
17839260046698910429578152020430.jpg
Give proper ans with deep research with image
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive material from Bailey and Love's Surgery 28th Edition. Let me compile the full, detailed answer.
Varicose Vein with Venous Ulcer - Complete Long Answer
Source: Bailey and Love's Short Practice of Surgery, 28th Edition
i. Provisional Diagnosis with Reasons
Diagnosis: Varicose veins of the left lower limb with venous (stasis) ulcer at the medial malleolus
Reasons supporting this diagnosis:
| Feature | Significance |
|---|---|
| 50-year-old male, bus conductor (prolonged standing) | Occupation involving prolonged standing is a recognized risk factor for varicose veins |
| Pain and swelling in the left lower limb | Classic symptoms of chronic venous hypertension |
| Aggravation in the evening | Venous symptoms typically worsen with gravity through the day and with prolonged standing |
| Swelling along the course of the great saphenous vein | Varicose veins in the GSV territory - subcutaneous dilated veins ≥3 mm in the medial aspect of limb |
| 3 x 4 cm ulcer near medial malleolus | Venous ulcers characteristically develop in the gaiter area (between calf and ankle), predominantly on the medial side near Cockett perforators connecting the posterior tibial vein to the posterior arch vein |
Pathophysiology: Prolonged standing leads to venous incompetence (valvular dysfunction), causing retrograde flow (reflux) and sustained venous hypertension. This results in:
- Pericapillary fibrin cuff formation
- Leukocyte trapping and free radical generation
- Proteolytic enzyme activation
- Fibroblast senescence
- Ultimately - ulceration in the gaiter region
Venous disease accounts for ~85% of all chronic lower limb ulcers. Ambulatory venous hypertension is the only accepted underlying cause of venous ulceration. - Bailey and Love, p. 1061
ii. Course of the Great Saphenous Vein with Tributaries
Course of the GSV
The GSV is the longest vein in the body and the most frequently affected by superficial incompetence:
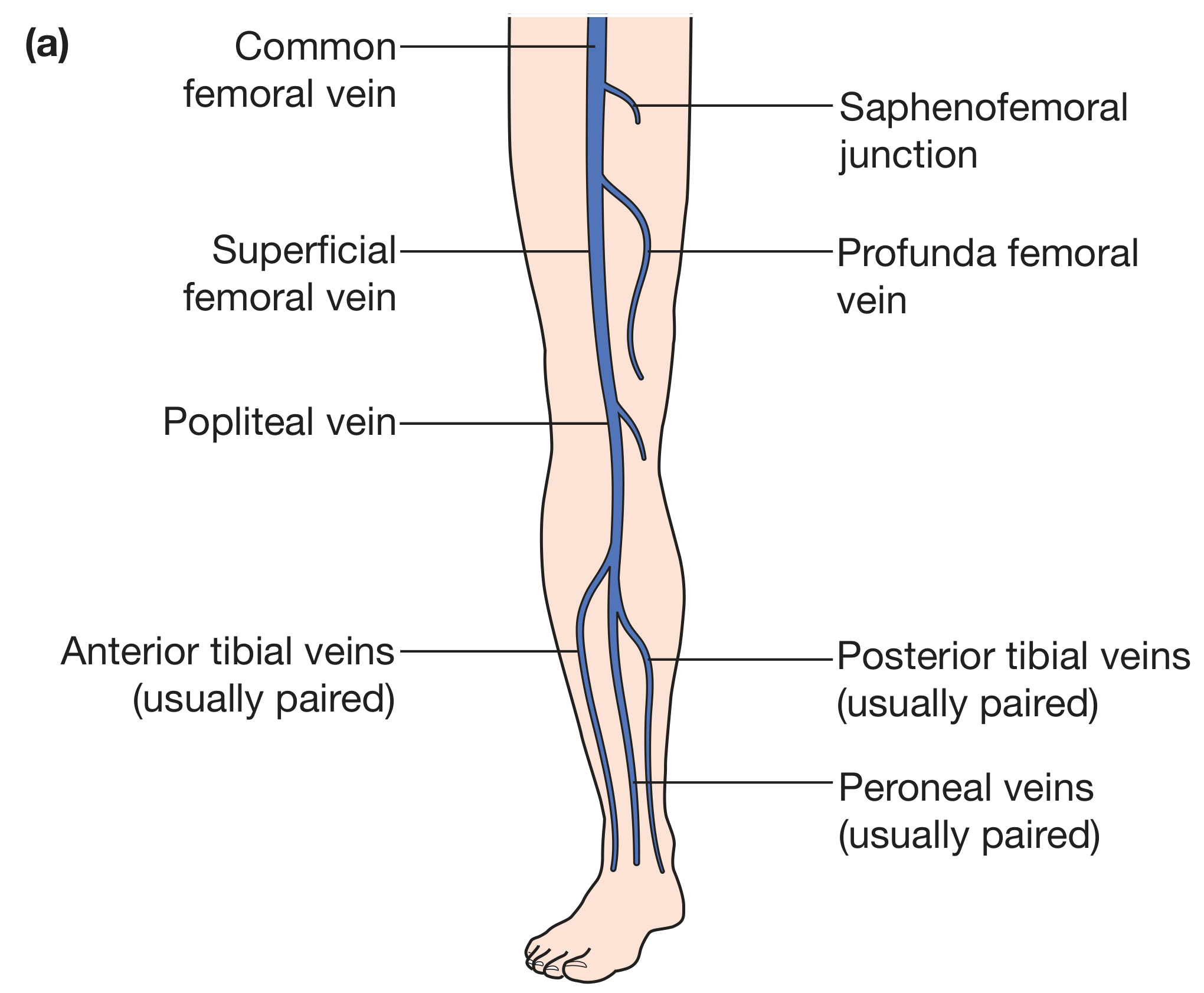
Origin:
- Arises from the medial end of the dorsal venous arch of the foot
Leg (Crus):
- Passes anterior to the medial malleolus
- Ascends the leg in the superficial tissues medial to the tibia
- Accompanied by the saphenous nerve (a branch of the femoral nerve)
- Loops posteriorly at the level of the medial condyle of the femur
Thigh:
- Continues in the medial thigh (the saphenous compartment/envelope, between the saphenous fascia and deep fascia)
- In the proximal thigh, it may be accompanied by the anterior accessory of the great saphenous vein (AAGSV) running anterolaterally
Groin (Termination):
- Pierces the cribriform fascia covering the saphenous opening (approximately 2.5 cm below and lateral to the pubic tubercle)
- Terminates by draining into the common femoral vein (CFV) at the saphenofemoral junction (SFJ)
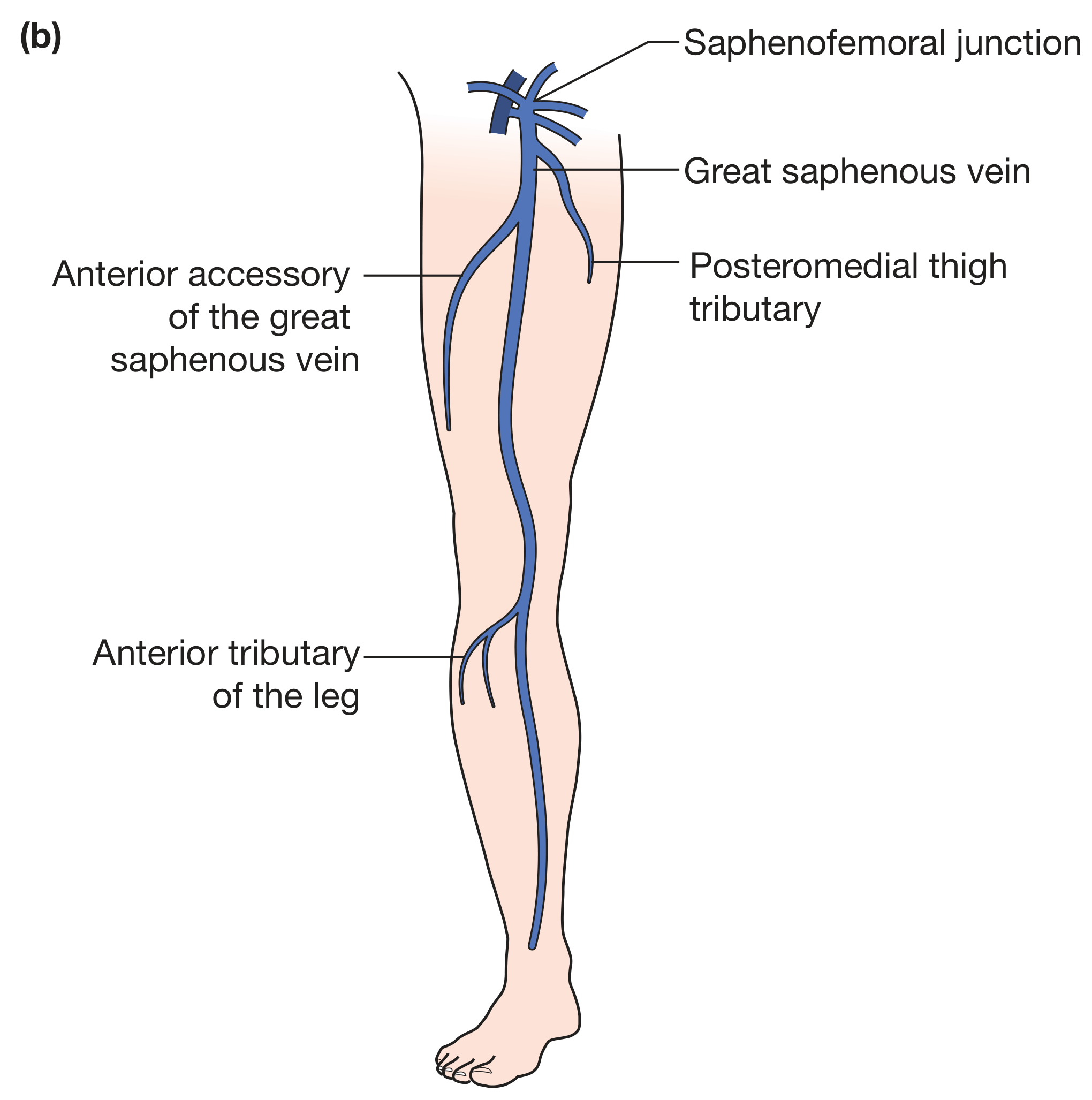
Tributaries at the Saphenofemoral Junction (Groin)
Six major tributaries are encountered at the SFJ:
Laterally:
- Superficial inferior epigastric vein
- Superficial circumflex iliac vein
Medially:
3. Superficial external pudendal vein
4. Deep external pudendal vein
Distally:
5. Anterior accessory of the great saphenous vein (AAGSV)
6. Posteromedial thigh vein
Tributaries in the Thigh and Leg:
- Posteromedial thigh tributary
- Anterior tributary of the leg
- Variable superficial tributaries throughout its course
- Connects to deep system via perforating (communicating) veins - the most important being the Cockett perforators (direct perforating veins of the medial calf connecting to posterior tibial vein)
iii. Investigation to Confirm Diagnosis
Duplex Ultrasound Scanning (Colour Doppler)
This is the single most important investigation for this patient.
Why duplex ultrasound?
- Tourniquet tests and hand-held Doppler have now been abandoned
- Good evidence supports duplex scanning for all patients with varicose veins prior to any intervention
- It provides both anatomical (B-mode) and haemodynamic (Doppler) information in real time
What it assesses:
- Presence of reflux in the deep and superficial venous systems
- Exact distribution and extent of reflux in the superficial system
- Presence of perforator incompetence
- Status of the deep veins (obstruction/DVT)
- Diameter of the GSV
Technique:
- High-frequency linear array transducer (7.5-13 MHz)
- Patient stands, leg externally rotated
- Scan commences in the groin - identifies the "Mickey Mouse" sign (GSV and CFV medial to common femoral artery in transverse view)
- The GSV within the "saphenous eye" (fascial compartment) is traced throughout
- Reflux = retrograde flow lasting >0.5 seconds (>1 second for proximal deep veins)
For venous ulcer assessment specifically:
"Most vascular surgeons will carry out a duplex scan when the patient with an ulcer is first seen to assess the status of the deep and superficial veins. The presence of reflux in these veins does not confirm a venous ulcer, but supports the diagnosis in the absence of another cause and helps direct treatment." - Bailey and Love, p. 1062
Additional investigations for the ulcer:
- ABPI (ankle-brachial pressure index) - mandatory to exclude arterial component (15-30% of venous ulcers have concomitant arterial disease)
- Full blood count, blood glucose, ESR/CRP, sickle cell test if appropriate
- Biopsy if malignancy suspected (Marjolin's ulcer)
iv. Principles of Management of Varicose Veins and Venous Ulcer
A. Management of Varicose Veins
1. Conservative (Non-interventional):
- Lifestyle modification: weight reduction, regular exercise, avoid prolonged standing
- Graduated compression hosiery
- Leg elevation
2. Endovenous (Minimally Invasive) - Now First-Line:
a) Endothermal Ablation:
- Endovenous Laser Ablation (EVLA): Laser fibre (1470 nm) inserted under ultrasound guidance; perivenous tumescent anaesthesia injected; laser thermally ablates the GSV by withdrawal of the fibre
- Radiofrequency Ablation (RFA): Catheter delivers controlled radiofrequency energy to cause collagen contraction and vein occlusion
b) Foam Sclerotherapy (Ultrasound-Guided):
- Tessari method: 1:3/1:4 mix of sclerosant (sodium tetradecyl sulfate) and air oscillated into foam
- Foam injected into GSV under ultrasound guidance
- Maximum 10-12 mL per session
- Less painful; useful for tortuous veins and in patients with skin changes overlying the ulcer area
c) Mechanochemical Ablation (MOCA):
- Combines mechanical endothelial disruption with liquid sclerosant injection
- No tumescent anaesthesia required
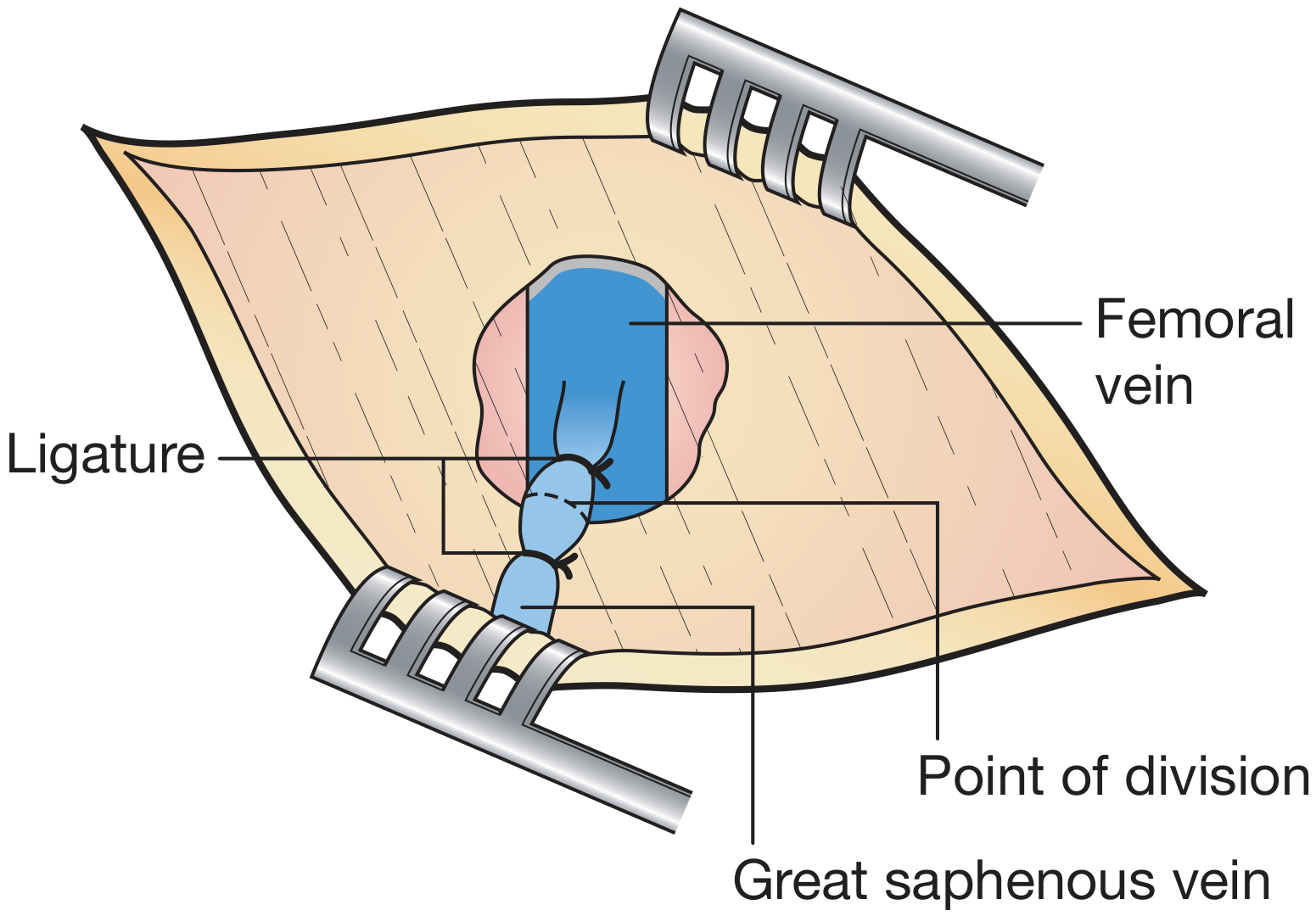
3. Surgical (Open) - When endovenous not feasible:
- Saphenofemoral junction (SFJ) ligation and GSV stripping
- Flush SFJ ligation; GSV stripped retrogradely to the knee
- All 6 SFJ tributaries ligated flush
- Avulsion phlebectomy of residual varicosities
B. Management of Venous Ulcer
Principle: Reduce ambulatory venous hypertension
1. Compression Therapy (Keystone of treatment):
- Four-layer bandaging (most effective):
- Orthopaedic wool (distributes pressure, absorbs exudate)
- Cotton crepe (smooths and holds wool)
- Elastic bandage (1/3 of interface pressure)
- Cohesive bandage (2/3 of interface pressure)
- Ideal interface pressure: 35-40 mmHg for pure venous ulceration
- Two-layer compression hosiery is equally cost-effective
- In mixed arterio-venous ulcer (ABPI 0.5-0.8): modified compression at 30 mmHg is safe
- ABPI <0.5 or ankle pressure <60 mmHg: revascularisation first, then compression
2. Superficial Venous Ablation (Accelerates healing + reduces recurrence):
- Treatment of superficial venous incompetence demonstrated to accelerate ulcer healing
- Expeditious referral to vascular service recommended
3. Wound Care:
- Cleansing with saline or water
- Appropriate dressings based on exudate level (non-adherent, moisture-retaining)
- Treat surrounding infection with antibiotics if cellulitis present
4. Adjunct Pharmacological Therapy:
- Pentoxifylline: Increases microvascular perfusion; useful adjunct to compression
- Horse chestnut seed extract: shown to improve venous symptoms and reduce leg volume
5. Skin Grafting (for recalcitrant ulcers):
- Pinch grafts or mesh grafting: 50% healed at 5 years
- Biological dressings (fetal keratinocytes, collagen meshes): improve healing but not cost-effective for most
6. Multidisciplinary Approach:
- Best results in specialist multidisciplinary ulcer services
- Specialist nursing teams in secondary or community care
v. Minimally Invasive Procedure for Varicose Veins
Endovenous Laser Ablation (EVLA) - or equally acceptable answers:
- Radiofrequency Ablation (RFA)
- Ultrasound-guided Foam Sclerotherapy (UGFS)
- Mechanochemical Ablation (MOCA)
All of these are performed under local/tumescent anaesthesia, with duplex ultrasound guidance, as day-case procedures without the need for general anaesthesia or surgical incision.
Summary Table
| Sub-question | Key Answer |
|---|---|
| (i) Diagnosis | Varicose veins (left GSV territory) + venous ulcer (medial gaiter area) due to chronic venous hypertension from prolonged standing |
| (ii) GSV Course | Dorsal venous arch → anterior to medial malleolus → medial leg with saphenous nerve → medial thigh → SFJ (2.5 cm below/lateral to pubic tubercle) into common femoral vein. 6 tributaries at SFJ (epigastric, circumflex iliac, external pudendal x2, AAGSV, posteromedial thigh vein) |
| (iii) Investigation | Duplex ultrasound (colour Doppler) - maps reflux, confirms incompetence, guides treatment |
| (iv) Management | Conservative: compression; Interventional: endovenous ablation/foam sclerotherapy/surgery; Ulcer: four-layer compression + wound care + venous ablation |
| (v) Minimally invasive procedure | Endovenous Laser Ablation (EVLA) / Radiofrequency Ablation / Foam Sclerotherapy |
This is a shared conversation. Sign in to Orris to start your own chat.