Hemiplegic gait
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Reading File
I now have excellent content from Adams and Victor's Neurology. Let me compile the full answer.
Hemiplegic Gait
Hemiplegic gait (also called spastic hemiparetic gait) is the abnormal walking pattern resulting from unilateral upper motor neuron (UMN) damage, most commonly from stroke, traumatic brain injury, or any lesion to the corticospinal pathway on one side.
Pathophysiology
Damage to the corticospinal (pyramidal) tract on one side produces:
- Spasticity - velocity-dependent increase in muscle tone, predominantly in the flexors of the arm and extensors of the leg (the antigravity muscle groups)
- Weakness - particularly of dorsiflexors and hip flexors on the affected side
- Loss of fine, fractionated voluntary movement
The spastic extensor pattern in the leg means the limb is extended and stiff, unable to flex freely at the hip, knee, and ankle during the swing phase.
Clinical Features
Lower Limb (Affected Side)
- The leg is held stiffly extended - restricted flexion at the hip, knee, and ankle
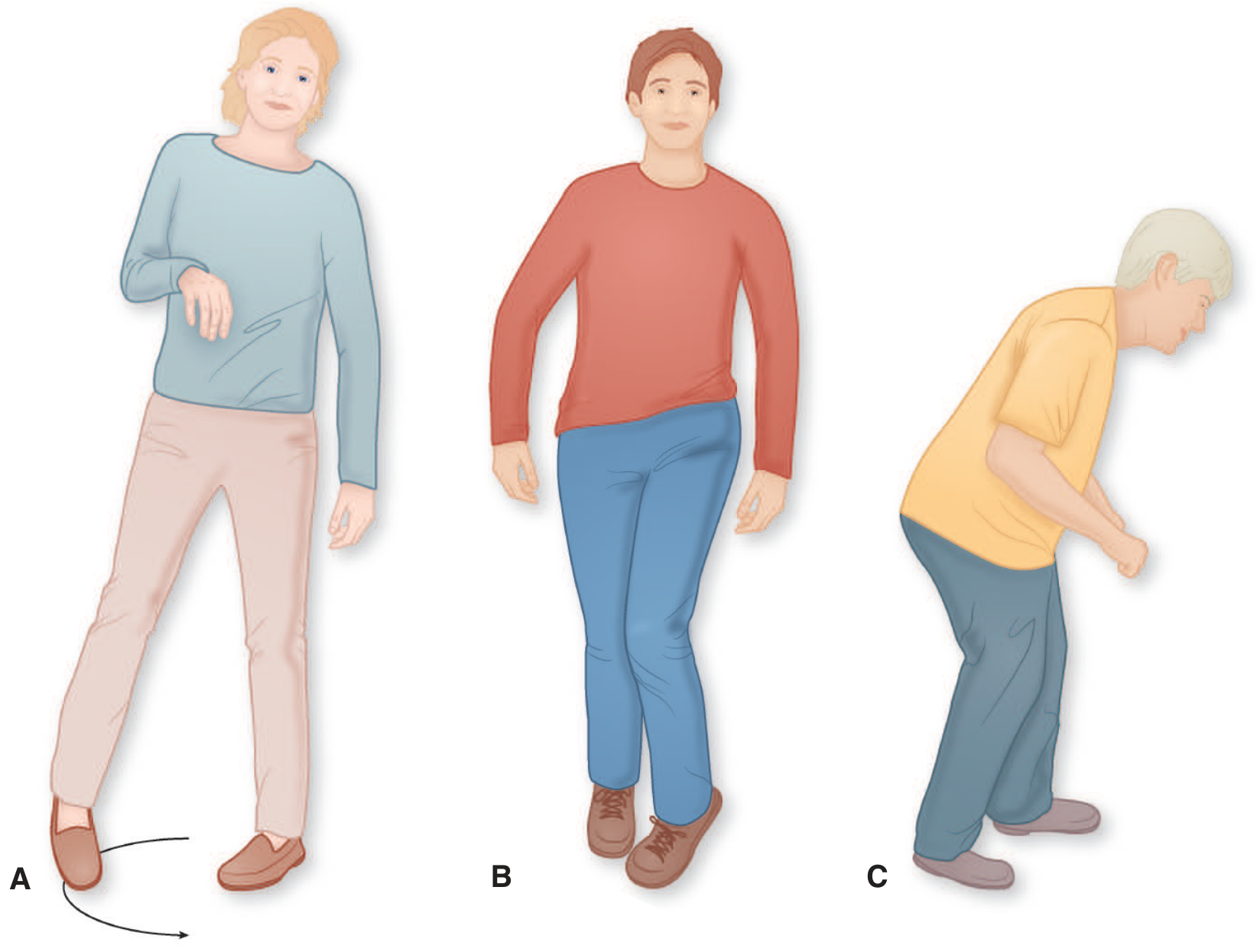
- During swing phase, the leg rotates outward in a semicircle (circumduction) - first away from then toward the trunk, to clear the floor
- The foot scrapes the floor, with contact made by the toe and outer heel
- Characteristic slow, rhythmic scuffing sound while walking
- The medial toe of the shoe shows preferential wear
Upper Limb (Affected Side)
- The arm is weak and stiff, carried in a flexed position
- It does not swing naturally during walking
- In hemiplegic children, the arm tends to abduct as the patient steps forward
Causes
This gait is most often a sequela of:
- Stroke (most common)
- Traumatic brain injury
- Any condition damaging the corticospinal pathway unilaterally - including brain tumors, demyelination, cervical cord lesions
Bilateral Form: Spastic (Scissor) Gait
When the lesion is bilateral (e.g., cerebral diplegia/Little disease, multiple sclerosis, spinal cord compression), the result is a bilateral hemiplegic gait - also called the scissor gait:
- Both legs advanced slowly and stiffly
- Thighs strongly adducted, causing legs to almost cross with each step
- Short, regular steps - patient walks "as though wading waist-deep in water"
- The defect is in stiffness of the stepping mechanism, not in support or equilibrium
Causes of spastic paraparetic gait include: cerebral diplegia (perinatal anoxia), multiple sclerosis, syringomyelia, subacute combined degeneration, spinal cord compression, adrenomyeloneuropathy, and familial spastic paraplegia.
Distinguishing Features from Other Gaits
| Gait | Key Feature |
|---|---|
| Hemiplegic | Unilateral circumduction, flexed arm, scuffing toe |
| Scissor/spastic | Bilateral stiff legs crossing (adduction), short steps |
| Steppage (foot drop) | Exaggerated hip flexion, foot hangs, slapping noise - no circumduction |
| Parkinsonian | Short shuffling steps, festination, forward-bent posture, no circumduction |
| Ataxic (cerebellar) | Wide-based, staggering, irregular steps |
Sources:
- Adams and Victor's Principles of Neurology, 12th Ed., pp. 137-138 - "Hemiplegic and Paraplegic (Spastic) Gaits"
- Harrison's Principles of Internal Medicine, 22nd Ed., p. 93
This is a shared conversation. Sign in to Orris to start your own chat.