How to prescribe medicine in thyroid disease
Reading File
Finding Sources
Finding Sources
Searching PubMed
"thyroid disease" AND "treatment guidelines"
Finding Sources
Searching PubMed
"hypothyroidism" AND "levothyroxine"
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the information needed for a comprehensive answer. Let me compile it:
Prescribing Medicines in Thyroid Disease
A structured guide covering hypothyroidism, hyperthyroidism, and special situations, drawn from Goldman-Cecil Medicine (27th ed).
PART 1: HYPOTHYROIDISM
First-Line Drug: Levothyroxine (L-T4)
Levothyroxine is the standard replacement therapy for all forms of primary and secondary hypothyroidism.
Dosing:
- Young, healthy adults: Start at the full replacement dose - approximately 1.6 mcg/kg/day orally once daily
- Elderly patients or those with cardiac disease: Start LOW at 25-50 mcg/day, then increase by 12.5-25 mcg every 4-6 weeks
- Average maintenance dose: 75-150 mcg/day (varies by body weight, residual thyroid function, and etiology)
- Congenital hypothyroidism (neonates): 10-15 mcg/kg/day - prompt treatment is essential to prevent neurological damage
How to take:
- Take on an empty stomach, 30-60 minutes before breakfast
- Avoid concurrent calcium, iron supplements, antacids - they reduce absorption
Monitoring:
- Check TSH at 6 weeks after initiating or changing dose
- Target TSH: 0.5-2.5 mIU/L for most patients
- Elderly (>65 years): some guidelines accept TSH 1-4 mIU/L
- Once stable, monitor TSH annually
Subclinical Hypothyroidism (elevated TSH, normal T4)
Treat with levothyroxine if:
- TSH > 10 mIU/L
- TSH 4.5-10 mIU/L with symptoms, or pregnancy, or age < 65 years with cardiovascular risk factors
Pregnancy: TSH target < 2.5 mIU/L in first trimester; dose often needs to be increased 25-30% upon confirmed pregnancy.
When to Add T3 (Liothyronine)?
- Some patients remain symptomatic on T4 monotherapy
- A T4/T3 combination (e.g., adding liothyronine 5-10 mcg) may be considered in selected patients, though evidence is mixed
- Not routinely recommended as first-line
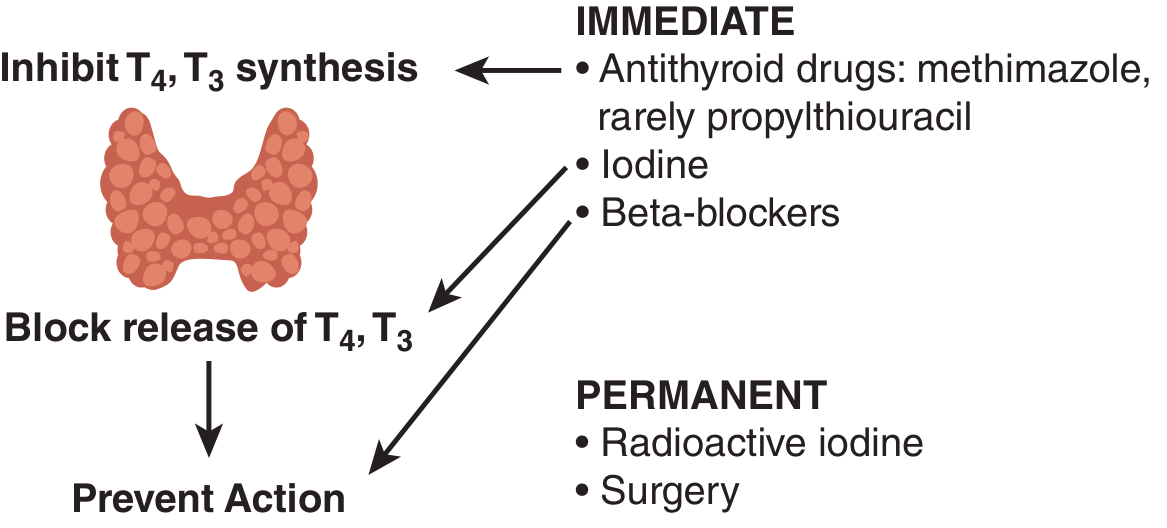
PART 2: HYPERTHYROIDISM
Overall Strategy
The treatment approach depends on the underlying cause:
| Treatment | Use Case | Outcome |
|---|---|---|
| Antithyroid drugs (methimazole, PTU) | Graves disease, first-line medical therapy | ~50% remission rate |
| Radioactive iodine (¹³¹I) | Definitive therapy for Graves, toxic MNG | 75-90% cure; ~80% risk of hypothyroidism at 1 year |
| Surgery (total thyroidectomy) | Definitive, large goiters, malignancy concern | Definitive cure; universal hypothyroidism follows |
A. Beta-Blockers (Symptom Control - Start First)
Use to control adrenergic symptoms (tremor, palpitations, tachycardia, atrial fibrillation rate):
- Propranolol (preferred): 20 mg every 6-8 hours, titrate up to maximum 240 mg/day in divided doses. Also inhibits type 1 deiodinase, reducing T3 by ~20%
- Atenolol 25-50 mg/day or Metoprolol 25-50 mg if patient has asthma/COPD (selective agents don't block deiodinase but control symptoms)
- Continue until thyroid hormone levels normalize
B. Antithyroid Drugs (Thionamides)
Mechanism: Block thyroid peroxidase, inhibiting thyroid hormone synthesis.
Methimazole (preferred)
- Initial dose (mild-moderate): 10-20 mg/day as a single oral dose
- Initial dose (severe/storm): 40-60 mg/day in divided doses
- Maintenance: 5-10 mg/day once biochemically controlled
- Duration: 12-18 months for a trial of remission in Graves disease
- Preferred over PTU except in first trimester of pregnancy and thyroid storm
Propylthiouracil (PTU)
- Initial dose: 100-150 mg every 8 hours (severe: up to 200 mg every 4-6 hours)
- Maintenance: 50-100 mg every 8-12 hours
- Advantages: Also blocks peripheral T4-to-T3 conversion - preferred in thyroid storm and first trimester pregnancy
- Disadvantage: Higher risk of hepatotoxicity (rare but serious) vs. methimazole
Monitoring Antithyroid Drugs:
- CBC before starting; recheck if fever or sore throat (agranulocytosis risk ~0.5%)
- Liver function tests - PTU can cause fulminant hepatic failure
- Check TFTs (free T4 + T3) every 4 weeks initially, then every 3-4 months
- Do not use TSH to monitor initially - it remains suppressed for months even after normalization of T4/T3
C. Radioactive Iodine (¹³¹I)
- Not a "prescription drug" per se but an outpatient treatment
- Contraindicated in pregnancy and breastfeeding
- May worsen Graves ophthalmopathy - consider steroid prophylaxis
- Results in hypothyroidism in up to 80% at 1 year - lifelong levothyroxine replacement follows
D. Iodine/Iodide
- Potassium iodide (SSKI) or Lugol's iodine - blocks thyroid hormone release acutely (Wolff-Chaikoff effect)
- Used for pre-operative preparation or in thyroid storm only - not for chronic management
PART 3: THYROID STORM (Thyrotoxic Crisis)
A medical emergency. Treat in ICU with all of the following simultaneously:
- PTU 200-300 mg every 4-6 hours (blocks synthesis AND T4-to-T3 conversion)
- Lugol's iodine 5-10 drops every 8 hours - start 1 hour AFTER PTU (to prevent using iodine as substrate for new hormone)
- Propranolol 60-80 mg every 4-6 hours orally, or IV esmolol if needed
- Hydrocortisone 100 mg IV every 8 hours (blocks T4-to-T3 conversion; treats relative adrenal insufficiency)
- Antipyretics (paracetamol - NOT aspirin, which displaces T4 from binding proteins)
- Treat the precipitant (infection, surgery, iodine load)
PART 4: SPECIAL POPULATIONS
| Population | Key Prescribing Points |
|---|---|
| Pregnancy | PTU in 1st trimester; switch to methimazole in 2nd/3rd trimester. Target maternal TSH lower than normal. Levothyroxine dose increases ~25-30% |
| Elderly | Start levothyroxine at very low dose (25 mcg); titrate slowly. Subclinical hypothyroidism may not need treatment if TSH < 10 |
| Cardiac disease | Start levothyroxine at 12.5-25 mcg; avoid over-replacement (risk of AF, angina). Beta-blockers essential in hyperthyroidism |
| Amiodarone-induced | Complex - may cause both hyper and hypothyroidism. Type 1 = excess synthesis (treat with thionamides); Type 2 = destructive thyroiditis (treat with glucocorticoids) |
| Neonates/children | Levothyroxine essential and urgent in congenital hypothyroidism; 10-15 mcg/kg/day |
PART 5: THYROID NODULE / CANCER
- Post-thyroidectomy for cancer: Levothyroxine at TSH-suppressive doses (target TSH 0.1-0.5 mIU/L for low-risk; < 0.1 mIU/L for high-risk differentiated cancer) to inhibit TSH-driven tumor growth
- Benign nodule: No routine suppressive levothyroxine unless there is symptomatic goiter
Summary: At-a-Glance Prescribing
| Condition | First Drug | Starting Dose | Target |
|---|---|---|---|
| Primary hypothyroidism | Levothyroxine | 1.6 mcg/kg/day (or 25-50 mcg in elderly) | TSH 0.5-2.5 |
| Graves hyperthyroidism | Methimazole + propranolol | Methimazole 10-20 mg/day; propranolol 20 mg q6-8h | Free T4/T3 normal |
| Thyroid storm | PTU + iodine + propranolol + hydrocortisone | See above | ICU management |
| Post-thyroidectomy (cancer) | Levothyroxine (suppressive) | Titrate to TSH 0.1-0.5 | TSH suppression |
- Goldman-Cecil Medicine (27th ed), Chapter 207 (Pearce EN & Hollenberg AN)
Recent literature note: A 2024 Lancet review on hypothyroidism (PMID 39368843) and a 2025 JAMA review (PMID 40900603) have reinforced the above guidelines. No major changes from standard practice, but the JAMA 2025 review highlights ongoing debate about T3 combination therapy and TSH targets in the elderly.
This is a shared conversation. Sign in to Orris to start your own chat.