Panopthalmitis case, presentation negative history.
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Loading Image
I now have comprehensive information to provide a thorough answer. Let me compile it.
Panophthalmitis: Case Presentation with Negative History
Definition and Distinction from Endophthalmitis
Endophthalmitis = suppurative inflammation confined to the vitreous humor (and anterior chamber).
Panophthalmitis = inflammation extending beyond the vitreous to involve the retina, choroid, and sclera, extending into the orbit - the entire globe and periorbital tissues are affected.
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 1216
The "Negative History" Problem - Endogenous Route
A negative history means no identifiable exogenous entry point - no trauma, no recent ocular surgery, no corneal ulcer. This pattern points decisively to endogenous panophthalmitis, where the organism reaches the eye hematogenously.
Classification
| Type | Route | History |
|---|---|---|
| Exogenous | Penetrating trauma, surgery, corneal ulcer, extension from paranasal sinuses | Positive history (trauma/surgery) |
| Endogenous | Hematogenous spread from bacteremia, fungemia, sepsis, distant focus | Negative ocular history |
- Tietz Textbook of Laboratory Medicine, 7th Ed., p. 3452
Endogenous Panophthalmitis - What to Look For
When the patient presents with no ocular injury or surgery, you must hunt for a systemic source:
Common Systemic Sources
- Bacteremia / sepsis (any cause) - gram-positive toxin-producing organisms, gram-negative rapidly destructive organisms
- Candidemia - especially in IV drug users, ICU patients, patients on broad-spectrum antibiotics, TPN, or immunocompromised hosts. Candida is the *leading fungal cause of endogenous endophthalmitis/panophthalmitis
- Pulmonary infections - hematogenous seeding from pneumonia or lung abscess
- Contiguous spread from paranasal sinuses (especially ethmoiditis), dacryocystitis, dacryoadenitis, orbital cellulitis
- Dental infections
- Infective endocarditis
"Endogenous fungal endophthalmitis may also occur in the absence of a known infection in the blood or other body sites" - making the history truly negative even on systemic review.
- Tietz Textbook of Laboratory Medicine, 7th Ed., p. 3452-3453
Pathophysiology
- Organism seeds the highly vascular choroid (most common initial site)
- Spreads to retina (chorioretinitis)
- Extension into the vitreous = endophthalmitis
- Progression through sclera into orbit = panophthalmitis
- The retina tolerates suppurative inflammation poorly - irreversible retinal injury can occur within hours
Clinical Presentation
Symptoms
- Sudden, rapidly progressive loss of vision
- Severe ocular pain
- Headache (from orbital involvement)
- Systemic fever/malaise if endogenous
Signs (Ocular)
- Eyelid edema and erythema
- Chemosis (conjunctival edema)
- Severe conjunctival injection
- Corneal edema
- Absent red reflex (vitreous opacification)
- Hypopyon (anterior chamber pus)
- Severe anterior uveitis
- Iris microabscesses
- Flame-shaped retinal hemorrhages ± white centers
- Retinal/subretinal/choroidal abscesses
- Retinal inflammatory infiltrates
- Proptosis (from orbital extension)
- Complete distortion of globe architecture in advanced cases (as seen in the pathology image below)
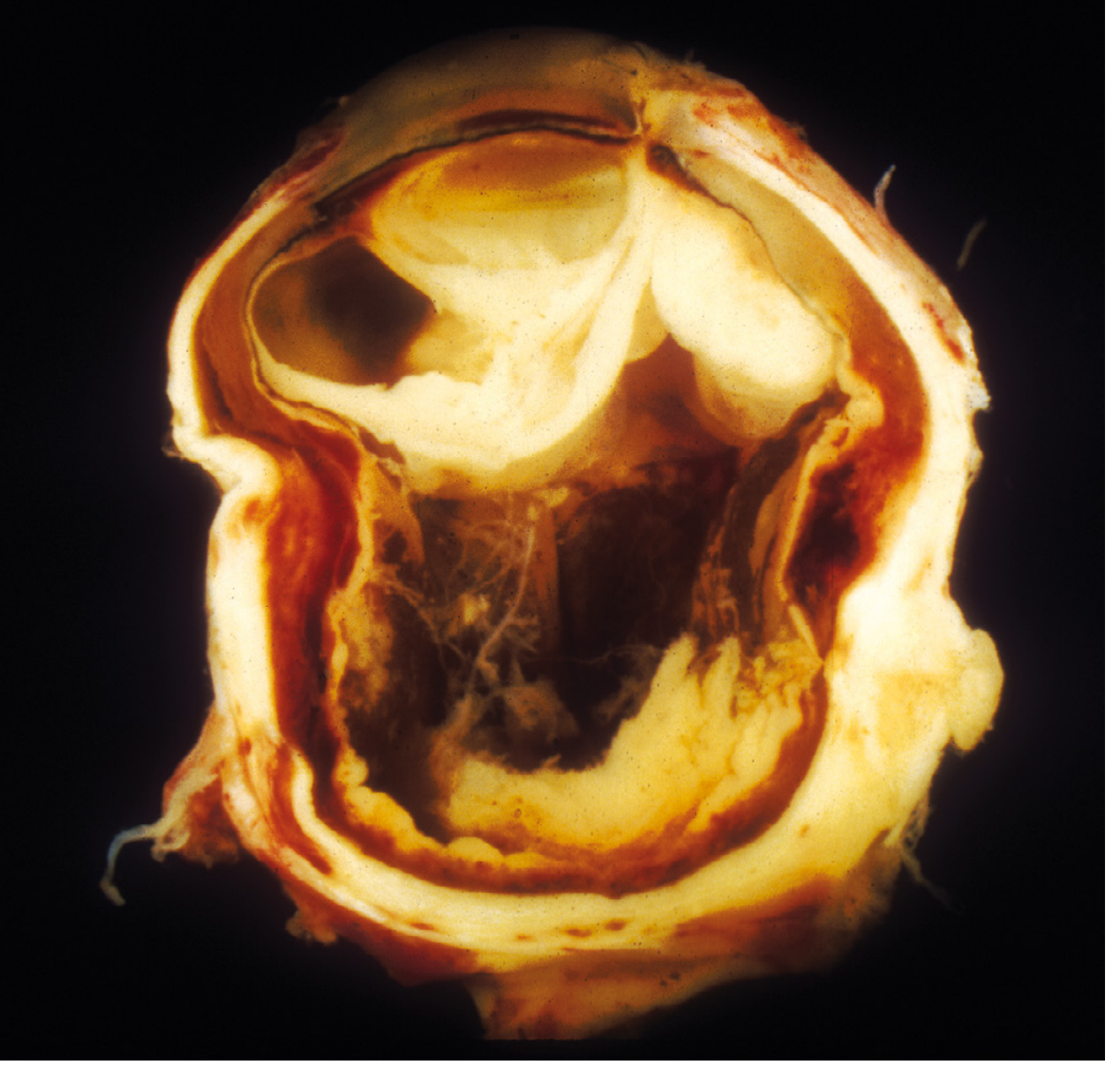
Fig. 29.16 - Exogenous panophthalmitis. Suppurative inflammation has completely distorted the eye's architecture. (Robbins Pathologic Basis of Disease)
Workup
Ocular
- Slit-lamp examination - cells in AC and vitreous (can only be seen by slit lamp biomicroscopy)
- B-scan ultrasound - vitreous opacification, orbital involvement
- Vitreous tap / aqueous tap - Gram stain + culture (most important step; vitreous sample preferred over aqueous)
- Culture of any removed foreign body (if applicable)
Systemic (for negative history / endogenous workup)
- Blood cultures x 2-3 sets (before antibiotics)
- Complete blood count, CRP, ESR, procalcitonin
- Fungal cultures (if candidemia risk factors)
- Echocardiography (rule out endocarditis)
- CT chest/abdomen/pelvis (source of bacteremia)
- Dental panorex (dental abscess)
- CT/MRI sinuses (sinusitis)
- HIV testing, immunodeficiency workup
Causative Organisms
Bacteria
- Post-traumatic / exogenous: Staphylococcus spp., Bacillus spp. (~90% of culture-positive post-traumatic cases)
- Virulent: Toxin-producing gram-positives and gram-negatives (rapid, destructive course)
- Indolent: Propionibacterium acnes, Staphylococcus epidermidis
- Post-surgical: Coagulase-negative Staphylococcus, S. aureus, streptococci
Fungi
- Endogenous: Candida spp. (main fungal cause of endogenous infection)
- Exogenous: Molds (more common in exogenous infections)
- Note: fungemia leads to endophthalmitis more readily than bacteremia; endogenous fungal infection may occur without detectable fungemia
Management
Immediate
- This is an ocular emergency - same-day ophthalmology involvement mandatory
- Intravitreal antibiotics (first-line):
- Vancomycin 1 mg/0.1 mL (gram-positives)
- Ceftazidime 2.25 mg/0.1 mL (gram-negatives)
- Repeat intravitreal antibiotics at 48 hours if no improvement
- Consider posterior vitrectomy (reduces microbial/inflammatory debris, treats associated vitreoretinal pathology)
Adjunctive
- Topical antibiotics (if corneal ulcer present)
- Topical steroids (after 48 hours, to reduce inflammation-mediated damage)
- Oral fluoroquinolones (ciprofloxacin 750 mg BD or moxifloxacin 400 mg OD) for 10-14 days
- Systemic antibiotics - generally not effective for isolated ocular infection but essential if endogenous (treat systemic source)
Endogenous Cases
- Treat the systemic source in parallel (antifungals for candidemia, antibiotics for bacteremia, surgical drainage of abscess, etc.)
Last Resort
- Evisceration or enucleation - when the eye is unsalvageable and there is risk of cavernous sinus thrombosis or intracranial extension; panophthalmitis outcome is often blindness or loss of eye, especially when virulent organisms are involved
Key Clinical Pearls for Negative History Cases
- Absence of trauma or surgery does not rule out infection - always consider endogenous route
- Candidemia is a major silent culprit - check for risk factors (IV lines, TPN, prior antibiotics, diabetes, immunosuppression)
- Fungemia can be absent even in true endogenous fungal panophthalmitis
- Endogenous hematogenous seeding starts in the choroid because of its rich vascularity
- Speed is everything - irreversible retinal injury within hours; vitreous tap and intravitreal antibiotics should not be delayed for culture results
- Poor outcomes (blindness, evisceration) are more likely when organisms are virulent (Bacillus, gram-negatives) or when treatment is delayed
Sources: Robbins, Cotran & Kumar Pathologic Basis of Disease (p. 1216); Tietz Textbook of Laboratory Medicine 7th Ed. (p. 3452-3453); Goldman-Cecil Medicine (Ch. 391); Kanski's Clinical Ophthalmology 10th Ed.; Tintinalli's Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.