
IMG_20260620_144503095_BURST0011.jpg
Inflammatory dis order of breast
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the content from Robbins Pathology. Here is the complete, detailed answer:
Inflammatory Disorders of the Breast
(From Robbins, Cotran & Kumar - Pathologic Basis of Disease, Chapter 23, p. 946-947)
Inflammatory diseases of the breast are rare - accounting for less than 1% of breast symptoms. They are caused by infections, autoimmune disease, or foreign body-type reactions to extravasated keratin or secretions. Inflammatory breast cancer clinically mimics inflammation and must always be excluded in a female presenting with an erythematous swollen breast.
1. Acute Mastitis
Etiology & Setting: Occurs almost exclusively during the first month of breastfeeding (lactational mastitis). Cracks and fissures in the nipple act as the portal of entry for:
- Staphylococcus aureus (most common) - leads to localized single/multiple abscesses
- Streptococci (less common) - causes spreading cellulitis
Clinical features: Breast erythema, pain, tenderness, and fever. Initially one duct system/sector is involved; if untreated, the infection can spread to the entire breast.
Treatment: Appropriate antibiotics + continued expression of milk. Surgical drainage is only rarely required.
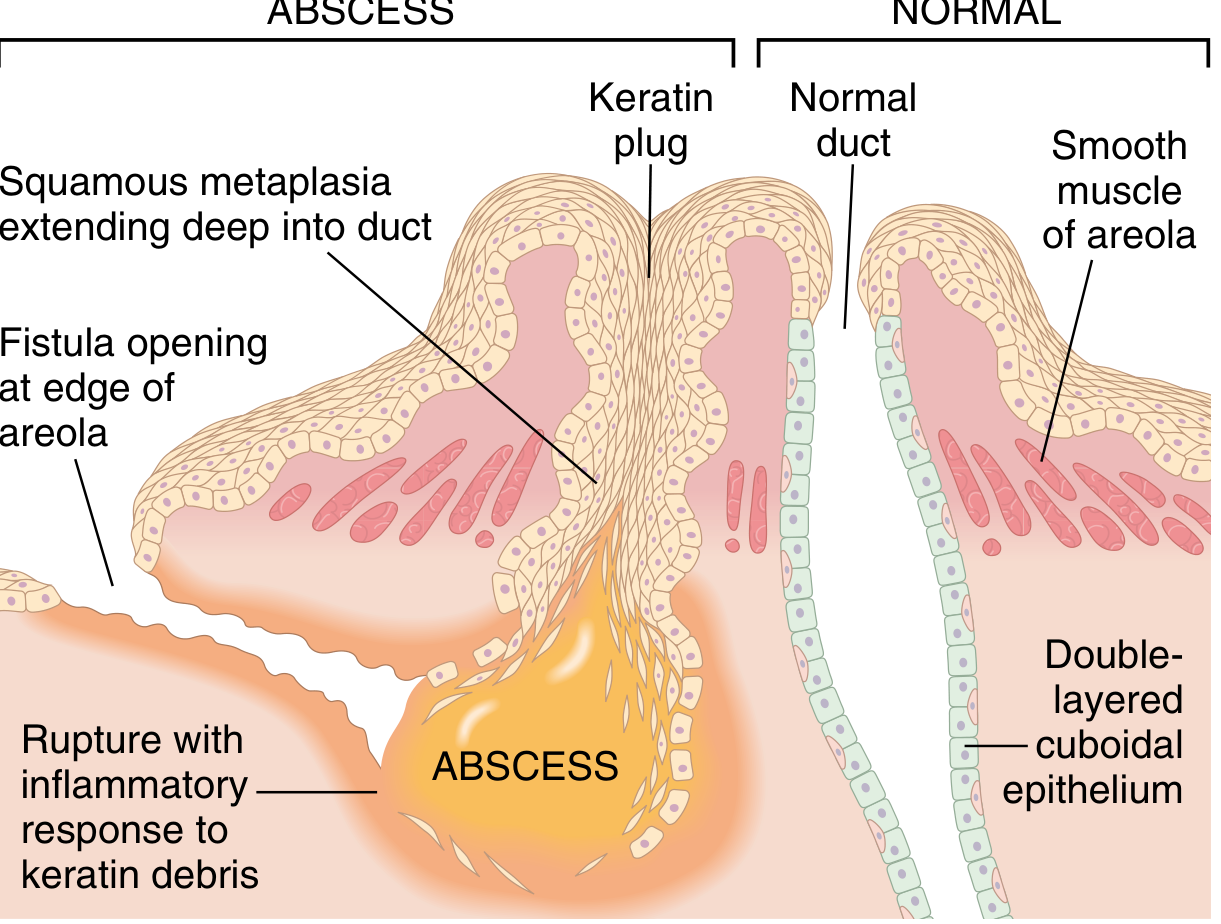
2. Squamous Metaplasia of Lactiferous Ducts
(also called: Recurrent subareolar abscess / Periductal mastitis / Zuska disease)
Pathogenesis: Keratinizing squamous metaplasia extends deep into the nipple duct past the normal squamocolumnar junction. Shed keratin is trapped, plugging the duct → dilation → rupture → intense chronic granulomatous inflammatory response to keratin spilling into periductal tissue.
Key association: >90% of affected individuals are smokers. Tobacco-associated relative vitamin A deficiency alters ductal epithelial differentiation.
Clinical features:
- Painful erythematous subareolar mass mimicking a bacterial abscess
- Recurrent fistula tract that burrows under the nipple smooth muscle and opens at the edge of the areola
- Nipple inversion due to traction from scarring
Treatment: En bloc surgical removal of the involved duct and fistula tract (simple incision and drainage alone leads to recurrence). Antibiotics if secondary bacterial infection is present.
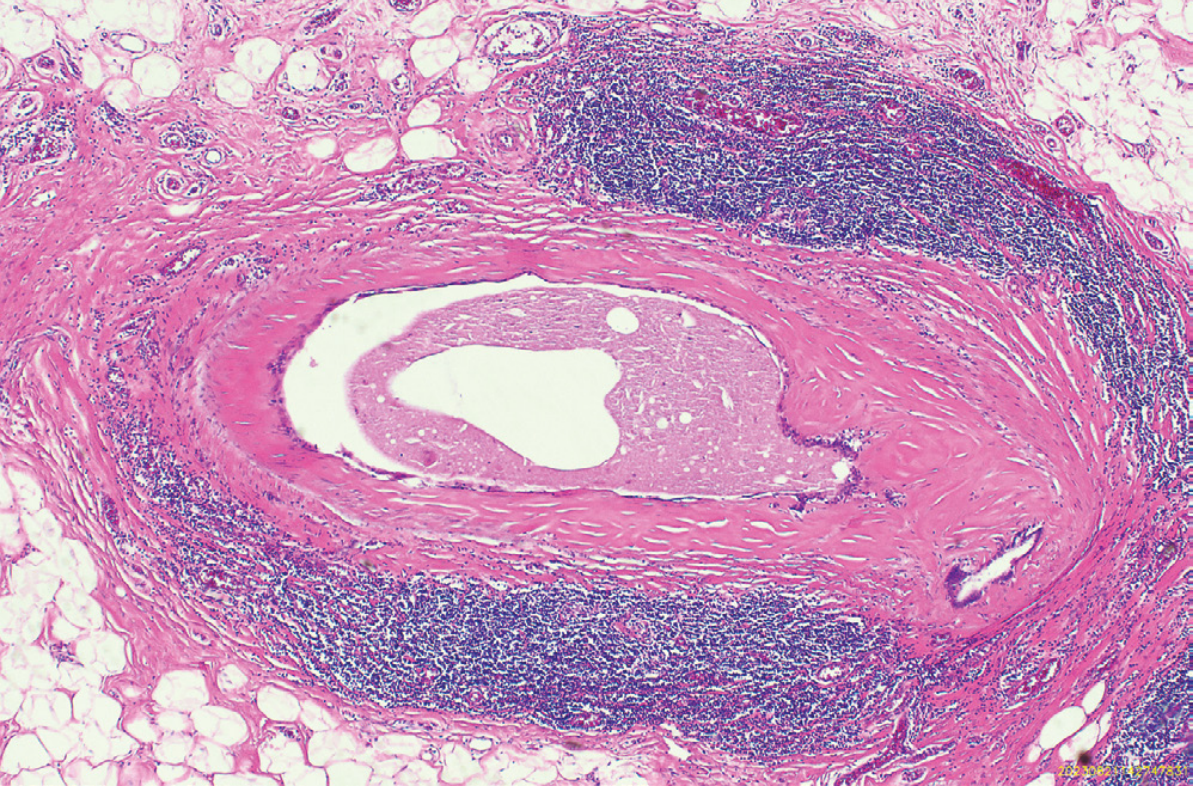
3. Duct Ectasia
Age/Setting: 5th-6th decade of life, multiparous females. NOT associated with cigarette smoking (distinguishes it from squamous metaplasia).
Clinical features:
- Palpable periareolar mass
- Thick, white nipple secretions
- Occasional skin retraction
- Pain and erythema are uncommon
- Can mimic invasive carcinoma clinically and radiologically
Morphology:
- Ectatic (dilated) ducts filled with inspissated secretions and numerous lipid-laden macrophages
- Duct rupture triggers chronic periductal/interstitial inflammation (lymphocytes, macrophages, plasma cells)
- Granulomas may form around cholesterol deposits
- Subsequent fibrosis produces an irregular mass with skin and nipple retraction
4. Fat Necrosis
Etiology: ~50% have history of breast trauma or prior surgery. The rest may be spontaneous (no identifiable cause).
Clinical features: Closely mimics cancer - presents as:
- Painless palpable mass
- Skin thickening or retraction
- Mammographic densities or calcifications
Morphology (evolving stages):
| Stage | Findings |
|---|---|
| Acute | Hemorrhagic, central liquefactive necrosis with neutrophils + macrophages |
| Subacute | Proliferating fibroblasts + chronic inflammatory cells surround the area |
| Late | Giant cells, calcifications, hemosiderin appear; lesion replaced by scar or encircled by fibrous tissue |
| Gross | Ill-defined, firm, gray-white nodules with small chalky-white foci |
5. Lymphocytic Mastopathy (Sclerosing Lymphocytic Lobulitis)
Clinical features: Single or multiple hard palpable masses or mammographic densities. Dense collagenized stroma may make needle biopsy difficult.
Morphology:
- Atrophic ducts and lobules with thickened basement membranes
- Surrounded by a lymphocytic infiltrate
- Densely collagenized stroma
Key associations:
- Type 1 diabetes (diabetic mastopathy) - most common
- Hashimoto thyroiditis
- Hypothesized to have an autoimmune basis
Clinical significance: Must be distinguished from breast cancer.
6. Granulomatous Mastitis
Causes:
- Systemic granulomatous diseases - granulomatosis with polyangiitis, sarcoidosis, tuberculosis
- Idiopathic granulomatous lobular mastitis - occurs only in parous females; granulomas closely associated with lobules and may contain lipid vacuoles surrounded by neutrophils
- Cystic neutrophilic granulomatous mastitis - similar histology; often caused by lipophilic Corynebacteria
- Localized infections - mycobacteria or fungi (rare; mainly in immunocompromised patients or around breast prostheses/nipple piercings)
Treatment: Antibiotics and sometimes corticosteroids.
Summary Table
| Condition | Age/Setting | Key Feature | Clinical Mimic |
|---|---|---|---|
| Acute Mastitis | Lactating women | S. aureus/streptococci | Abscess |
| Squamous Metaplasia | Smokers | Keratin plug → fistula | Abscess, nipple inversion |
| Duct Ectasia | 5th-6th decade, multiparous | White nipple discharge | Carcinoma |
| Fat Necrosis | Post-trauma/surgery | Chalky-white necrosis | Carcinoma |
| Lymphocytic Mastopathy | DM type 1 / Hashimoto | Dense collagenized stroma | Carcinoma |
| Granulomatous Mastitis | Parous females | Lobule-centered granulomas | Infection/abscess |
Key exam point: Duct ectasia, fat necrosis, and lymphocytic mastopathy can all mimic invasive carcinoma clinically and radiologically - biopsy is often required for definitive diagnosis.
- Robbins, Cotran & Kumar - Pathologic Basis of Disease, p. 946-947
- Schwartz's Principles of Surgery 11th Ed., p. 577
This is a shared conversation. Sign in to Orris to start your own chat.