Axis Deviation (RAD)
1. Change in Heart Position
- End of deep inspiration
- Standing up
- Tall, thin individuals (vertical heart)
- Neonates/infants (physiological, due to RV dominance)
2. Ventricular Hypertrophy
- Right ventricular hypertrophy (RVH) — dominant rightward vector from increased right-sided muscle mass
Causes of RVH → RAD:
- Pulmonary valve stenosis
- Tetralogy of Fallot
- Interventricular septal defect (VSD)
- Pulmonary hypertension
3. Bundle Branch Block
- Right bundle branch block (RBBB) → right axis deviation
- Left ventricle depolarizes first → becomes electronegative; vector points toward the electropositive right ventricle
- QRS also widened
4. Hemiblock
- Left posterior fascicular block (LPFB) → abnormal RAD
Why Axis Deviation Occurs in Hypertrophy
Two mechanisms drive the axis shift toward the hypertrophied ventricle:
- Greater electrical potential generated by the larger muscle mass on the hypertrophied side
- Longer depolarization time in the hypertrophied ventricle → the normal ventricle becomes electronegative first, creating a net vector pointing toward the hypertrophied (still electropositive) ventricle
Differentiating Bundle Branch Block from Hypertrophy
| Feature | Bundle Branch Block | Hypertrophy |
|---|---|---|
| QRS width | >0.12 s (widened) | May be slightly widened |
| Axis deviation | Present | Present |
| Cause | Conduction block | Increased muscle mass |
Summary
- LAD (axis more negative than −30°): LVH, LBBB, LAFB, obesity, expiration
- RAD (axis beyond +90°): RVH, RBBB, LPFB, thin/tall body, inspiration, neonates
- Axis deviation toward a hypertrophied ventricle occurs because more muscle = more electrical potential + longer depolarization time
- Bundle branch blocks cause axis deviation plus widened QRS — this distinguishes them from pure hypertrophy
Sources: Guyton & Hall Textbook of Medical Physiology; Goldman-Cecil Medicine, International Ed.; Ganong's Review of Medical Physiology, 26th ed.
This is a shared conversation. Sign in to Orris to start your own chat.