Endonasal dcr
Reading File
Finding Sources
Searching PubMed
endonasal dacryocystorhinostomy
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the key content. Let me compile a comprehensive answer.
Endonasal (Endoscopic) Dacryocystorhinostomy (DCR)
Definition and Rationale
Endonasal DCR is the surgical bypass of the lacrimal sac and nasolacrimal duct (NLD) performed entirely through the nasal cavity under endoscopic guidance. It treats epiphora caused by distal lacrimal system obstruction, without any external facial incision. The key principle is creating the widest possible marsupialization of the medial wall of the lacrimal sac.
Epiphora (tears draining down the face) must be distinguished from a "watery eye" (thick tear film without overflow) - the former has surgical indications, the latter is usually medical.
Anatomy (Key Landmarks)
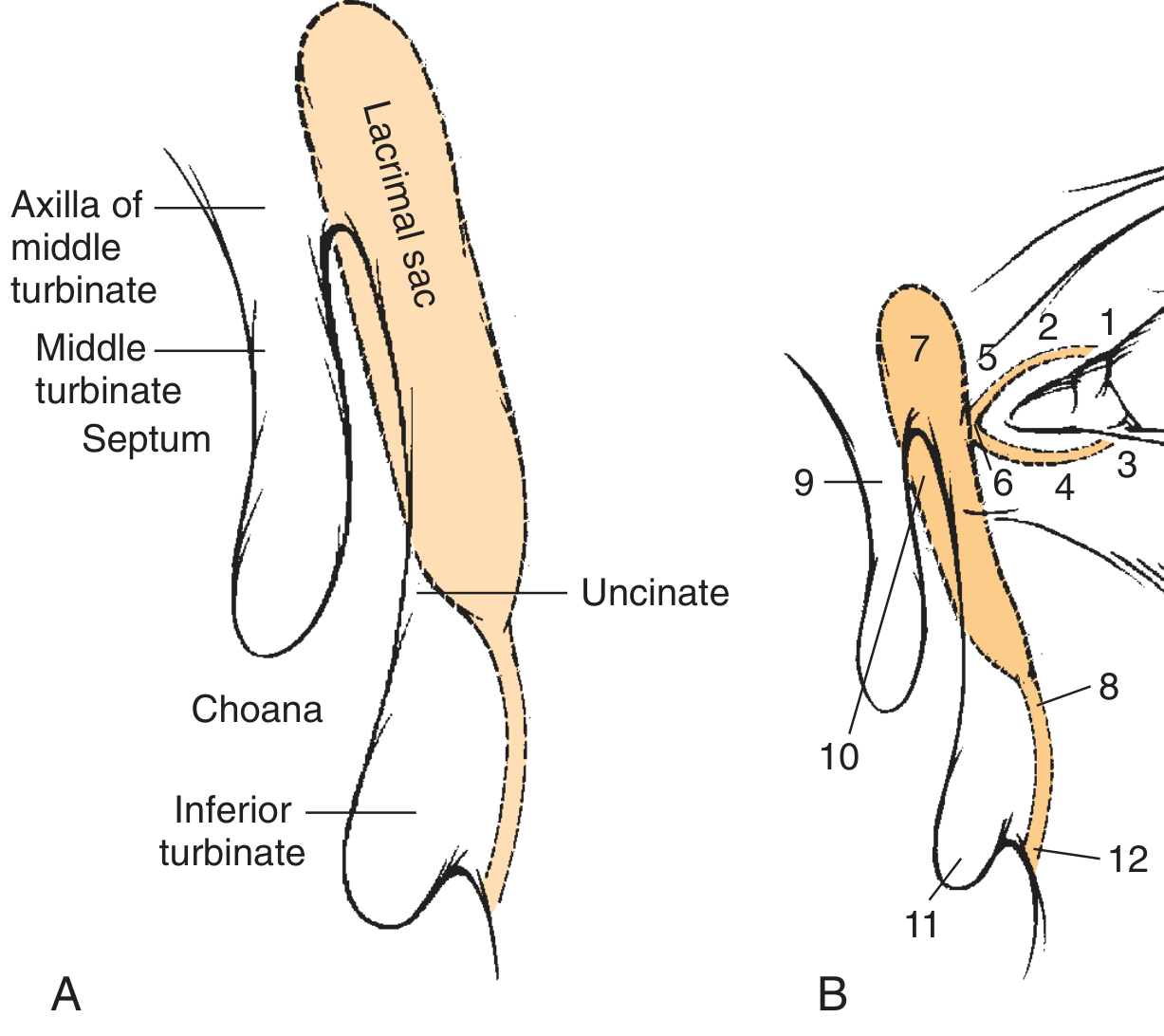
Fig. A - Endonasal view: Lacrimal sac lies under mucosa and the frontal process of maxilla. The axilla of the middle turbinate is the key endoscopic landmark.
- Upper 1/3 of sac: just superior to the anterior insertion of the middle turbinate
- Lower 2/3: oriented vertically just under the anterior maxillary line (lacrimomaxillary suture)
Bones covering the sac:
- Frontal process of maxilla (thicker, anterior)
- Lacrimal bone (thinner, posterior)
Structures (Fig. B):
- Superior punctum | 2. Superior canaliculus | 3. Inferior punctum | 4. Inferior canaliculus | 5. Medial canthal ligament | 6. Common canaliculus | 7. Lacrimal sac | 8. Lacrimal duct | 9. Middle turbinate | 10. Lacrimal bone | 11. Inferior turbinate | 12. Hasner valve
The common internal punctum (valve of Rosenmüller) is the critical landmark - it represents the most proximal level manageable by DCR. Pathology proximal to this (canalicular stenosis) cannot be fixed by DCR alone.
Indications
| Indication | Notes |
|---|---|
| Nasolacrimal duct obstruction (NLDO) - anatomic | Best outcomes; complete physical blockages |
| NLDO - functional | Critical narrowings or pump failure; inferior outcomes vs anatomic |
| Dacryocystitis (acute/chronic) | Early endonasal DCR now supported by evidence |
| Dacryoliths | Middle-aged patients |
| Failed external DCR (revision) | Endoscopic approach is ideal for revisions |
| Pediatric persistent epiphora | After failed probing; bony atresia |
Anatomic : functional obstruction ratio = 70% : 30%; anatomic obstructions have superior DCR outcomes.
Cannot be treated by DCR alone: Superior, inferior, or common canalicular stenosis.
Pre-operative Diagnostics
Physical Examination
- Exclude lid laxity, malposition, punctal anomalies, blepharitis
- Palpation over lacrimal sac - reflux of mucopurulence = dacryocystitis = obstruction amenable to DCR
- Dye disappearance test - 2% fluorescein in conjunctival fornix; normal = complete symmetrical disappearance in 5 minutes
- Jones I test - cotton swab in inferior meatus confirms fluorescein flow
Jones II Test (Probing)
- Hard stop: probe impacts medial wall of sac/bone = canalicular system patent = obstrucion is distal
- Soft stop: probe impeded before entering sac = canalicular stenosis = DCR alone insufficient
Lacrimal Irrigation
- Patient tastes saline = rules out complete obstruction but suggests partial/functional block
- No taste = complete obstruction
Radiologic Evaluation
- Dacryocystography (DCG) - anatomic obstruction: dye fails to penetrate to nasal cavity
- Lacrimal scintigraphy - functional obstruction: dye reaches nasal cavity on DCG but fails to clear on 25-min scintigraphy
- CT scan: useful pre-operatively to assess bony anatomy and sac position
Surgical Technique (Powered Endoscopic DCR)
Setup
- General or local anaesthesia
- Topical decongestion (oxymetazoline) + local infiltration (lidocaine with epinephrine) at axilla of middle turbinate
- 0-degree and 30-degree 4 mm rigid endoscopes
Step-by-Step
Step 1 - Mucosal incision
A vertical/H-shaped mucosal incision is made anterior to the axilla of the middle turbinate, over the frontal process of maxilla.
Step 2 - Mucosal flap elevation
Anterior-based mucosal flap is elevated to expose the frontal process of maxilla and lacrimal bone.
Step 3 - Bone removal
- A powered microdebrider with a cutting burr removes the frontal process of maxilla (thicker bone anteriorly)
- The thinner posterior lacrimal bone is removed with through-cutting forceps (Kerrison rongeurs)
- Critical: bone removal must be complete, medial to the entire lacrimal sac - "saucerization" of surrounding bone
Step 4 - Sac identification and opening
- The lacrimal sac is identified by light transillumination from a canalicular probe placed by the ophthalmology team
- The medial wall of the sac is incised with a sickle knife/needle and marsupialised using through-cutting forceps to create anterior and posterior flaps
Step 5 - Mucosal apposition
- Anterior sac flap is anastomosed to anterior nasal mucosal flap
- Posterior sac flap is laid against the lateral nasal wall
- Goal: complete mucosal coverage of the osteotomy site to prevent stenosis
Step 6 - Silicone stent placement
- A bicanalicular silicone stent is threaded from upper and lower puncta, through the canaliculi into the sac, and retrieved endoscopically from the nose
- Ends secured with a clip or cotton swab loop intranasally (no tension on puncta)
- Removed at 3-6 months
Advantages Over External DCR
| Feature | Endonasal | External |
|---|---|---|
| Facial scar | None | Yes (medial canthal) |
| Lacrimal pump | Preserved (medial canthal ligament intact) | Disrupted |
| Blood loss | Less | More |
| Revision cases | Superior access | Difficult scarring |
| Success rate | ~85-95% (similar) | ~85-95% |
| Learning curve | Steeper | More established |
Outcomes
- Success rates for endoscopic DCR are equivalent to external DCR (both ~85-95%)
- Anatomic obstruction > functional obstruction in terms of outcomes
- Inadequate marsupialization of the lacrimal sac is the primary cause of failure
- Children: excellent success rates comparable to adult DCR
- A 2023 network meta-analysis (PMID 37184641) compared external, endonasal, and transcanalicular laser DCR with/without silicone stenting across RCTs
Complications
Common
| Complication | Details |
|---|---|
| Ostial granuloma | Most common; 47% at ostium edge; treat with topical steroids, excision, or intralesional triamcinolone; recurrence <5% |
| Cheese-wiring | Silicone stent under tension tears through puncta; prevented by looping tube before fixation |
| Surgical failure | Inadequate bone removal leaving unopened sac portion → fluid meniscus → increased resistance |
| Haemorrhage | Intraoperative; minimised with decongestion and epinephrine |
| Synechiae | Middle turbinate adhesion to lateral wall |
Rare but Serious
| Complication | Details |
|---|---|
| CSF leak | Due to surgeon inexperience with endoscopic anatomy |
| Orbital penetration | Damage to extraocular muscles |
| Frontal/maxillary sinusitis | Damage to drainage pathways |
| CPAP air regurgitation | 80% of CPAP users may develop post-op ophthalmic symptoms |
Missed lacrimal sac tumour
- Tumour presents in delayed fashion in ~1/3 of DCR failures
- Warning signs: bloody nasal drainage, medial canthal swelling, proptosis
- Common benign: squamous/transitional papilloma; malignant: SCC/transitional cell carcinoma
- Management: combined external + endoscopic extirpation + adjuvant radiotherapy for malignant lesions
Revision DCR
Indications for revision include persistent epiphora with confirmed ostial stenosis/closure on endoscopy. Endoscopic approach is preferred over external for revision as it avoids scarring from the prior external incision. The scar tissue at the ostium is excised, remaining sac mucosa marsupialised, and silicone stent re-inserted.
Key Points Summary
- Goal: widest possible marsupialization of medial sac wall
- Critical landmark: axilla of middle turbinate (upper sac); lacrimomaxillary suture (lower sac)
- Don't miss: common canalicular obstruction (soft stop on probing) = DCR won't work alone
- Success: complete bone removal + mucosal flap apposition + adequate sac opening
- Primary failure cause: inadequate bony removal with incomplete sac opening
- Best team approach: otolaryngologist (endoscopic anatomy) + oculoplastic surgeon (lacrimal system)
Sources:
- Cummings Otolaryngology Head and Neck Surgery, Chapter 49 - Endoscopic DCR
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol 2 - DCR section
- Evereklioglu C et al. Network meta-analysis of DCR techniques. Graefes Arch Clin Exp Ophthalmol 2023 [PMID: 37184641]
- Li J et al. Early endonasal DCR for acute dacryocystitis: meta-analysis. Am J Rhinol Allergy 2024 [PMID: 38444220]
Tongue tie
Reading File
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
Tongue tie release
Finding Sources
Searching PubMed
ankyloglossia frenulotomy frenotomy
Finding Sources
Searching PubMed
ankyloglossia tongue tie frenotomy outcomes
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Reading File
Loading Image
Loading Image
I now have all the content needed for a comprehensive answer. Let me compile it.
Tongue Tie (Ankyloglossia) and Its Release
Definition
Ankyloglossia (tongue tie) is a congenital anomaly in which an abnormally short, thick, or anteriorly placed lingual frenulum restricts tongue mobility. The frenulum tethers the undersurface of the tongue to the floor of mouth, limiting protrusion, elevation, and lateral movement.
Epidemiology
- Incidence: 0.02% to 10.7% of newborns (wide range due to varying diagnostic criteria)
- More common in males: M:F ratio 1.5-2.6:1
- No racial predilection
- 21-50% of individuals report a family history - genetic basis
- Associated with X-linked cleft palate via mutations in the TBX22 gene
- Incidence appears to decrease with age, suggesting some resolve spontaneously as frenulum naturally stretches or breaks
Classification

| Type | Frenulum Insertion | Category |
|---|---|---|
| Type I | At tongue tip | Anterior (traditional) |
| Type II | Slightly behind tongue tip | Anterior (traditional) |
| Type III | Mid- to posterior undersurface of tongue; thickened | Posterior |
| Type IV | Submucosal flat broad mound at tongue base | Posterior |
- Types I & II = "anterior" or classic ankyloglossia
- Types III & IV = "posterior" ankyloglossia (harder to identify, increasingly recognised)
- ~60% of cases are Type III
Clinical Features and Diagnosis
Physical Signs
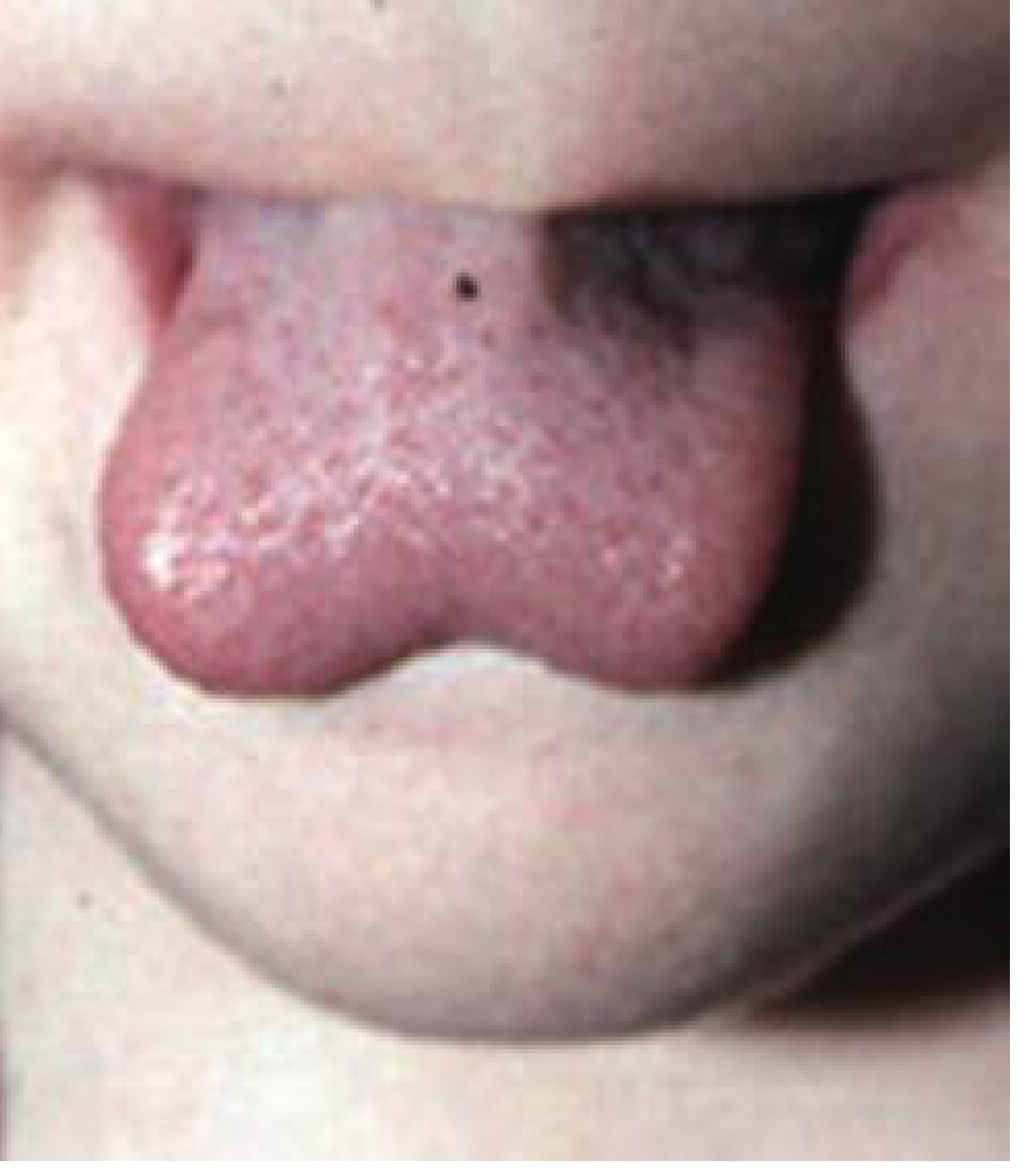
Heart-shaped tongue on maximal protrusion - classic sign

Severe ankyloglossia in adult with near-complete inability to protrude tongue
- Heart-shaped or notched tongue on protrusion (midtethering causes bifid appearance)
- Tongue may roll or curl rather than extend straight
- Inability to elevate tongue tip to upper dentition
- Impaired side-to-side tongue movement
- Tongue fails to extend past lower lip (though some with tongue tie can protrude past the lip)
- Diastasis (gap) between lower central incisors in some cases
Assessment Tools
| Tool | Use | Details |
|---|---|---|
| LATCH score | Validated breastfeeding assessment | Latch, Audible swallow, Nipple type, Comfort, Help |
| HATLFF (Hazelbaker) | Neonatal functional assessment | 7 tongue movements each scored 0-2; comprehensive but complex |
| BTAT (Bristol Tongue Assessment Tool) | Screening tool by midwives | Simpler, suitable for busy hospital settings |
Interincisal Distance Test
The tongue tip is placed behind upper incisors and the mouth opened maximally. The interincisal distance measures the degree of tongue elevation - reduced distance indicates functional limitation.
Sequelae / Clinical Problems
In Infants (Breastfeeding)
- 15-44% of babies with ankyloglossia have breastfeeding problems
- Poor latch due to inability to extend and cup the tongue adequately
- Infant unable to bring sufficient breast tissue into mouth
- Maternal nipple pain - most common complaint (28% of mothers in first 6 days postpartum)
- Ineffective milk transfer leading to poor weight gain / failure to thrive
- Premature breastfeeding cessation
In Older Children/Adults
- Speech articulation difficulties - particularly lingual sounds (l, r, t, d, n, th, s, z)
- Dental: diastasis of lower central incisors; dental caries on anterior maxillary incisors (from poor oral hygiene access); periodontal disease/gingival recession
- Difficulty licking lips, playing wind instruments, kissing
- Mechanical eating difficulties
Treatment Indications
Treatment is not universally required. The decision should be guided by functional impairment:
Treat when:
- Breastfeeding difficulties with documented latch problems AND poor maternal-infant dyad
- Failure to thrive due to poor milk transfer
- Significant speech articulation problems not responsive to therapy
- Symptomatic dental/periodontal consequences
Observe when:
- Anatomic tie present but no functional problems
- Breastfeeding progressing well
- No speech difficulties
Note: There is ongoing controversy about treatment - especially for posterior ties and in the absence of clear functional deficits.
Surgical Procedures
Three procedures are used:
| Procedure | Description |
|---|---|
| Frenotomy | Simple incision/division of the frenulum - does not require excision |
| Frenuloplasty | Division with plastic repair (horizontal-to-vertical Z-plasty); lengthens floor of mouth mucosa |
| Frenectomy | Complete removal - technically a misnomer when applied to lingual frenulum (rarely needed) |
Frenotomy (Neonatal - Most Common)
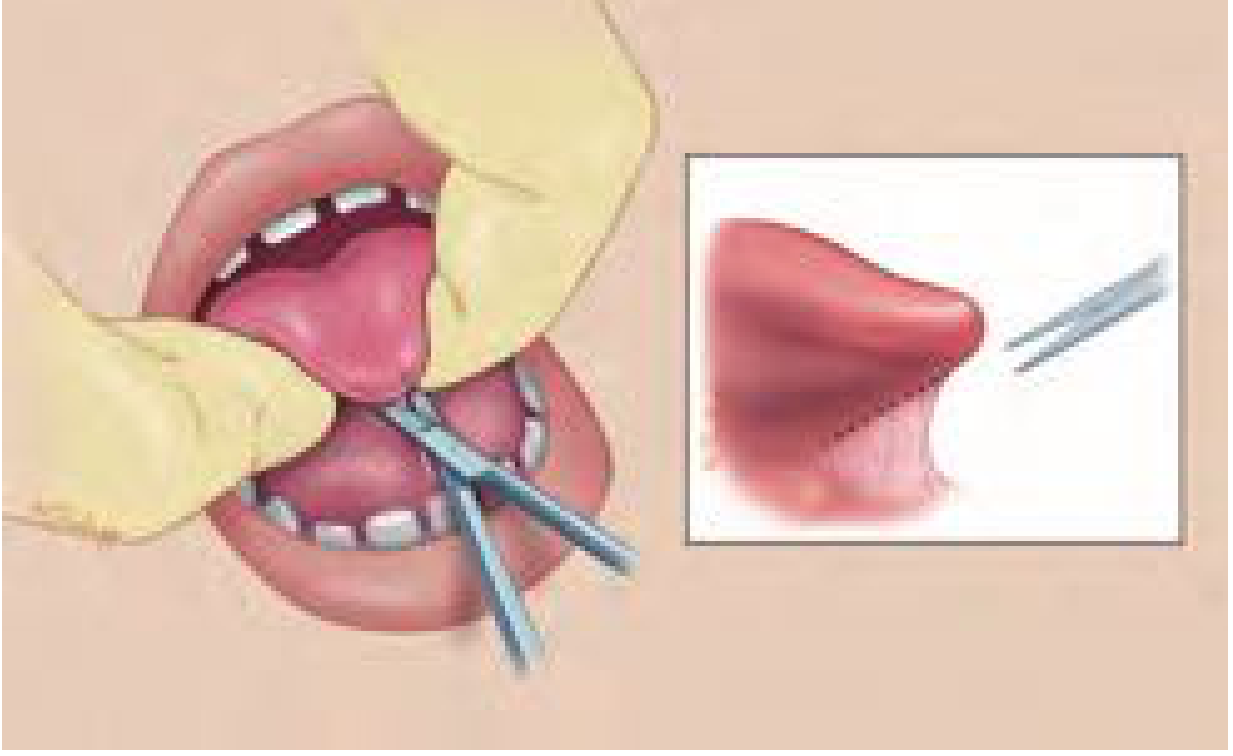
Frenulum is incised close to the undersurface of the tongue with care to avoid the submandibular (Wharton's) ducts
Steps:
- Infant is swaddled and positioned supine
- Tongue elevated with grooved director or two-fingered technique
- Frenulum is visualised - the avascular midline tissue is identified
- Sharp scissors divide the frenulum transversely, close to the tongue underside, parallel to and away from Wharton's ducts
- Results in a diamond-shaped wound (Fig. below) that heals by secondary intention
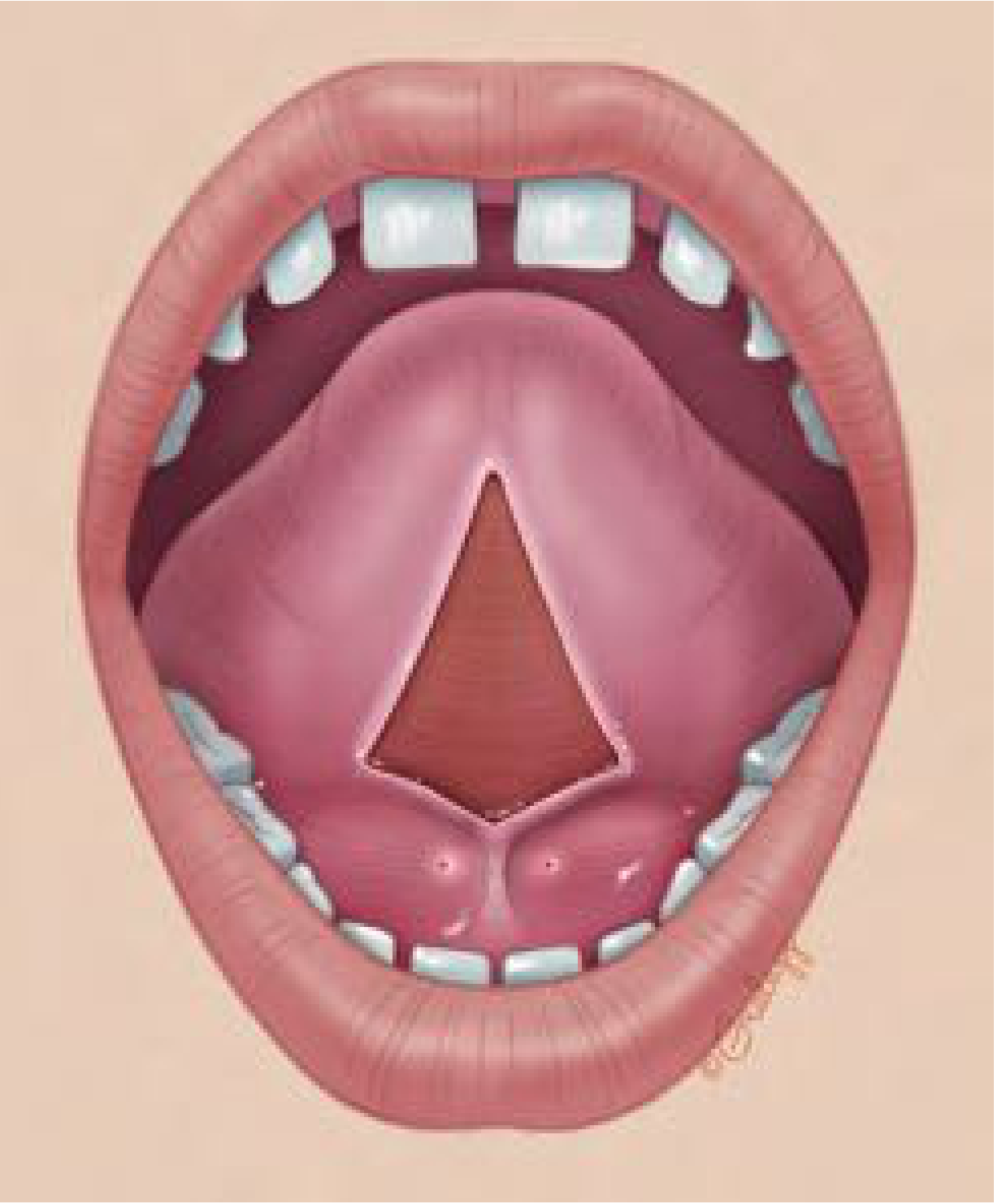
Diamond-shaped mucosal defect after frenotomy
Anaesthesia:
- Neonates: no general anaesthesia required - procedure done awake
- 24% oral sucrose is effective for procedural pain reduction in neonates
- Do NOT use topical lidocaine or benzocaine in neonates - FDA boxed warning due to risk of seizures and methemoglobinemia
- Older children: local infiltration or GA depending on age and compliance
Who performs it:
- Otolaryngologists, pediatricians, pediatric dentists, midwives/nurses
- Laser frenotomy (CO2 or diode) increasingly used by dentists
Frenuloplasty (Older Children/Adults)
Used when simple frenotomy is insufficient or when there is a posterior/thick frenulum.
- Performed under GA or outpatient local depending on patient age
- Z-plasty technique: vertical incision from gingival margin to vestibule, with two oblique incisions at 60 degrees - transposition of triangular flaps lengthens the floor of mouth
- Alternatively, the diamond-shaped defect after frenuloplasty can be closed with sutures (mucosal apposition) to prevent re-tethering
- Provides more durable release, especially for thick posterior ties
Complications
| Complication | Details |
|---|---|
| Bleeding | Most common; usually self-limited; occasionally persistent mild bleeding |
| Infection | Rare |
| Damage to Wharton's ducts | Submandibular duct injury → submandibular edema (rare) |
| Hypovolemic shock | Very rare case reports following significant bleeding |
| Recurrence / re-tethering | Occurs if wound edges re-approximate - more common with simple frenotomy without flap repair |
| Procedural pain/stress | Newborn pain has potential long-term neurodevelopmental implications - informed consent discussion |
Evidence and Outcomes
Breastfeeding (Primary Indication)
- A 2024 meta-analysis (PMID 37608056) found frenotomy produces a quantitative improvement in breastfeeding outcomes - maternal pain and infant latch scores improved
- A 2026 umbrella review (PMID 40990400) confirmed lingual frenotomy benefits breastfeeding infants
- The FROSTTIE RCT (PMID 37839892) - UK multicenter trial - compared frenotomy + breastfeeding support vs. breastfeeding support alone; found limited additional benefit of frenotomy over support alone for some outcomes, adding to ongoing debate
- The 2025 RCT (PMID 40319911) specifically examined lingual frenotomy in newborns with ankyloglossia
Speech
- Evidence for speech improvement after frenotomy is weaker - speech therapy is generally tried first
- Surgery is reserved for those failing therapy with confirmed structural restriction
Beyond Breastfeeding (Scoping Review, PMID 37606583)
- Evidence for ankyloglossia causing sleep-disordered breathing, TMJ disorders, and postural problems is insufficient and controversial
Key Points
- Ankyloglossia is common (up to 10%); functional impact is present in only a subset
- Type I/II (anterior) = easy to identify; Type III/IV (posterior) = often missed
- Neonatal frenotomy is a quick, safe, low-risk procedure without GA
- Avoid topical LA (lidocaine/benzocaine) in neonates - FDA warning
- Key risk during surgery: Wharton's ducts (submandibular duct orifices) just lateral to the frenulum base
- For older patients or thick/posterior ties, Z-plasty frenuloplasty provides more reliable release
- A multidisciplinary approach (ENT/paediatric dentist + lactation consultant + speech therapist) gives the best outcomes
Source: Cummings Otolaryngology Head and Neck Surgery, Chapter 207 - Ankyloglossia and Frenuloplasty
Indications and complications of endonasal dcr
Finding Sources
Searching PubMed
endonasal dacryocystorhinostomy indications complications
Finding Sources
Reading File
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.