HPV
Reading File
Asking for Preferences
Finding Sources
Searching PubMed
"human papillomavirus"[MeSH Terms] AND vaccination
Searching the Web
HPV human papillomavirus overview types pathogenesis vaccines 2025
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Now I have enough from the textbooks to give a thorough, well-organized answer. Let me compile it.
Human Papillomavirus (HPV): A Complete Overview
1. Virology
HPV belongs to the Papovaviridae family. It is a non-enveloped, icosahedral virus ~55 nm in diameter, with an 8 kb double-stranded DNA genome contained within a protein capsid. The virus infects only epidermal cells (skin or mucosa) and cannot survive outside a host.
Genome Organization
The ~8,000 base-pair genome encodes 8 main genes, split into:
| Category | Genes | Function |
|---|---|---|
| Early (E) | E1, E2 | Viral DNA replication, transcription regulation |
| E4 | Supports viral amplification and maturation | |
| E5 | Cell proliferation support | |
| E6 | Degrades p53 (tumor suppressor) - key oncogene | |
| E7 | Inactivates pRb (retinoblastoma protein) - key oncogene | |
| Late (L) | L1, L2 | Capsid proteins - targets for vaccines |
| LCR | - | Long control region: regulates replication |
2. HPV Types
More than 120 HPV genotypes have been identified, divided into:
- Mucosal (~40 types) vs. cutaneous types
- Low-risk types: HPV 6 and 11 - cause genital warts (condyloma acuminata) and laryngeal/recurrent respiratory papillomatosis
- High-risk (oncogenic) types: HPV 16 and 18 are the most important
- HPV 16 and 18 cause ~70% of cervical cancers
- HPV 16 drives ~96% of HPV-positive oropharyngeal cancers
- Other high-risk types: 31, 33, 45, 52, 58
3. Life Cycle & Pathogenesis
Entry
HPV infects basal epithelial stem cells through micro-abrasions in skin or mucosa. The virus binds heparan sulfate proteoglycans on cell surfaces, with α6 integrin proposed as a key receptor. Entry occurs via clathrin-mediated or caveolar endocytosis. The incubation period can last weeks, months, or even years.
Replication - Two Phases
-
Maintenance phase: Virus maintains 50-100 episomal copies per basal cell. E1 and E2 proteins sustain low-level replication. Crucially, this low copy number helps the virus evade immune detection.
-
Differentiation-dependent phase: As cells move into the suprabasal layer, E6 and E7 drive continued cell proliferation. Late promoter activation produces thousands of viral copies per cell. L1 and L2 capsid proteins are expressed and new virions are shed during normal epithelial cell shedding (not cell lysis - another immune evasion strategy).
Oncogenesis - The E6/E7 Mechanism
This is the central mechanism of HPV-related cancer:
- E7 binds and inactivates pRb (retinoblastoma protein), releasing E2F transcription factors and forcing the cell into uncontrolled S-phase (DNA replication)
- E6 binds and degrades p53, blocking the apoptotic response that would normally follow
- With both tumor suppressors disabled, cells accumulate mutations and chromosomal instability, leading to malignant transformation
- p16 overexpression is a surrogate marker: because E7 disrupts pRb, negative feedback on p16 is lost, causing p16 to accumulate - used diagnostically in pathology
In productive (non-transforming) infection, E2 suppresses E6/E7, allowing normal differentiation. In transforming (oncogenic) infection, the viral genome integrates into the host genome, disrupting E2 and unleashing E6/E7.
4. Clinical Manifestations
Benign Lesions
- Common warts (verruca vulgaris): HPV 2, 4 - skin
- Plantar warts: HPV 1, 2
- Flat warts: HPV 3, 10
- Genital warts / condyloma acuminata: HPV 6, 11 - soft, flesh-colored exophytic lesions of the genitals, perineum, anus
- Recurrent respiratory papillomatosis (RRP): HPV 6, 11 - laryngeal papillomas, can cause hoarseness and airway obstruction; perinatal transmission from mother to child
Premalignant/Malignant Lesions
- Cervical intraepithelial neoplasia (CIN) - graded I, II, III; CIN III = carcinoma in situ
- Cervical cancer: predominantly HPV 16, 18 - 99% of cases are HPV-positive
- Anal intraepithelial neoplasia (AIN) and anal squamous cell carcinoma
- Oropharyngeal squamous cell carcinoma (OPSCC): HPV 16 dominant; as of 2020, HPV-associated head and neck cancers in the US now exceed cervical cancer in incidence
- Penile, vulvar, and vaginal cancers: less common but HPV-associated
- Epidermodysplasia verruciformis (EV): rare, with HPV-5 and -8 causing SCCs on sun-exposed skin; acquired form (AEDV) seen in HIV patients
HPV in Immunocompromised Patients
HIV-positive individuals have:
- Higher HPV prevalence and reduced clearance
- 3x increased incidence of CIN and higher-grade lesions
-
90% anal HPV prevalence in MSM with HIV; up to 50% prevalence of high-grade AIN
- 30-50x higher anal cancer risk; 5x higher penile cancer risk compared to the general population
5. Screening
Cervical Cancer Screening (USPSTF Guidelines)
| Age | Recommendation |
|---|---|
| Under 21 | No screening |
| 21-29 | Pap smear (cytology) every 3 years |
| 30-65 | Pap + HPV co-testing every 5 years (preferred), or Pap alone every 3 years |
| Over 65 | Discontinue if adequate prior screening & low risk |
- HPV DNA testing alone as primary cervical screening is an evolving area; it is not universally adopted as a standalone primary screen in all settings
- Colposcopy with biopsy is indicated for abnormal Pap (e.g., ASC-US with positive HPV, LSIL, HSIL) - allows directed biopsies of acetowhite lesions
- During pregnancy: cytology, HPV testing, and physical exam are used; endocervical curettage is avoided
Anal Cancer Screening
- No universal guidelines from USPSTF
- International Anal Neoplasia Society consensus recommends screening in high-risk groups (HIV-positive, MSM, immunocompromised)
- Methods: anal cytology, high-resolution anoscopy (HRA)
Oropharyngeal Cancer
- No established screening guidelines as of now
- HPV vaccination expected to reduce incidence over time
6. Vaccines
Three HPV vaccines have been developed, all based on self-assembled Virus-Like Particles (VLPs) from the L1 major capsid protein - they are not live vaccines and cannot cause infection.
| Vaccine | Types Covered | Targets |
|---|---|---|
| Cervarix (bivalent) | 16, 18 | Cervical cancer |
| Gardasil 4 (quadrivalent) | 6, 11, 16, 18 | Cervical cancer + genital warts |
| Gardasil 9 (9-valent) | 6, 11, 16, 18, 31, 33, 45, 52, 58 | ~90% of cervical cancers + warts |
Vaccination Schedule (ACIP Recommendations)
- Routine: Age 11-12 years (can start at age 9); 2-dose series if started before age 15 (0 and 6-12 months)
- Catch-up: Through age 26 for all unvaccinated males and females; 3-dose series if starting at ≥15 years
- Ages 27-45: Shared clinical decision-making (not routine recommendation); benefit decreases with prior exposure
- Not licensed for adults over 45
Key principles:
- Vaccines are prophylactic only - they prevent new HPV infections but do NOT treat established infection or reverse HPV-related disease
- Protection lasts >10 years (ongoing studies suggest likely longer)
- Herd immunity effect: reduces HPV prevalence even in unvaccinated individuals
- Effective in HIV-positive patients, though antibody titers are somewhat lower (recommend 3-dose series in PLWH); vaccination recommended up to age 26 in PLWH
7. Treatment of HPV-Related Lesions
No therapy eliminates HPV from surrounding tissue. Recurrence is common due to reactivation of latent virus, autoinoculation, or reinfection. Goals: eliminate visible lesions, eradicate premalignant tissue, prevent transmission.
Genital Warts
| Therapy | Notes |
|---|---|
| Imiquimod 5% cream | Patient-applied, 3x/week up to 16 weeks; 56% clearance; 13% recurrence; activates Toll-like receptors (innate immunity) |
| Imiquimod 3.75% | Daily x 8 weeks; fewer side effects, slightly lower clearance |
| Podophyllotoxin 0.5% | Patient-applied; anti-mitotic |
| Cryotherapy | Provider-applied; destructive |
| Electrosurgery / laser | For larger or resistant lesions |
| Surgical excision | Definitive for large or recalcitrant lesions |
| Interferon-α intralesional | 1.0 x 10⁶ IU per lesion 3x/week x 3 weeks; immune stimulation; side effects include flu-like symptoms |
- Imiquimod and podophyllotoxin should NOT be used for vaginal, cervical, or anal lesions
- Safety in pregnancy not established for imiquimod
Cervical Disease
- CIN I: often observed (high spontaneous regression rate)
- CIN II/III: ablative or excisional therapy (LEEP - loop electrosurgical excision procedure, cold knife cone biopsy, cryotherapy)
- Invasive cervical cancer: surgery (hysterectomy), radiation, chemotherapy depending on stage
Sources: Harrison's Principles of Internal Medicine 22E; Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol. 1; Dermatology 2-Volume Set 5e; NCI HPV Vaccine Fact Sheet; Immune responses to HPV infection and vaccination - Frontiers in Immunology 2025
Give images also
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Finding Sources
Excellent - I now have a rich set of textbook images. Here is the complete illustrated overview:
Human Papillomavirus (HPV) - Illustrated Overview
1. Virology - Structure
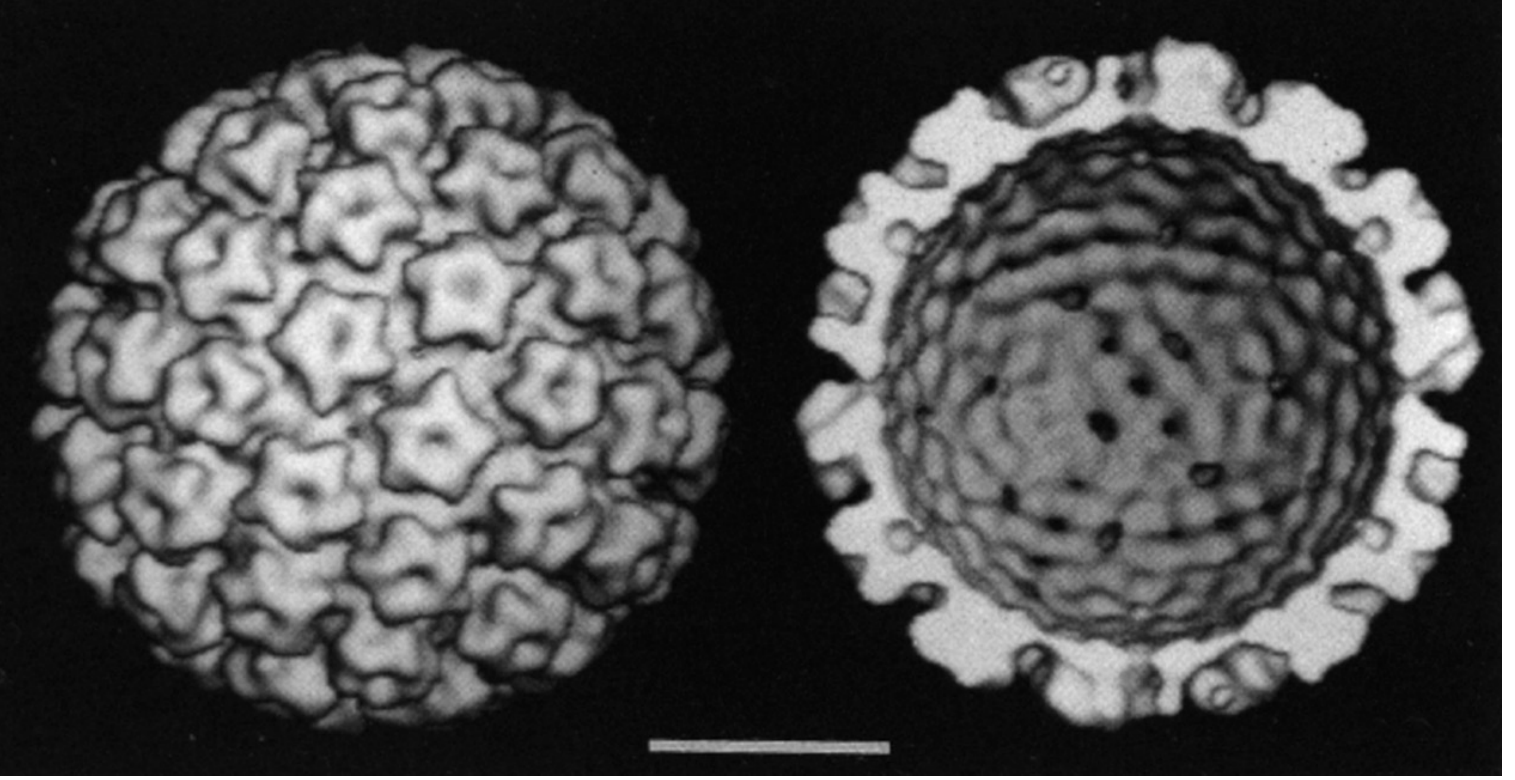
Fig. 1 - Computer reconstruction of cryoelectron micrographs of HPV. Left: Surface view showing 72 capsomeres in an icosahedral arrangement, each forming a 5-point star shape. Right: Cross-section showing capsomere interaction and internal channels. The virion is ~55 nm in diameter and non-enveloped.
(Medical Microbiology 9e)
2. Genome Organization
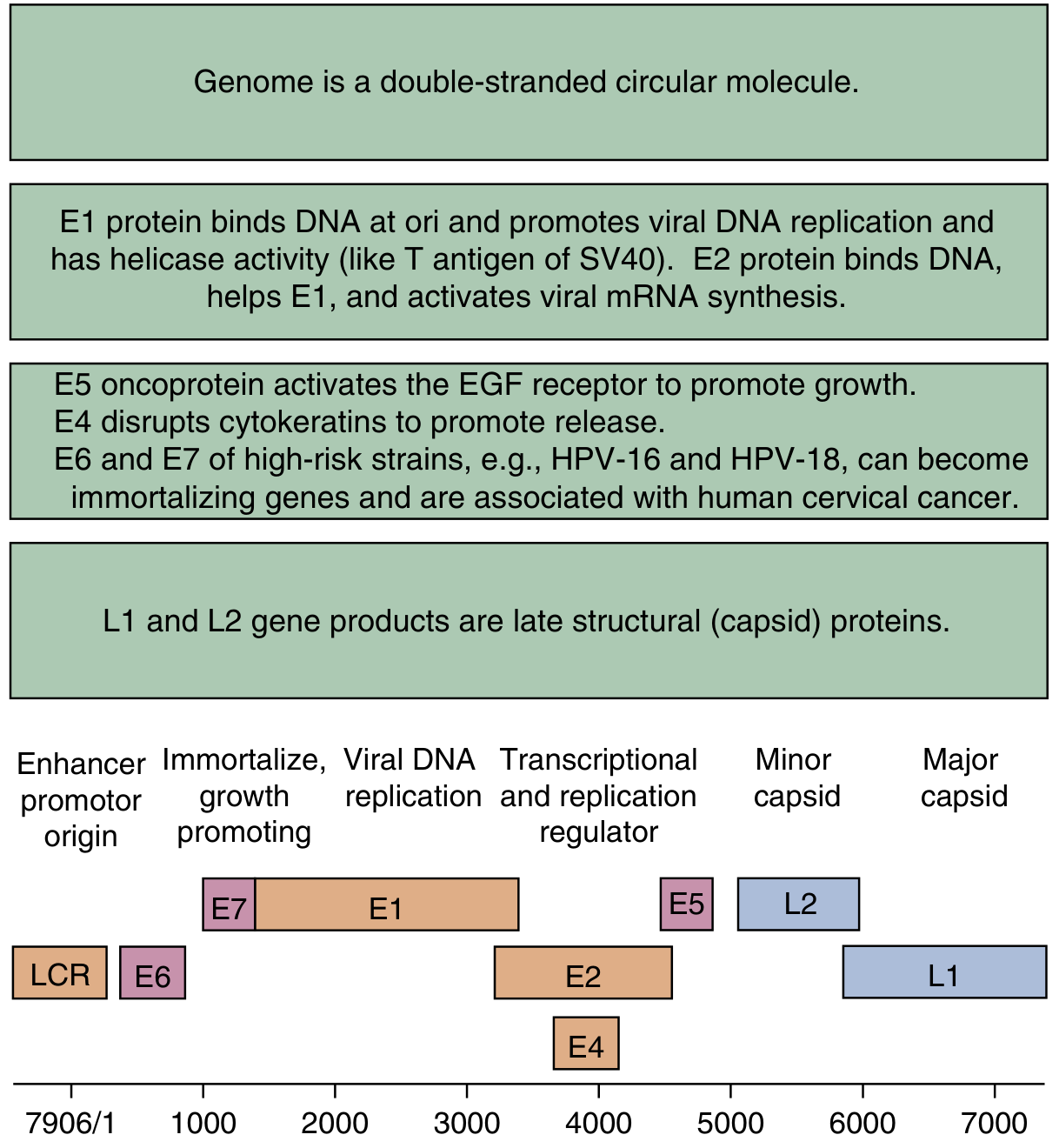
Fig. 2 - Genome of HPV-16 shown in linear form. The ~8,000 bp double-stranded circular DNA encodes:
- LCR - Long control region (enhancer/promoter/origin of replication)
- E6 - Binds and degrades p53; activates telomerase; suppresses apoptosis
- E7 - Binds and inactivates pRb (p105 retinoblastoma protein)
- E1 - Viral DNA replication (helicase activity)
- E2 - Transcriptional and replication regulator; suppresses E6/E7 in productive infection
- E4 - Disrupts cytokeratins; promotes virion release
- E5 - Activates EGF receptor; promotes cell growth
- L2 - Minor capsid protein
- L1 - Major capsid protein (target of all HPV vaccines) (Medical Microbiology 9e)
3. Life Cycle - Epithelial Layer Replication
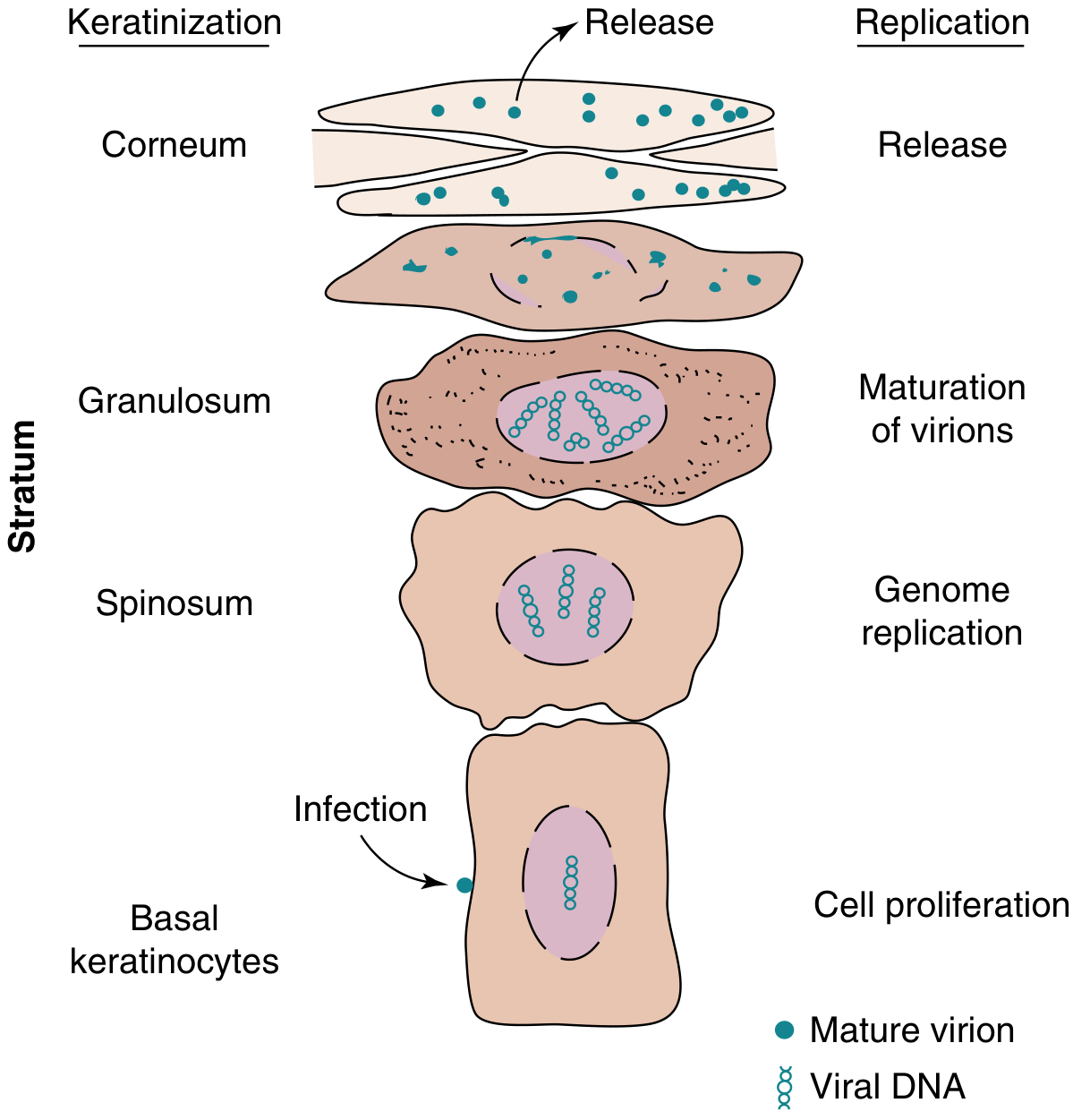
Fig. 3 - HPV replication through the epithelial layers:
- Basal keratinocytes: Initial infection; viral DNA enters nucleus; cell proliferation begins; only a few viral copies maintained (immune evasion)
- Stratum spinosum: Active genome replication as cells differentiate
- Stratum granulosum: Virion maturation - L1 and L2 capsid proteins assembled
- Stratum corneum: Release of thousands of mature virions during normal epithelial shedding (not cell lysis - another immune evasion mechanism) (Medical Microbiology 9e)
4. Oncogenesis - Koilocytes (Hallmark of HPV Infection)
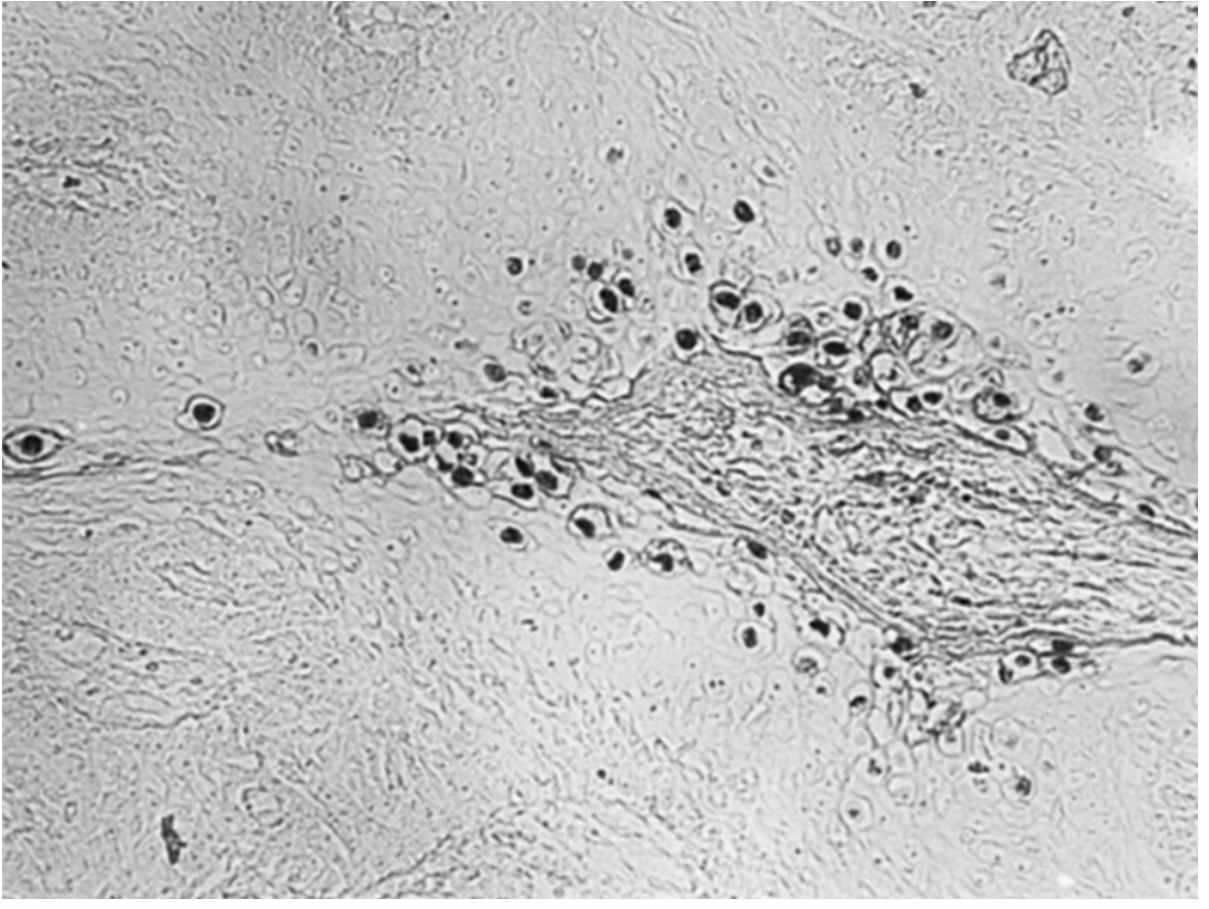
Fig. 4 - DNA probe analysis of HPV-6-induced anogenital condyloma. Dark staining (horseradish peroxidase-labeled probe) localizes over the nuclei of koilocytes - enlarged keratinocytes with perinuclear cytoplasmic halos (clearing) around shrunken, raisinoid nuclei. Koilocytosis is the pathognomonic histologic finding of active HPV infection.
(Medical Microbiology 9e)
5. Condyloma Acuminatum - Histology
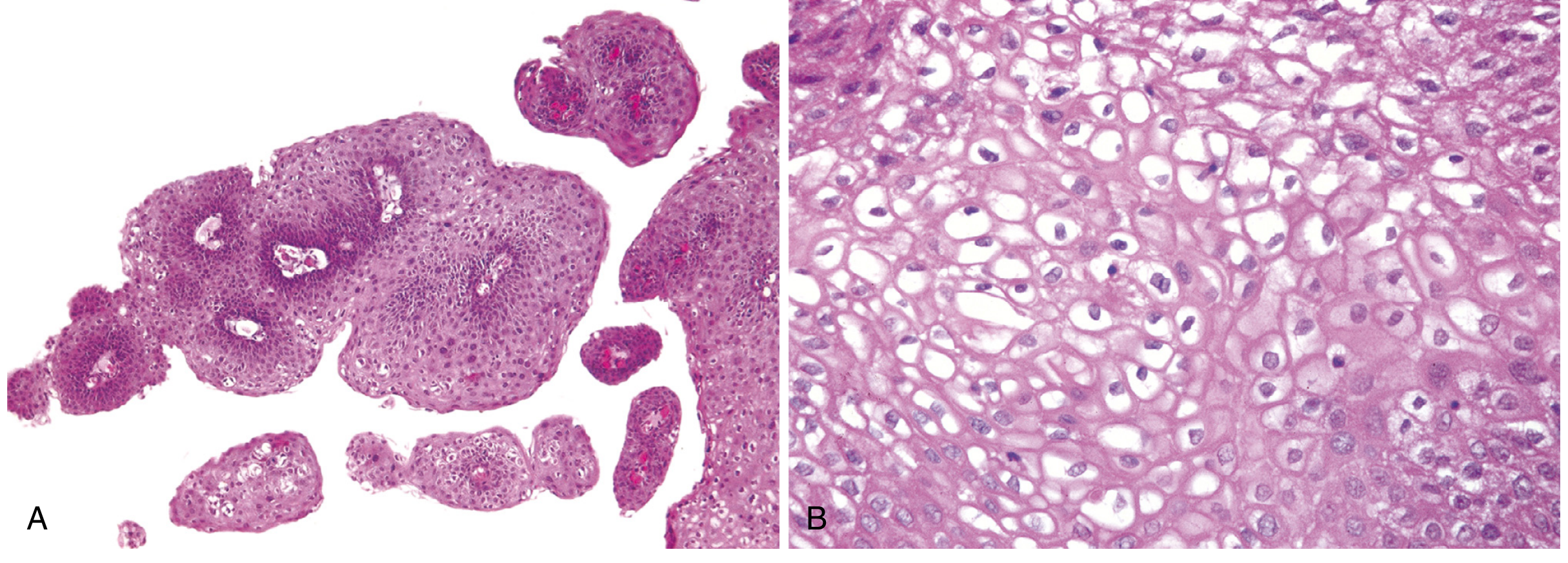
Fig. 5 - Condyloma acuminatum (genital wart) caused by HPV 6/11:
- (A) Low power: Branching villous/papillary architecture with acanthosis (epidermal thickening) and hyperkeratosis - the classic "cauliflower" appearance histologically
- (B) High power: Koilocytosis - perinuclear cytoplasmic vacuolization with shrunken nuclei; this is the defining feature of productive HPV infection in tissue sections (Robbins & Cotran Pathologic Basis of Disease)
6. Bowen Disease (HPV-Associated Carcinoma In Situ)
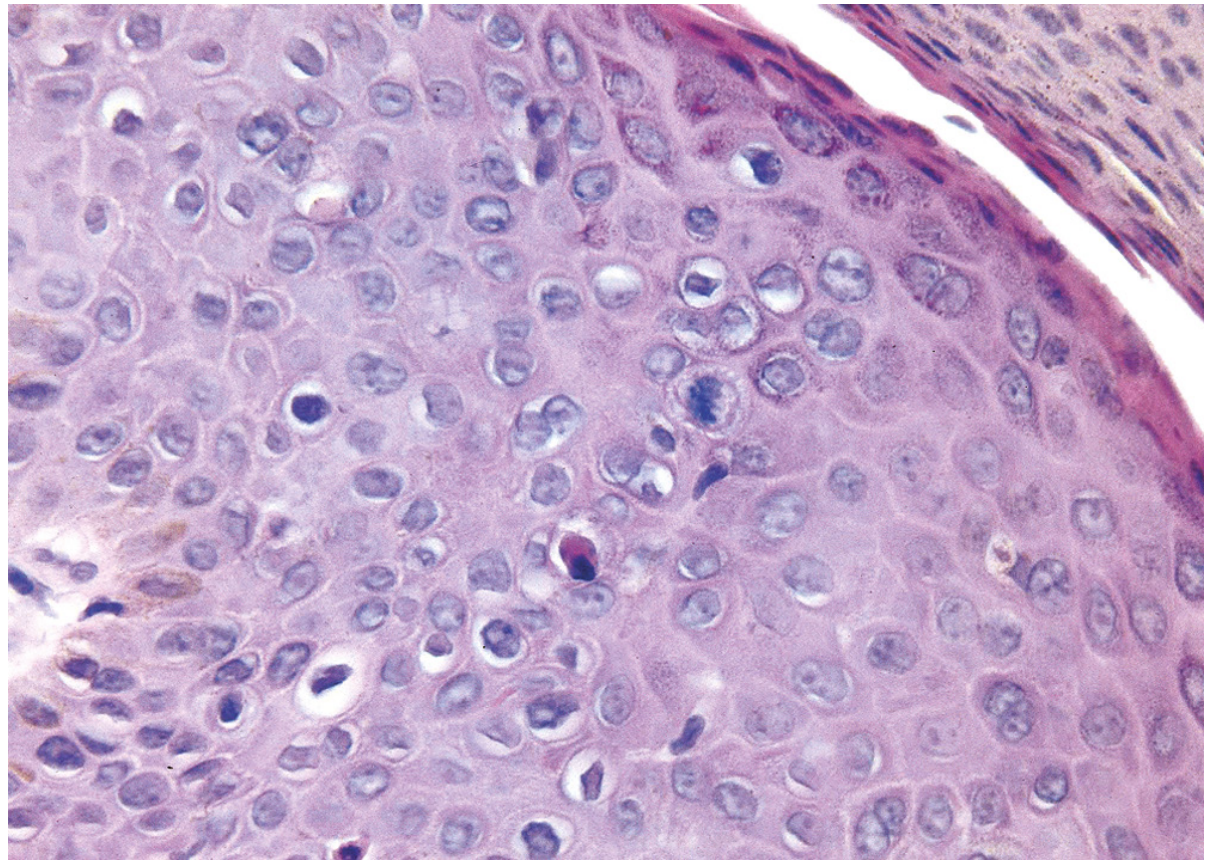
Fig. 6 - Bowen disease (carcinoma in situ / high-grade intraepithelial neoplasia) associated with high-risk HPV 16. Histology shows:
- Hyperchromatic, dysplastic, dyskeratotic epithelial cells throughout all layers
- Loss of orderly maturation (full-thickness dysplasia)
- Scattered mitoses above the basal layer (abnormal mitotic figures)
- Intact basement membrane (in situ - not yet invasive)
This is the morphologic equivalent of CIN III (cervical intraepithelial neoplasia grade 3) when it occurs at the cervix.
(Robbins & Cotran Pathologic Basis of Disease)
Summary: Key HPV Types at a Glance
| HPV Type | Risk | Disease |
|---|---|---|
| 1, 2, 4 | Low | Plantar/common skin warts |
| 6, 11 | Low | Genital warts, laryngeal papillomatosis |
| 16 | High | Cervical, oropharyngeal, anal, penile cancers |
| 18 | High | Cervical cancer (adenocarcinoma predominant) |
| 31, 33, 45, 52, 58 | High | Cervical and other cancers |
The E6/E7 Oncogenic Mechanism (Summary)
HPV integrates → E2 disrupted → E6/E7 unleashed
↓ ↓
E6 degrades p53 E7 inactivates pRb
↓ ↓
No apoptosis Uncontrolled S-phase entry
↓ ↓
DNA mutations ──→ Genomic instability ──→ CANCER
Sources: Medical Microbiology 9e; Robbins & Cotran Pathologic Basis of Disease; Harrison's Principles of Internal Medicine 22E; Scott-Brown's Otorhinolaryngology Head & Neck Surgery
This is a shared conversation. Sign in to Orris to start your own chat.