Fever drugs
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Here is a complete overview of drugs used to treat fever (antipyretics), drawn from Harrison's Principles of Internal Medicine (22nd ed.), Lippincott Pharmacology, and Tietz Laboratory Medicine.
Fever Drugs (Antipyretics)
How Antipyretics Work
Fever is driven by prostaglandin E2 (PGE2) raising the hypothalamic set point. Antipyretics reduce PGE2 by inhibiting cyclooxygenase (COX) enzymes, thereby lowering the set point and facilitating heat loss. Glucocorticoids act at two levels: they inhibit phospholipase A2 (blocking arachidonic acid release) and block transcription of pyrogenic cytokines.
- Harrison's Principles of Internal Medicine 22E, p. 180
1. Acetaminophen (Paracetamol) - First-line Antipyretic
| Property | Detail |
|---|---|
| Mechanism | Inhibits COX in the CNS (particularly COX-3); weak peripheral COX inhibition so minimal anti-inflammatory effect |
| Route | Oral, IV, rectal suppository |
| Use | Fever + mild-to-moderate pain; preferred in children, GI-sensitive patients |
| Special note | Drug of choice in children with viral infections or chickenpox (avoids Reye syndrome risk from aspirin) |
| Key toxicity | Hepatotoxicity in overdose - NAPQI metabolite depletes glutathione and causes liver necrosis |
| Antidote | N-acetylcysteine (NAC) - most effective within 8 hours of overdose |
| Avoid in | Severe hepatic impairment, chronic alcoholism, malnutrition (increased hepatotoxicity risk) |
Oral aspirin and acetaminophen are equally effective at reducing fever, but acetaminophen is preferred due to fewer GI and platelet side effects.
- Lippincott Illustrated Reviews: Pharmacology, p. 1364
Acetaminophen Metabolism Diagram
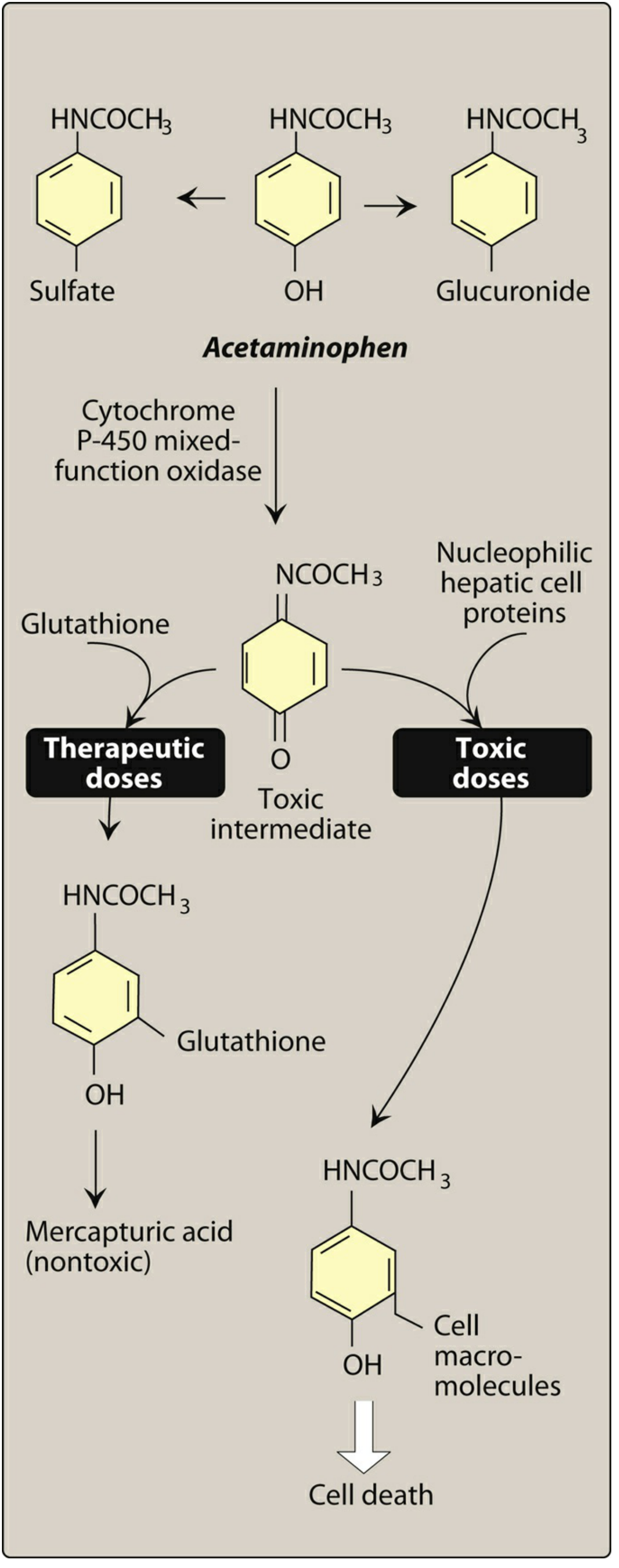
Figure: Metabolism of acetaminophen - normal doses safely conjugate NAPQI with glutathione; overdose saturates this pathway causing hepatic necrosis (Lippincott Pharmacology)
2. NSAIDs (Non-Steroidal Anti-Inflammatory Drugs)
All NSAIDs work by inhibiting COX-1 and/or COX-2, reducing PGE2 synthesis peripherally and centrally.
| Drug | Notes |
|---|---|
| Ibuprofen | Commonly used; in children under 2, may have improved efficacy vs. acetaminophen in first 24 hours; available OTC |
| Aspirin | Effective antipyretic; contraindicated in children (Reye syndrome risk with viral illness); affects platelets |
| Naproxen | Longer-acting NSAID; used in adults |
| Indomethacin | Potent; used for refractory fever (e.g., Hodgkin-related fever) |
| COX-2 inhibitors (e.g., celecoxib) | Excellent antipyretics; less GI toxicity but potential cardiovascular risk |
Class adverse effects: GI irritation/bleeding, platelet inhibition, renal impairment. As a group (except aspirin), NSAIDs may increase risk of MI and stroke.
- Harrison's Principles of Internal Medicine 22E, p. 180
3. Glucocorticoids
- Act by inhibiting phospholipase A2 (reducing arachidonic acid release) AND blocking pyrogenic cytokine mRNA transcription
- Used for fever in autoimmune/autoinflammatory diseases (e.g., systemic lupus, adult Still disease)
- Not first-line for routine infectious fever
4. Anticytokine Therapies (for Autoinflammatory Diseases)
- Anakinra and canakinumab (IL-1 blockers): dramatically reduce fever in IL-1beta-driven autoinflammatory conditions (familial Mediterranean fever, adult/juvenile Still disease, pericarditis, gout)
- These are disease-specific, not general antipyretics
When Treating Fever is Strongly Recommended
- Patients with cardiac, pulmonary, or CNS impairment (fever raises O2 demand by ~13% per 1°C above 37°C)
- Children with history of febrile seizures (treat aggressively)
- Hyperpyrexia - cooling blankets should be combined with oral antipyretics, not used alone
Quick Comparison Table
| Drug | COX Inhibition | Anti-inflammatory | Safe in Children | GI Risk |
|---|---|---|---|---|
| Acetaminophen | CNS only (COX-3) | Minimal | Yes | Low |
| Ibuprofen | COX-1 + COX-2 | Yes | Yes (not <6 months) | Moderate |
| Aspirin | COX-1 > COX-2 | Yes | No (Reye risk) | High |
| Naproxen | COX-1 + COX-2 | Yes | Caution | Moderate |
| Glucocorticoids | Phospholipase A2 | Yes | Caution | Moderate |
Sources: Harrison's Principles of Internal Medicine 22E | Lippincott Illustrated Reviews: Pharmacology | Tietz Textbook of Laboratory Medicine 7th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.