Describe coronary circulator. And factors that alter blood flow in the coronary circulation .
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
I now have comprehensive information from multiple authoritative textbooks. Let me compile the full answer.
Coronary Circulation
1. Anatomical Overview
The coronary arteries arise from sinuses behind two cusps of the aortic valve at the root of the aorta. The main coronary arteries course along the epicardial surface of the heart, with smaller penetrating branches supplying the deeper myocardium. Only the innermost 0.1 mm of endocardial surface receives direct nutrition from intracavitary blood - this is physiologically negligible.
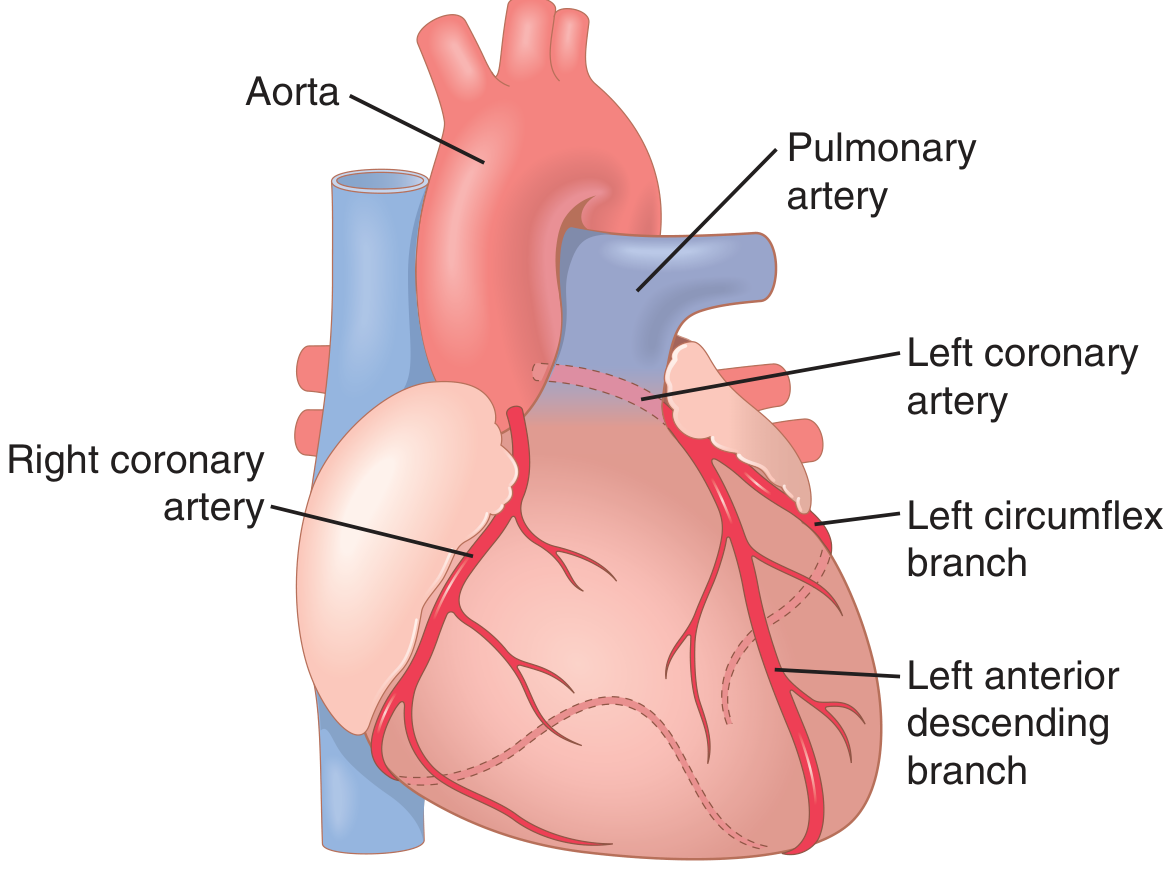
Coronary arteries and their branches (Guyton & Hall, Fig. 21.3)
Left Coronary Artery (LCA)
- Supplies the anterior and left lateral portions of the left ventricle
- Divides into the left anterior descending (LAD) branch and the left circumflex branch
Right Coronary Artery (RCA)
- Supplies most of the right ventricle
- Also supplies the posterior left ventricle in 80-90% of people ("right dominant" circulation)
Coronary Venous Drainage
- About 75% of left ventricular venous blood returns via the coronary sinus to the right atrium
- Most right ventricular blood returns through anterior cardiac veins directly into the right atrium
- A small amount drains via Thebesian veins (vv. cordis minimae), which empty directly into all four cardiac chambers
- Additionally, arteriosinusoidal vessels connect arterioles to chambers, and arterioluminal (arterio-luminal) vessels are small arteries draining directly into chambers
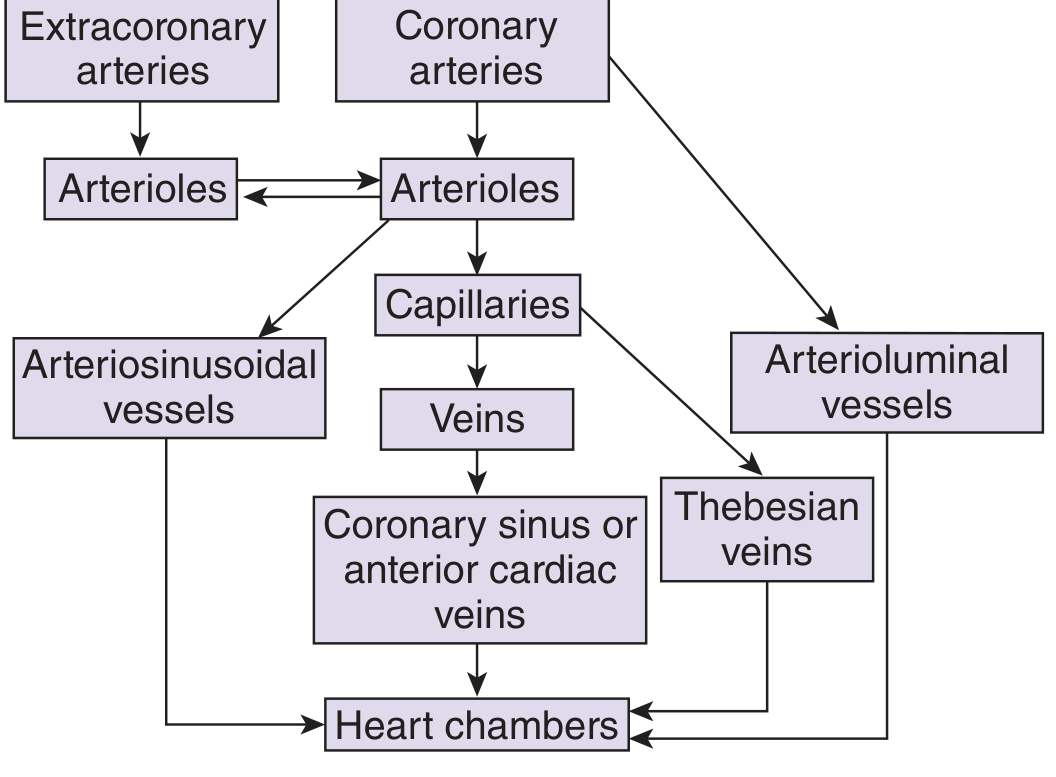
Diagram of the complete coronary circulation (Ganong's, Fig. 33-12)
2. Normal Coronary Blood Flow
- At rest: approximately 70 mL/min/100 g of heart weight, or about 225 mL/min total
- This equals roughly 4-5% of total cardiac output
- Coronary blood flow per gram is typically higher in women than in men
- During strenuous exercise, coronary flow increases 3-4 fold to meet the heart's increased oxygen demands (while cardiac work may increase 6-9 fold, making efficiency more important)
3. Epicardial vs. Subendocardial Perfusion
Epicardial coronary arteries supply the outer layers and penetrate inward. A subendocardial arterial plexus lies immediately beneath the endocardium:
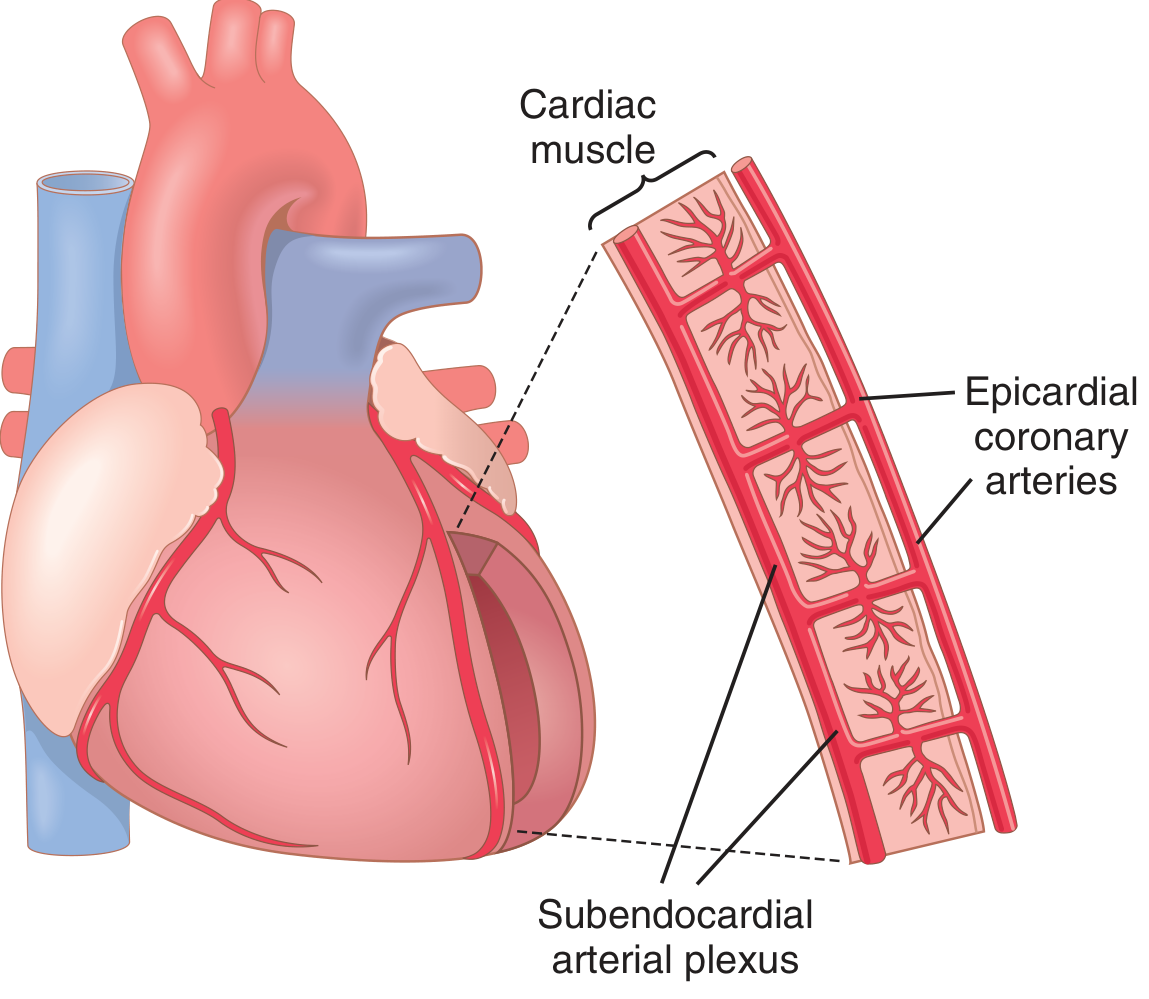
Epicardial, intramuscular, and subendocardial coronary vasculature (Guyton & Hall, Fig. 21.5)
The subendocardium is the most vulnerable region because:
- It bears the highest wall stress
- Its perfusion is most compromised during systole
- The extra vessels of the subendocardial plexus must compensate - any imbalance leads to subendocardial ischemia, which is the most common site of myocardial infarction
4. Phasic Nature of Coronary Blood Flow
The coronary circulation has a unique feature: it is compressed during systole, so the left ventricle is perfused almost exclusively during diastole.
| Phase | Left Coronary | Right Coronary |
|---|---|---|
| Systole | Flow falls sharply (near zero or briefly reversed) due to intramyocardial compression | Flow is only mildly reduced (RV pressure is low, ~25 mmHg) |
| Diastole | Maximum flow - fills during full diastole | Continuous flow through both phases |
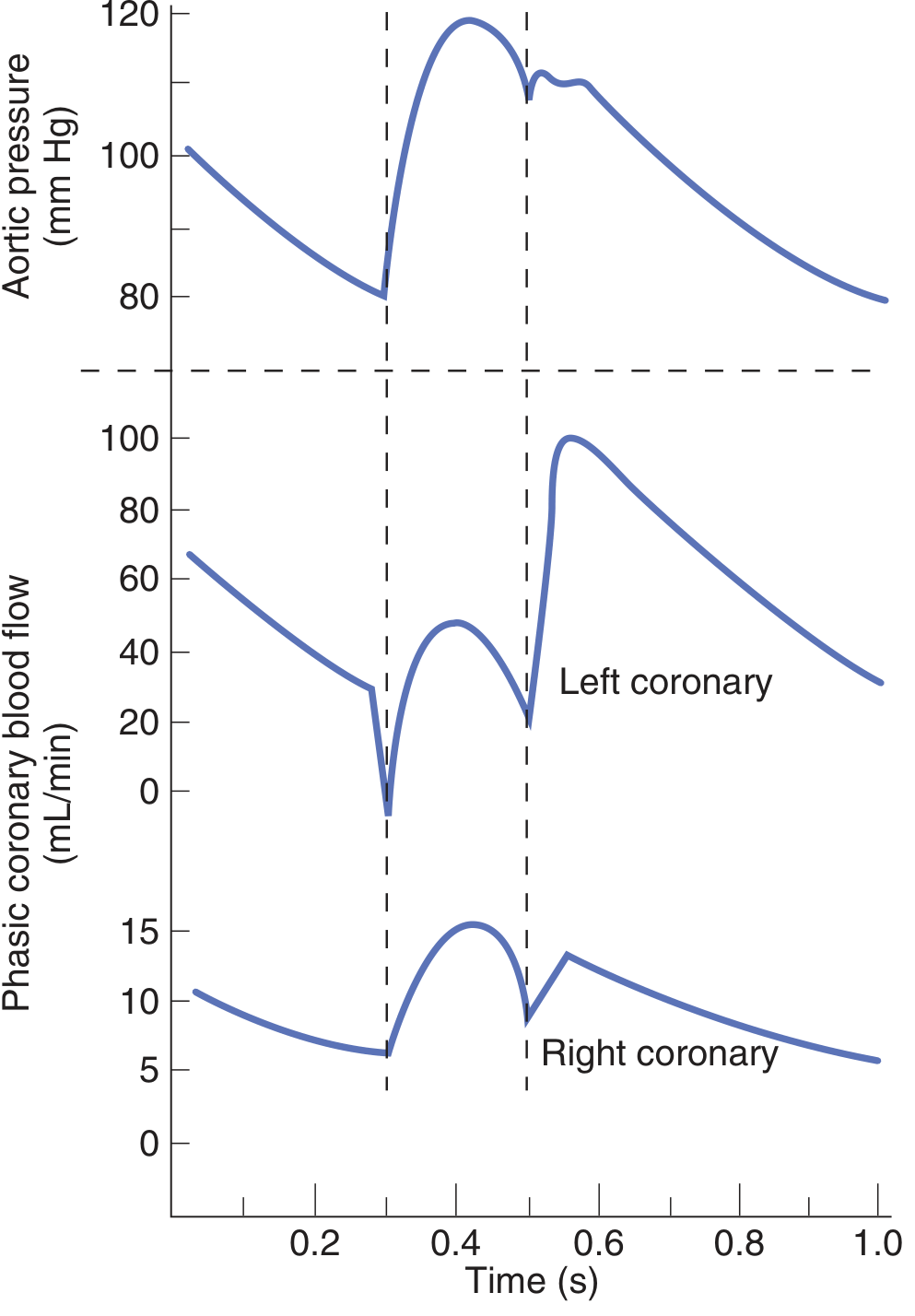
Phasic coronary blood flow in left and right coronary arteries during the cardiac cycle (Ganong's, Fig. 33-13)
The pressure differential explains this: during systole, left ventricular pressure (121 mmHg) actually slightly exceeds aortic pressure (120 mmHg), eliminating the driving gradient for subendocardial perfusion. During diastole, aortic pressure (80 mmHg) far exceeds LV pressure (0 mmHg), providing an 80 mmHg driving gradient.
5. Factors That Alter Coronary Blood Flow
A. Local Metabolic Factors (Primary Regulators)
This is the dominant control mechanism. The coronary circulation autoregulates almost entirely in response to local myocardial metabolism.
1. Oxygen demand / Hypoxia
- ~70% of oxygen delivered by coronary blood is extracted at rest (compared to ~25% in other tissues)
- This leaves almost no O2 reserve, so the only way to increase O2 delivery is to increase flow
- When O2 consumption rises (increased contractility, heart rate, wall stress), local tissue hypoxia triggers arteriolar vasodilation (active hyperemia)
- When O2 supply falls (reduced flow), reactive hyperemia restores flow after occlusion ends
2. Adenosine
- The most potent vasodilator in the coronary circulation
- When increased cardiac work depletes ATP → ATP → ADP → AMP → adenosine
- Adenosine diffuses out of cardiac cells and causes profound coronary arteriolar dilation
- Also the mechanism behind reactive hyperemia: adenosine accumulates during the ischemic period and causes a surge in flow once compression ends
3. Other local metabolites
- CO2 accumulation, H⁺ (lactic acidosis), decreased O2 tension
- Prostaglandins (particularly prostacyclin, PGI₂ - a vasodilator)
- Nitric oxide (NO) from endothelium - tonic vasodilation
These metabolic factors override all other control mechanisms. Even if nervous stimulation tends to constrict coronary vessels, metabolic vasodilation overcomes that vasoconstriction within seconds.
B. Aortic Diastolic Pressure (Perfusion Pressure)
- Since the left coronary artery fills almost entirely in diastole, the aortic diastolic pressure is the key perfusion pressure
- Reduced aortic diastolic pressure (e.g., aortic regurgitation, severe hypotension, shock) directly reduces coronary perfusion
- Elevated diastolic pressure (e.g., hypertension) increases coronary driving pressure
C. Heart Rate
- Tachycardia reduces left coronary flow by shortening diastole (the filling period)
- At high heart rates, less time is available for left ventricular diastolic filling, reducing net coronary flow
- This is especially significant when combined with increased O2 demand (exercise) or coronary stenosis
D. Intramyocardial / Extravascular Compression
- Ventricular wall tension during systole compresses intramural coronary vessels
- Greater wall tension = greater compression = greater impedance to flow
- Increased preload (higher LVEDV), increased afterload (aortic stenosis, hypertension), and hypertrophy all increase wall tension and worsen subendocardial perfusion
E. Autonomic Nervous System
Nervous control plays a secondary but important role:
Sympathetic stimulation:
- Direct effect: Epicardial coronary arteries have predominantly alpha-1 receptors (vasoconstriction); intramuscular arteries have more beta-2 receptors (vasodilation). Net direct effect is mild vasoconstriction
- Indirect (dominant) effect: Sympathetic activation increases heart rate and contractility → raises O2 demand → triggers metabolic vasodilation that far outweighs the direct constrictor effect
- Net result: sympathetic stimulation increases coronary flow overall via metabolic override
- In some individuals, disproportionate alpha vasoconstriction causes vasospastic angina
Parasympathetic (vagal) stimulation:
- Direct effect: acetylcholine causes direct coronary vasodilation
- Indirect effect: slows heart rate and slightly depresses contractility → reduces O2 consumption → indirectly reduces flow
- Net effect: vagal stimulation mildly reduces coronary flow (indirect dominates)
F. Coronary Perfusion Pressure (Autoregulation)
The coronary circulation exhibits autoregulation: flow remains relatively constant across a wide range of perfusion pressures (roughly 60-140 mmHg). Below 60 mmHg, autoregulation fails and flow falls linearly with pressure.
G. Cardiac Metabolism and Substrates
- At rest, the heart derives ~70% of its energy from fatty acid oxidation
- Under ischemia/hypoxia, the heart shifts to anaerobic glycolysis - much less efficient, produces lactic acid
- The increased demand for glucose and accumulation of lactate/H⁺ further stimulates vasodilation
H. Pathological Factors
- Coronary artery stenosis: A fixed stenosis limits maximal vasodilatory reserve. Patients may be asymptomatic at rest (autoregulation compensates) but develop ischemia on exertion when flow demand exceeds the limited maximum supply
- Coronary vasospasm: Abnormal alpha-adrenergic or endothelin-mediated constriction (Prinzmetal/variant angina)
- Increased venous pressure (heart failure): Reduces the pressure gradient across the coronary bed
- Aortic valve stenosis: Left ventricular systolic pressure must greatly exceed aortic pressure to eject blood, which both compresses coronary vessels more severely and increases O2 demand
Summary Table
| Factor | Effect on Coronary Flow |
|---|---|
| Increased O2 demand / hypoxia | Increase (vasodilation via adenosine/metabolites) |
| Adenosine | Strong increase |
| Increased aortic diastolic pressure | Increase |
| Tachycardia | Decrease (less diastolic time) |
| Systolic compression (LV) | Decrease during systole |
| Sympathetic stimulation | Net increase (metabolic override) |
| Vagal stimulation | Net mild decrease |
| Aortic stenosis | Decrease |
| Coronary artery stenosis | Decrease (limits reserve) |
| Reduced venous/right atrial pressure | Increase (improved gradient) |
Sources:
- Guyton and Hall Textbook of Medical Physiology, Chapter 21 (Coronary Circulation)
- Ganong's Review of Medical Physiology, 26th Ed., Chapter 33
- Costanzo Physiology, 7th Edition (Coronary Circulation section)
Can you give it as an answer for md anaesthesia question
Here is a structured MD Anaesthesia exam answer for this topic:
Coronary Circulation and Factors Affecting Coronary Blood Flow
Introduction
The coronary circulation is the vascular system that exclusively supplies the myocardium with oxygenated blood. It is unique among organ circulations because of its near-complete oxygen extraction at rest, phasic flow pattern, and predominant metabolic regulation. About one-third of all deaths in industrialized countries are due to coronary artery disease, making this one of the most clinically relevant topics in anaesthesia.
Anatomical Considerations
Arterial Supply
The two coronary arteries arise from sinuses behind the aortic valve cusps at the root of the aorta, just above the semilunar valve leaflets.
Left Coronary Artery (LCA)
- Arises from the left aortic sinus
- Divides almost immediately into:
- Left Anterior Descending (LAD) - supplies the anterior left ventricle, anterior interventricular septum, and apex
- Left Circumflex (LCx) - supplies the lateral and posterior left ventricle
- Supplies the anterior and left lateral portions of the left ventricle
Right Coronary Artery (RCA)
- Arises from the right aortic sinus
- Supplies most of the right ventricle
- Supplies the posterior left ventricle in 80-90% of individuals (right dominant circulation)
- Gives off the posterior descending artery (PDA) in right dominant hearts
Coronary Dominance:
- Right dominant: 80-90% (RCA gives PDA)
- Left dominant: 10-15% (LCx gives PDA)
- Co-dominant: 5%
Coronary Venous Drainage
| Vessel | Territory Drained | Drains Into |
|---|---|---|
| Coronary sinus | ~75% of LV venous blood | Right atrium |
| Anterior cardiac veins | RV venous blood | Right atrium directly |
| Thebesian veins (vv. cordis minimae) | Small amount | All cardiac chambers |
| Arteriosinusoidal vessels | Arterioles to chambers | Cardiac chambers |
Anatomical Layers of Coronary Vasculature
- Epicardial coronary arteries: Large conduit vessels on the heart surface; act as capacitance vessels; site of atherosclerosis
- Intramuscular arteries: Penetrate from epicardium into myocardium; primary resistance vessels
- Subendocardial arterial plexus: Lies immediately beneath the endocardium; most vulnerable to ischemia
Normal Coronary Blood Flow
- At rest: 70 mL/min/100 g heart weight, total approximately 225 mL/min
- Represents 4-5% of resting cardiac output
- At rest: approximately 70% of delivered oxygen is extracted (cf. ~25% in other tissues)
- This near-maximal extraction means the only mechanism to increase O2 delivery is to increase flow
- During maximal exercise: flow increases 3-4 fold
Phasic Nature of Coronary Blood Flow
This is a distinguishing feature of the coronary circulation, highly relevant to anaesthesia.
Left Coronary Artery:
- During systole: LV intramyocardial pressure (121 mmHg) slightly exceeds aortic pressure (120 mmHg) → pressure gradient reverses → flow falls to near zero or briefly reverses
- During diastole: Aortic pressure (80 mmHg) greatly exceeds LV pressure (0 mmHg) → 80 mmHg driving gradient → most left coronary flow occurs in diastole
Right Coronary Artery:
- RV systolic pressure is only ~25 mmHg → aorta-to-RV gradient remains positive even in systole (95 mmHg)
- Flow occurs in both systole and diastole, with only partial reduction in systole
Clinical implication: Tachycardia reduces diastolic time and therefore left coronary perfusion, while simultaneously increasing myocardial O2 demand - a double insult in coronary artery disease.
Factors Altering Coronary Blood Flow
1. Local Metabolic Factors (Primary / Dominant Mechanism)
The coronary circulation is regulated almost entirely by local myocardial metabolism. Metabolic vasodilation overrides all neural and humoral influences.
Oxygen demand and tissue hypoxia
- When myocardial work increases → increased O2 consumption → local hypoxia → arteriolar vasodilation → increased coronary flow (active hyperemia)
- When coronary occlusion is transiently relieved → surge in flow proportional to the O2 debt accumulated (reactive hyperemia)
Adenosine (most potent coronary vasodilator)
- Mechanism: Increased myocardial work → ATP degraded to ADP → AMP → adenosine
- Adenosine diffuses out of myocytes and causes profound arteriolar vasodilation
- Adenosine is the principal mediator of both active and reactive hyperemia in the coronary circulation
- Basis for pharmacological coronary stress testing (adenosine/dipyridamole)
Other metabolic vasodilators
- CO2 accumulation, H⁺ (lactic acidosis), decreased O2 tension
- Nitric oxide (NO) from endothelium - tonic vasodilation
- Prostacyclin (PGI2) - endothelial vasodilator
2. Aortic Diastolic Pressure (Perfusion Pressure)
- Coronary perfusion pressure (CPP) = Aortic diastolic pressure - Left ventricular end-diastolic pressure (LVEDP)
- Since the LV is perfused in diastole, aortic diastolic BP is the driving pressure
- Conditions that reduce CPP and impair coronary flow:
- Hypotension (shock, induction of anaesthesia)
- Aortic regurgitation (low diastolic BP + elevated LVEDP)
- Elevated LVEDP (heart failure, LV hypertrophy)
- Tachycardia (reduces diastolic time)
3. Heart Rate
- Tachycardia decreases diastolic filling time → reduces left coronary blood flow
- Simultaneously increases myocardial O2 demand
- This is the most dangerous combination in ischaemic heart disease patients
- Anaesthetic goal: avoid tachycardia in patients with coronary artery disease
4. Intramyocardial / Extravascular Compression
- Ventricular wall tension during systole compresses intramural coronary vessels
- Increased by: high preload (elevated LVEDV), high afterload (hypertension, aortic stenosis), ventricular hypertrophy
- The subendocardium is most vulnerable because wall tension is highest at the inner layer
- Subendocardium is the most common site of myocardial infarction
5. Autonomic Nervous System
Sympathetic stimulation:
| Effect Type | Mechanism | Result |
|---|---|---|
| Direct | NE on alpha-1 receptors (epicardial vessels) | Vasoconstriction |
| Direct | NE/Epi on beta-2 receptors (intramuscular arteries) | Vasodilation |
| Indirect (dominant) | Increased HR and contractility → increased O2 demand → metabolic vasodilation | Net increase in flow |
- Net result: sympathetic stimulation increases coronary flow via metabolic override
- In susceptible individuals, disproportionate alpha vasoconstriction causes coronary vasospasm (Prinzmetal's angina)
Parasympathetic (vagal) stimulation:
- Direct: acetylcholine causes direct vasodilation of coronary arteries
- Indirect: reduces HR and contractility → decreased O2 demand → reduced metabolic drive → flow decreases
- Net result: mild decrease in coronary flow (indirect effect dominates)
6. Coronary Autoregulation
- Coronary flow is maintained relatively constant over a perfusion pressure range of 60-140 mmHg
- Below 60 mmHg (or above 140 mmHg), autoregulation fails and flow becomes pressure-dependent
- Mechanism: myogenic response (intrinsic smooth muscle) + metabolic feedback
- In severe coronary artery stenosis, vasodilatory reserve is exhausted at rest → any further reduction in perfusion pressure causes ischemia
7. Pharmacological Agents Relevant to Anaesthesia
| Agent | Effect on Coronary Flow | Mechanism |
|---|---|---|
| Volatile anaesthetics | Vasodilation (direct) + ↓ O2 demand | Multiple; may cause coronary steal in CAD |
| Nitrates | Vasodilation (mainly venodilation) | NO donor; ↓ preload, ↓ LVEDP; dilate epicardial arteries |
| Beta-blockers | Increase flow (indirectly) | ↓ HR → ↑ diastolic time; ↓ O2 demand |
| Vasopressors (alpha agonists) | May reduce flow (vasoconstriction) | Alpha-1 mediated constriction |
| Adenosine / dipyridamole | Strong vasodilation | Direct on A2 receptors / inhibits adenosine breakdown |
| Calcium channel blockers | Vasodilation | ↓ smooth muscle tone in coronary arteries |
8. Other Pathological Factors
- Coronary artery stenosis: Limits maximum vasodilatory reserve; resting flow maintained by autoregulation until stenosis >70% diameter; flow reserve exhausted on exertion
- Coronary vasospasm: Exaggerated alpha-adrenergic or endothelin-mediated constriction
- Elevated right atrial/venous pressure: Reduces coronary outflow gradient (as in cardiac tamponade, PEEP, heart failure)
- Aortic stenosis: Increased wall stress + systolic compression + LV hypertrophy → severe subendocardial ischemia risk
- Anaemia: Reduces O2-carrying capacity → compensatory vasodilation to maintain O2 delivery
Anaesthetic Relevance - Summary Points
- Maintain heart rate in the 50-70 range in ischaemic heart disease - tachycardia is the enemy
- Maintain diastolic BP - this is the coronary driving pressure; hypotension during induction is dangerous
- Avoid increases in LVEDP - rises with volume overload, failure, or myocardial depression
- Tachycardia + hypotension = most dangerous combination in CAD (reduces CPP and diastolic time simultaneously)
- Coronary steal (with volatile agents/vasodilators) occurs when flow is diverted away from areas beyond a fixed stenosis
- Beta-blockers protect by reducing HR, prolonging diastole, and reducing O2 demand
References: Guyton and Hall Textbook of Medical Physiology | Ganong's Review of Medical Physiology, 26th Ed. | Costanzo Physiology, 7th Ed. | Miller's Anaesthesia, 10th Ed.
Define cardiac output . What are the factors affecting cardiac output . Determinants of CO . For MD anaesthesia exam
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Loading Image
I now have comprehensive material from Guyton, Costanzo, and Miller's. Let me compile the full MD Anaesthesia exam answer.
Cardiac Output: Definition, Determinants and Factors Affecting It
Definition
Cardiac output (CO) is the volume of blood ejected by one ventricle into the aorta (or pulmonary artery) per minute. It is the product of stroke volume and heart rate.
CO = Stroke Volume (SV) × Heart Rate (HR)
- Normal resting CO: ~5 L/min (range 4-8 L/min) in a 70 kg adult
- Stroke volume: ~70 mL/beat; Heart rate: ~72 beats/min
- Cardiac Index (CI) = CO ÷ Body Surface Area = ~3 L/min/m² (normalises for body size)
- CI is a better clinical comparator than absolute CO
Related terms:
- End-diastolic volume (EDV): Volume in ventricle at end of diastole (~140 mL)
- End-systolic volume (ESV): Volume remaining after ejection (~70 mL)
- Stroke volume = EDV - ESV = 140 - 70 = 70 mL
- Ejection fraction (EF) = SV/EDV = 70/140 = 50-65% (normal >55%)
Measurement of Cardiac Output
1. Fick Principle
The most classic method. Based on conservation of mass:
CO = O2 consumption (VO2) / (CaO2 - CvO2)
where CaO2 = arterial O2 content, CvO2 = mixed venous O2 content.
2. Indicator Dilution Methods
- Dye dilution (indocyanine green): indicator injected into venous system, detected in arterial blood
- Thermodilution (PA catheter - Swan-Ganz): cold saline injected into RA, temperature change detected in pulmonary artery. Most widely used in clinical anaesthesia
3. Echocardiography (Doppler)
- CO = SV × HR, where SV = CSA(LVOT) × VTI(LVOT)
- Widely used intraoperatively with TEE/TTE
Four Primary Determinants of Cardiac Output
Cardiac output is determined by four factors - two intrinsic to the heart and two extrinsic:
| Determinant | Type | Primary Regulator |
|---|---|---|
| Preload | Extrinsic (loading condition) | Venous return / EDV |
| Afterload | Extrinsic (loading condition) | Systemic vascular resistance / wall stress |
| Contractility | Intrinsic | Sympathetic tone, calcium, inotropes |
| Heart Rate | Intrinsic | Autonomic nervous system |
1. PRELOAD
Definition: The degree of myocardial stretch at the end of diastole, just before contraction. Clinically represented by end-diastolic volume (EDV) or end-diastolic pressure (EDP).
Frank-Starling Law (Fundamental basis)
- The volume ejected per beat depends on the volume present at end-diastole
- As EDV increases → sarcomere stretch increases → greater overlap of actin-myosin cross-bridges → stronger contraction → higher SV
- This is the length-tension relationship applied to the whole ventricle
- Frank-Starling ensures cardiac output automatically equals venous return in steady state
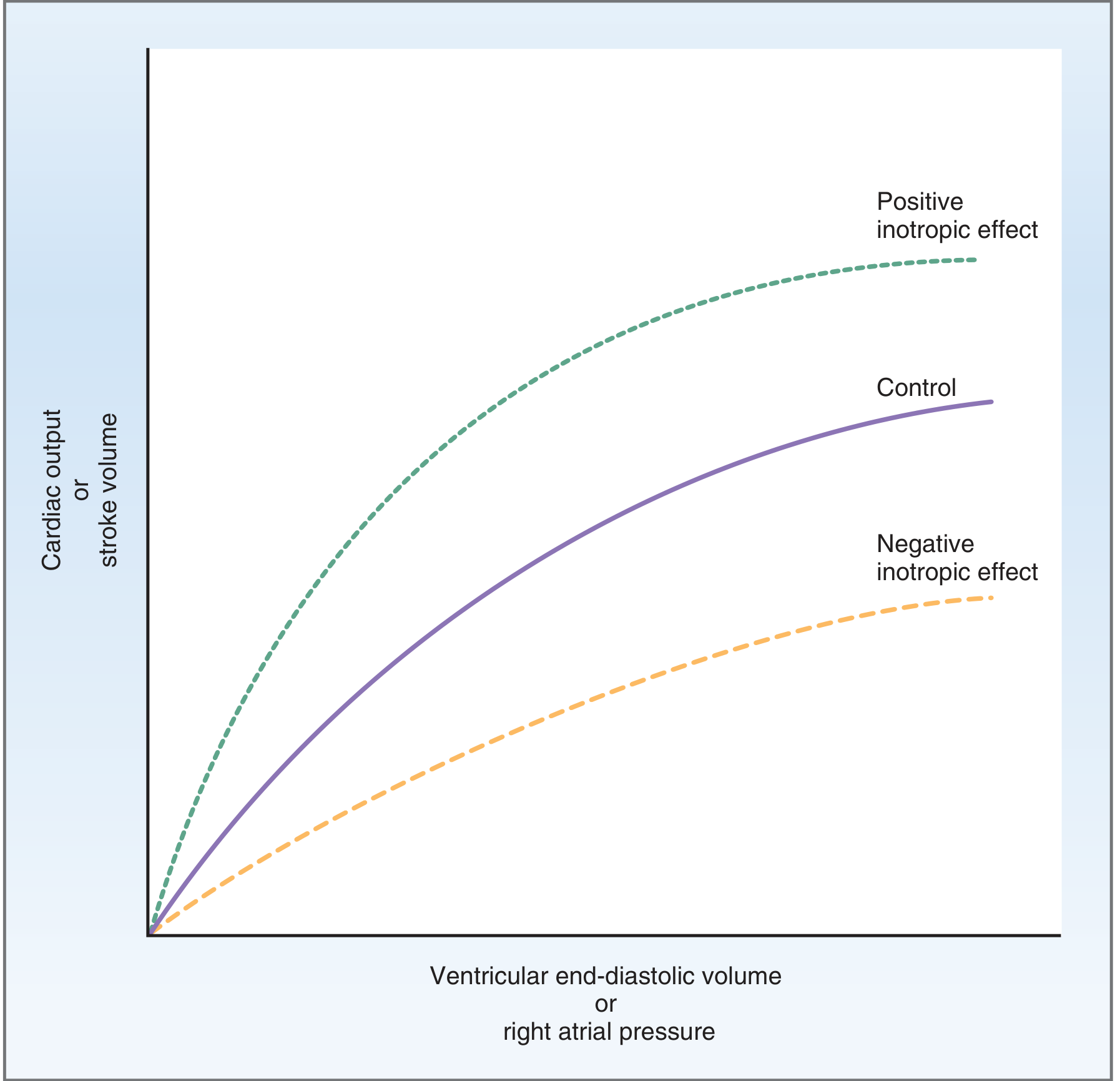
Positive inotropic agents shift the curve upward (higher SV for same EDV); negative inotropes shift it downward
Factors Increasing Preload (↑ EDV → ↑ CO)
- Increased venous return (exercise, autotransfusion, Trendelenburg position)
- Increased blood volume (IV fluids, pregnancy)
- Increased venomotor tone (sympathetic activation)
- Bradycardia (longer diastolic filling time)
- Mitral/tricuspid regurgitation (volume overload)
Factors Decreasing Preload (↓ EDV → ↓ CO)
- Haemorrhage, dehydration
- Vasodilators (nitrates, spinal/epidural anaesthesia → venodilation)
- Positive pressure ventilation / high PEEP (reduces venous return)
- Cardiac tamponade, tension pneumothorax (compresses cardiac chambers)
- Tachycardia (reduced diastolic filling time)
- Patient positioning (reverse Trendelenburg, sitting position)
Clinical Relevance to Anaesthesia
- Induction of anaesthesia typically reduces preload via venodilation and sympatholysis
- Positive pressure ventilation markedly reduces venous return and preload
- Fluid boluses increase preload - used to treat intraoperative hypotension
2. AFTERLOAD
Definition: The resistance the ventricle must overcome to eject blood - the load against which the ventricle contracts. Physiologically represented by:
- Systemic vascular resistance (SVR) for the LV
- Pulmonary vascular resistance (PVR) for the RV
- More precisely described by ventricular wall stress (LaPlace's law):
Wall Stress (σ) = (Pressure × Radius) / (2 × Wall Thickness)
LaPlace's Law - Key Points
- A dilated ventricle (↑ radius) faces higher wall stress for the same aortic pressure
- A hypertrophied ventricle (↑ wall thickness) has lower wall stress - this is why hypertrophy develops as a compensatory response to chronic pressure overload
Relationship to Stroke Volume
- Increased afterload → increased wall stress → reduced velocity of myocyte shortening → reduced stroke volume and CO
- The ventricle must do more work to generate the same SV against a higher afterload
Factors Increasing Afterload (↓ SV → ↓ CO)
- Hypertension, aortic stenosis
- Vasoconstriction (hypothermia, pain, sympathetic activation)
- Vasopressors (phenylephrine, norepinephrine)
- Ventricular dilation (heart failure - LaPlace's law)
Factors Decreasing Afterload (↑ SV → ↑ CO)
- Vasodilators (volatile agents, SNP, hydralazine)
- Sympathetic blockade (spinal/epidural anaesthesia)
- IABP (intra-aortic balloon pump) - reduces LV afterload by deflating during systole
- ACE inhibitors, calcium channel blockers
Clinical Relevance to Anaesthesia
- Volatile anaesthetics reduce SVR/afterload - beneficial in high-afterload states but can cause hypotension in already vasodilated patients
- Phenylephrine increases afterload - may reduce CO despite raising BP
- In heart failure, excessive afterload reduction must be balanced to avoid hypotension
3. CONTRACTILITY (Inotropy)
Definition: The intrinsic ability of the myocardium to generate force and shorten, independent of preload and afterload. It reflects the intensity of myocyte cross-bridge cycling and is determined by intracellular calcium availability.
- Contractility shifts the entire Frank-Starling curve up (positive) or down (negative)
- Clinically indexed by ejection fraction, dP/dt max (rate of LV pressure rise), or end-systolic pressure-volume relationship (ESPVR)
Cellular Mechanism
- Beta-1 adrenoceptor activation → ↑ cAMP → ↑ PKA activity → phosphorylation of L-type Ca²⁺ channels → ↑ Ca²⁺ entry → ↑ SR Ca²⁺ release → stronger actin-myosin cross-bridge formation
- Contractility correlates directly with cytosolic Ca²⁺ concentration
Factors Increasing Contractility (Positive Inotropes)
| Agent/Factor | Mechanism |
|---|---|
| Catecholamines (adrenaline, noradrenaline, dobutamine) | Beta-1 → ↑ cAMP → ↑ Ca²⁺ |
| Sympathetic stimulation | Same mechanism |
| Digoxin | Na⁺/K⁺-ATPase inhibition → ↑ intracellular Na⁺ → ↑ Ca²⁺ via NCX |
| Calcium (IV CaCl₂) | Direct ↑ Ca²⁺ |
| Milrinone (PDE inhibitor) | ↑ cAMP (inhibits breakdown) |
| Tachycardia (Bowditch/Treppe effect) | Increased Ca²⁺ cycling |
| Exercise | Sympathetic catecholamine release |
Factors Decreasing Contractility (Negative Inotropes)
| Agent/Factor | Mechanism |
|---|---|
| Volatile anaesthetics | ↓ Ca²⁺ release, ↓ myofilament sensitivity |
| Beta-blockers | Block beta-1 → ↓ cAMP → ↓ Ca²⁺ |
| Calcium channel blockers | Reduce Ca²⁺ entry |
| Acidosis | Reduces Ca²⁺ sensitivity of myofilaments |
| Hypoxia / ischaemia | ATP depletion, Ca²⁺ overload |
| Hyperkalaemia | Membrane depolarisation |
| Propofol | Ca²⁺ channel modulation |
| Heart failure / cardiomyopathy | Reduced beta-receptor density, Ca²⁺ cycling defects |
LV Pressure-Volume Loop - Effect of Contractility
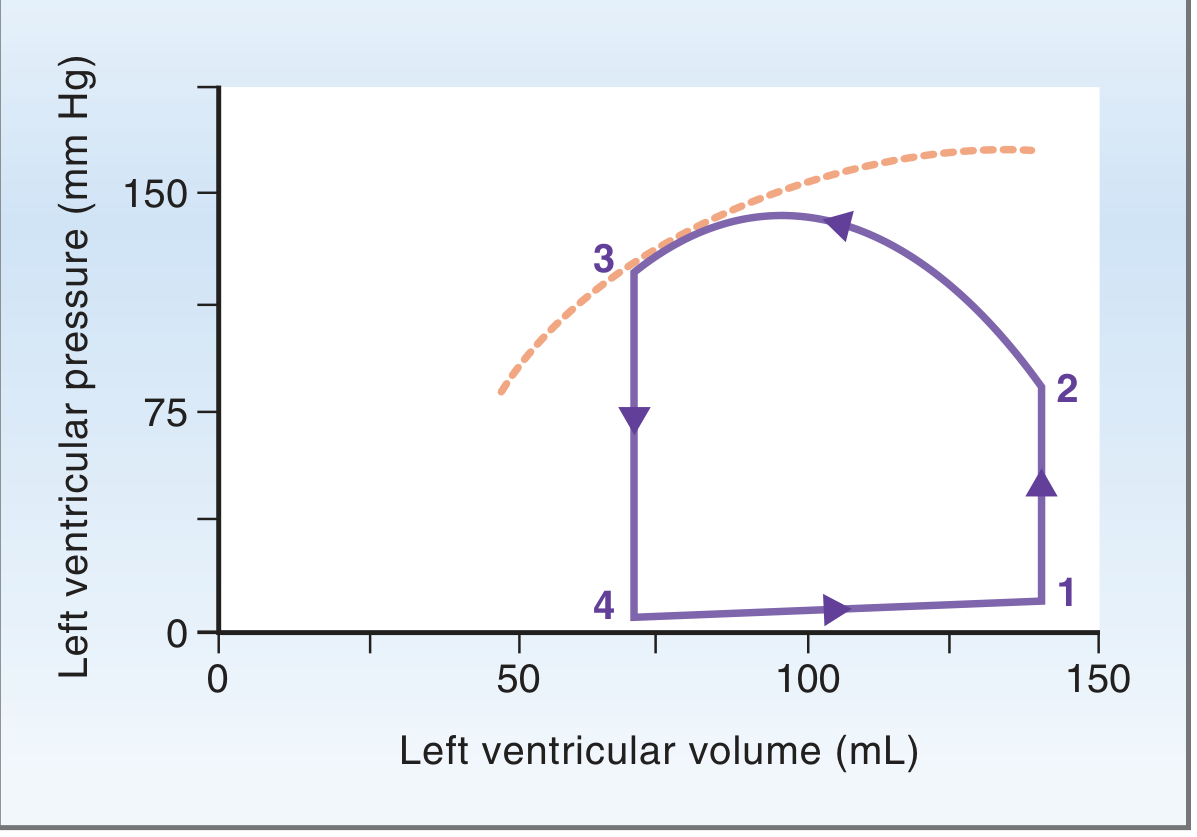
Points 1→2: isovolumetric contraction; 2→3: ejection; 3→4: isovolumetric relaxation; 4→1: filling. The width of the loop = stroke volume. Increased contractility shifts point 3 to a lower ESV and increases loop width.
4. HEART RATE
Definition: The number of ventricular contractions per minute. Normal: 60-100 beats/min.
CO = SV × HR
Heart rate has a direct and inverse relationship with CO - increases in HR increase CO up to a point, beyond which diastolic filling time is so short that SV falls and CO decreases.
Effect of Heart Rate on CO
| Heart Rate | Effect |
|---|---|
| Moderate tachycardia (100-150 bpm) | Initially ↑ CO (HR effect dominates) |
| Severe tachycardia (>150-180 bpm) | ↓ CO (SV falls due to inadequate filling and coronary ischaemia) |
| Bradycardia (<40-50 bpm) | ↓ CO despite large SV (HR effect dominates) |
Bainbridge Reflex
- Stretch of the right atrium (from increased venous return) increases heart rate via a vagal reflex arc through the medulla, ensuring CO keeps pace with venous return
Bowditch / Treppe Effect
- At higher heart rates, increased intracellular Ca²⁺ cycling increases contractility (positive inotropy from tachycardia)
Factors Increasing Heart Rate
- Sympathetic activation, catecholamines, pain, anxiety
- Hypovolaemia (reflex tachycardia)
- Drugs: atropine, ketamine, pancuronium, salbutamol
- Fever, thyrotoxicosis, anaemia
Factors Decreasing Heart Rate
- Vagal stimulation (laryngoscopy, oculocardiac reflex, peritoneal traction)
- Beta-blockers, digoxin, calcium channel blockers (non-dihydropyridine)
- Hypothermia, hypothyroidism
- High spinal anaesthesia (blocks cardiac accelerator fibres T1-T4)
- Increased ICP (Cushing's reflex - bradycardia with hypertension)
Other Factors Affecting Cardiac Output
5. Venous Return
- In the steady state, CO = venous return; they are equal and interdependent
- The heart cannot pump more than it receives (Frank-Starling)
- Venous return is driven by the mean systemic filling pressure (MSFP) gradient:
Venous Return = (MSFP - Right Atrial Pressure) / Venous Resistance
- Factors increasing venous return: increased blood volume, venoconstriction, skeletal muscle pump, respiratory pump (inspiration), Trendelenburg, exercise
- Factors decreasing venous return: venodilation (nitrates, epidural), positive pressure ventilation, hypovolaemia, tamponade
6. Autonomic Nervous System
| Stimulus | HR | Contractility | SVR | Net CO |
|---|---|---|---|---|
| Sympathetic (beta-1) | ↑ | ↑↑ | ↑ (alpha) | ↑↑ |
| Parasympathetic (vagal) | ↓↓ | ↓ (mild) | - | ↓ |
| Adrenaline (low dose) | ↑ | ↑↑ | ↓ (beta-2) | ↑↑ |
| Noradrenaline | ↑ (reflex ↓) | ↑ | ↑↑ | Variable |
7. Metabolic / Physiological States
| State | Change in CO | Mechanism |
|---|---|---|
| Exercise | ↑ (up to 4-7x) | ↑ HR + ↑ SV + ↑ venous return |
| Pregnancy | ↑ 30-50% by term | ↑ blood volume + ↑ HR + ↓ SVR |
| Fever/sepsis (early) | ↑ (hyperdynamic) | ↑ metabolic demand + ↓ SVR |
| Anaemia | ↑ | ↓ viscosity + ↑ HR + ↑ venous return |
| Hyperthyroidism | ↑ | ↑ HR + ↑ contractility + ↓ SVR |
| Hypothermia | ↓ | ↓ HR + ↓ contractility + ↑ viscosity |
| Hypovolaemia | ↓ | ↓ preload → ↓ SV |
| Heart failure | ↓ | ↓ contractility + ↑ afterload |
| AV fistula/Paget's disease | ↑ | ↓ peripheral resistance (shunting) |
8. Anaesthetic Agents and Their Effect on CO
| Agent | Preload | Afterload | Contractility | HR | Net CO |
|---|---|---|---|---|---|
| Halothane | - | ↓ | ↓↓ | ↓ | ↓↓ |
| Isoflurane | ↓ (venodil.) | ↓↓ | ↓ | ↑ (reflex) | Maintained |
| Sevoflurane | ↓ | ↓ | ↓ | - | Mild ↓ |
| Propofol | ↓↓ (venodil.) | ↓ | ↓ | - | ↓↓ |
| Ketamine | ↑ (sympath.) | ↑ | ↑ (indirect) | ↑↑ | ↑↑ |
| Etomidate | - | - | - | - | Neutral |
| Spinal/Epidural | ↓↓ (venodil.) | ↓ | - | ↓ (high) | ↓ |
| Dobutamine | ↑ (↑ CO) | ↓ (↑ CO) | ↑↑ | ↑ | ↑↑ |
Summary Diagram
CARDIAC OUTPUT = STROKE VOLUME × HEART RATE
|
┌────────────┼────────────┐
PRELOAD AFTERLOAD CONTRACTILITY
(EDV) (SVR/Wall (Inotropy)
Stress)
↑ ↑ ↑
Venous return Aortic BP Sympathetic
Blood volume SVR Catecholamines
Frank-Starling LaPlace Ca²⁺ availability
Key Normal Values (for exam)
| Parameter | Normal Value |
|---|---|
| Cardiac Output | 4-8 L/min |
| Cardiac Index | 2.5-4.0 L/min/m² |
| Stroke Volume | 60-100 mL/beat |
| Stroke Volume Index | 33-47 mL/beat/m² |
| Heart Rate | 60-100 beats/min |
| Ejection Fraction | >55% |
| SVR | 800-1200 dyn·sec·cm⁻⁵ |
| PVR | 100-250 dyn·sec·cm⁻⁵ |
| LVEDP | 6-12 mmHg |
References: Guyton and Hall Textbook of Medical Physiology | Costanzo Physiology, 7th Ed. | Miller's Anaesthesia, 10th Ed.
Bain bridge reflex . Short note for me anaesthesia exam .
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Excellent - I now have comprehensive, detailed information from four authoritative textbooks. Here is the complete MD Anaesthesia short note:
Bainbridge Reflex
Definition
The Bainbridge reflex (also called the atrial volume reflex or atrio-accelerator reflex) is a cardioacceleratory reflex in which an increase in right atrial pressure and stretch causes a reflex increase in heart rate, thereby helping the heart to "keep pace" with an increased venous return.
It was first described by Francis Arthur Bainbridge in 1915.
Receptor (Afferent Limb)
- Receptor type: Low-pressure mechanoreceptors (stretch receptors / volume receptors)
- Location: Right atrial wall and the cavoatrial junction (junction of the venae cavae with the right atrium)
- These are Type B atrial receptors - they fire in response to passive stretch of the atrial wall during filling
- They are distinct from arterial baroreceptors (high-pressure receptors in the carotid sinus and aortic arch)
- Stimulus: Increased right atrial filling pressure and wall stretch - caused by increased venous return / blood volume
Afferent Pathway
- Stretch receptor signals travel via vagal afferent fibres (CN X) to the nucleus tractus solitarius (NTS) in the medulla
- Signals then reach the cardiovascular centre in the medulla oblongata (cardioinhibitory and cardioacceleratory areas)
Efferent Pathway and Response
- The cardiovascular centre responds by:
- Inhibiting parasympathetic (vagal) outflow to the SA node - reduces vagal tone
- Increasing sympathetic outflow to the SA node and myocardium via cardiac sympathetic nerves
- Result: Tachycardia (increased heart rate)
- The effect on contractility and stroke volume is minimal - the primary response is on heart rate alone
Mechanism of Tachycardia - Two Components
| Component | Mechanism | Magnitude |
|---|---|---|
| Direct SA node stretch | Atrial stretch directly depolarises the SA node | ~15% increase in HR |
| Bainbridge reflex (neural) | Vagal afferent → medullary centre → sympathetic/vagal efferent | 40-60% increase in HR |
Physiological Significance
- Prevents congestion - prevents damming of blood in the veins, right atrium, and pulmonary circulation when venous return increases
- Matches CO to venous return - increases heart rate and therefore cardiac output to match the increased inflow; works in concert with the Frank-Starling mechanism
- Counterbalances the arterial baroreceptor reflex - the two reflexes work in opposition:
| Situation | Baroreceptor Reflex | Bainbridge Reflex | Net HR |
|---|---|---|---|
| ↑ Blood volume | ↓ HR (high arterial pressure → reflex bradycardia) | ↑ HR (atrial stretch → tachycardia) | Depends on dominance |
| ↓ Blood volume | ↑ HR (low arterial pressure → reflex tachycardia) | No activation (no atrial stretch) | ↑ HR |
- During volume loading, the Bainbridge reflex prevails and HR increases
- During volume depletion, the arterial baroreceptor reflex dominates and HR also increases
- Heart rate is at its minimum when circulating volume is normal (both reflexes balanced)
Important Features
- The magnitude of the heart rate increase is greatest when the baseline heart rate is slow (the reflex saturates at higher baseline rates)
- At fast baseline heart rates, infusion of fluids may paradoxically cause a small decrease in HR (arterial baroreceptors activated by rising BP dominate over the Bainbridge reflex)
- The Bainbridge reflex is not solely dependent on a neural arc - direct mechanical stretch of the SA node also contributes
- Efferent limb involves both sympathetic and parasympathetic pathways (primarily withdrawal of vagal tone + sympathetic activation)
Additional Atrial Stretch Responses (Clinically Linked)
Stretch of atrial low-pressure receptors also triggers (independent of Bainbridge reflex per se):
- ↓ ADH secretion (from hypothalamus) → increased water excretion
- ↓ Renal sympathetic tone → renal vasodilation → natriuresis and diuresis
- ↑ ANP (Atrial Natriuretic Peptide) release → natriuresis, diuresis, vasodilation
- Together these responses reduce blood volume back toward normal
Anaesthetic Relevance
| Clinical Scenario | Bainbridge Reflex Relevance |
|---|---|
| IV fluid bolus | Increases right atrial stretch → Bainbridge reflex → tachycardia; this is physiologically appropriate |
| Rapid blood transfusion | Same - tachycardia expected |
| Spinal/epidural anaesthesia | Venodilation reduces venous return → atrial stretch reduced → Bainbridge contribution withdrawn → bradycardia |
| Positive pressure ventilation / high PEEP | Reduces venous return and atrial stretch → can contribute to bradycardia and reduced CO |
| Positioning (Trendelenburg) | Increases venous return → ↑ atrial stretch → mild tachycardia |
| Cardiac tamponade | Despite raised CVP, effective atrial filling is impaired → reflex is not effectively activated |
| Heart transplant | Denervated heart - the neural arc of the Bainbridge reflex is absent; only the direct SA node stretch component persists |
Summary (for quick recall)
↑ Venous Return
↓
Right atrial stretch
↓
Type B low-pressure receptors (cavoatrial junction)
↓
Vagal afferents → NTS → Medullary cardiovascular centre
↓
↓ Vagal efferent tone + ↑ Sympathetic efferent
↓ ↓
SA node: direct stretch SA node stimulation
↓
↑ Heart Rate → ↑ Cardiac Output → prevents atrial congestion
References: Guyton and Hall Textbook of Medical Physiology | Miller's Anaesthesia, 10th Ed. | Costanzo Physiology, 7th Ed. | Boron & Boulpaep Medical Physiology
CVP monitoring
Finding Sources
Finding Sources
Reading File
Reading File
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.