Explain clearly about heart sounds
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive material from Guyton & Hall, Ganong's, and Harrison's to write a thorough explanation. Here is a complete, well-structured overview of heart sounds:
Heart Sounds
Overview
Heart sounds are vibrations produced by valve closures, turbulent blood flow, and ventricular wall oscillations during the cardiac cycle. Normally, two sounds are heard with a stethoscope — S1 ("lub") and S2 ("dub") — but two additional sounds (S3 and S4) may occur in health or disease.
The Normal Cardiac Cycle and Sound Timing
| Phase | Event | Sound |
|---|---|---|
| Start of systole | AV valve closure | S1 |
| During systole | (normally silent) | — |
| End of systole | Semilunar valve closure | S2 |
| Early diastole (rapid filling) | Ventricular wall vibration | S3 (if present) |
| Late diastole (atrial contraction) | Atrial kick / ventricular filling | S4 (if present) |
S1 — First Heart Sound ("lub")
Cause: Closure of the mitral (bicuspid) and tricuspid valves at the onset of ventricular systole.
Mechanism: At the start of systole, ventricular contraction causes sudden backflow of blood against the AV valves, slamming them shut and bulging them toward the atria. The chordae tendineae abruptly arrest this bulge, and the elastic recoil bounces blood back into the ventricles. This sets the valves, blood, and ventricular walls into vibration — the sound is conducted through adjacent tissues to the chest wall.
Characteristics:
- Duration: ~0.14 seconds
- Frequency: 25–45 Hz (low-pitched, relatively prolonged — "lub")
- Best heard: Mitral area (cardiac apex, 5th intercostal space, midclavicular line) and tricuspid area (lower left sternal border)
- S1 contains both M1 (mitral) and T1 (tricuspid) components; normal splitting of S1 can occasionally be heard
Factors affecting S1 intensity:
| Louder S1 | Softer S1 |
|---|---|
| Short PR interval | Long PR interval |
| Hyperkinetic states (fever, thyrotoxicosis, pregnancy) | LV systolic dysfunction |
| Early rheumatic mitral stenosis | Late calcified mitral stenosis |
| Tachycardia | β-blocker use |
"S1 is classically loud in the early phases of rheumatic MS and in patients with hyperkinetic circulatory states or short PR intervals." — Harrison's Principles of Internal Medicine, 22nd Ed.
S2 — Second Heart Sound ("dub")
Cause: Closure of the aortic (A2) and pulmonic (P2) valves at the end of ventricular systole.
Mechanism: When ejection ends and ventricular pressure falls below arterial pressure, the semilunar valves snap shut. They bulge back toward the ventricles, setting up a short reverberation of blood between the valve cusps and arterial walls. These vibrations travel through the vessel walls to the chest.
Characteristics:
- Duration: ~0.11 seconds (shorter than S1 because semilunar valves are tauter)
- Frequency: ~50 Hz (higher-pitched than S1 — "dub")
- Best heard: Aortic area (2nd right intercostal space) and pulmonic area (2nd left intercostal space)
Splitting of S2
S2 has two audible components — A2 (aortic) and P2 (pulmonic). Normally A2 precedes P2.
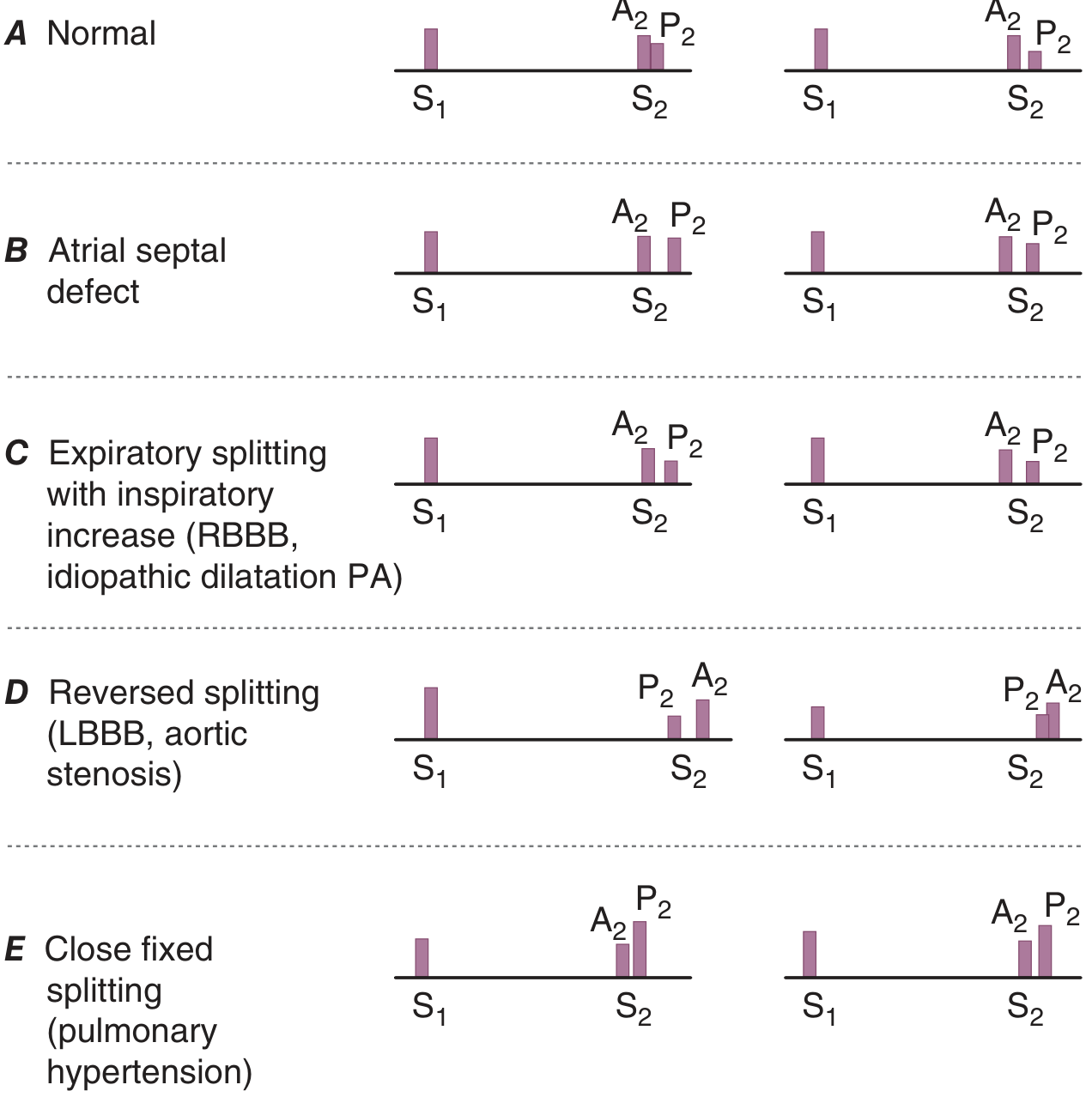
| Type of Splitting | A2–P2 Interval | Cause |
|---|---|---|
| Physiologic (normal) | Widens on inspiration, narrows on expiration | Increased venous return on inspiration delays P2 |
| Wide splitting | Always wide, increases on inspiration | RBBB, pulmonary stenosis, severe MR |
| Fixed splitting | Wide and does not change with respiration | Atrial septal defect (ASD) |
| Paradoxical (reversed) splitting | Widens on expiration, narrows on inspiration | LBBB, aortic stenosis, HOCM, RV pacing |
| Narrow/single S2 | Components fused | Pulmonary arterial hypertension, severe AS |
Note: P2 is considered loud when its intensity exceeds A2 at the base — a sign of pulmonary hypertension.
S3 — Third Heart Sound
Timing: Early diastole — during the rapid ventricular filling phase, approximately one-third of the way through diastole.
Cause: As blood rushes from the atria into the ventricles during passive filling, the ventricular walls suddenly decelerate the inflow, causing oscillation of blood back and forth — analogous to water rushing into a paper bag. This produces a low-frequency vibration.
Characteristics:
- Frequency: Very low (~20–40 Hz) — barely audible; recorded more easily on phonocardiogram
- Pitch: Low, dull ("lub-dub-ta")
- Best heard: With the bell of the stethoscope at the LV apex (left-sided S3) or lower left sternal border (right-sided S3, louder on inspiration)
Clinical significance:
| Context | Meaning |
|---|---|
| Children, adolescents, young adults | Normal ("physiologic S3") |
| Adults >40 years | Pathological — indicates systolic heart failure |
| Right-sided S3 | Right heart failure |
| Predictive value | Left-sided S3 in heart failure predicts ↑ cardiovascular morbidity and mortality |
"An S3 is equally prevalent among heart failure patients with preserved and reduced LV ejection fraction." — Harrison's, 22nd Ed.
S4 — Fourth Heart Sound
Timing: Late diastole — just before S1, during atrial contraction ("presystolic").
Cause: The atria contract forcefully to push blood into a stiff, non-compliant ventricle, causing ventricular wall vibration.
Characteristics:
- Frequency: Very low (~20 Hz or less) — rarely audible at bedside
- Creates a "ta-lub-dub" rhythm (gallop)
- Best heard: Cardiac apex (left-sided), lower left sternal border (right-sided)
Clinical significance:
| Condition | Mechanism |
|---|---|
| LV hypertrophy (hypertension, AS) | Stiff ventricle — needs strong atrial kick |
| Active myocardial ischemia | Reduced compliance |
| Hypertrophic cardiomyopathy | Stiff, hypertrophied myocardium |
| Absent in atrial fibrillation | No organized atrial contraction |
Auscultation Areas
Sound is transmitted from each valve along blood flow rather than directly through the chest wall, so the auscultation areas differ from the actual valve locations:
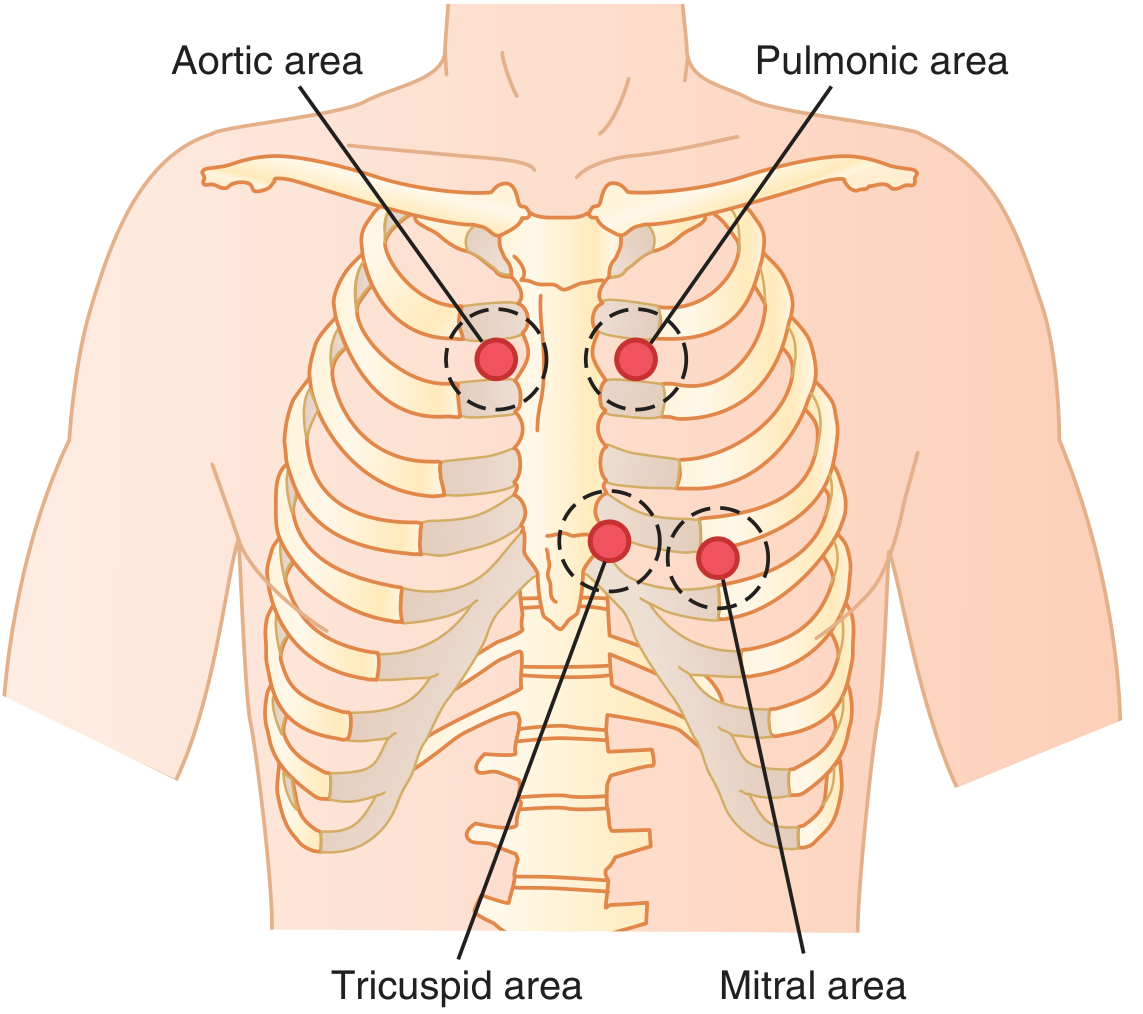
| Valve | Auscultation Area | Location |
|---|---|---|
| Aortic | 2nd right intercostal space, right sternal border | Sound conducted up the aorta |
| Pulmonic | 2nd left intercostal space, left sternal border | Sound conducted up the pulmonary artery |
| Tricuspid | Lower left sternal border (4th–5th ICS) | Over the right ventricle |
| Mitral | Cardiac apex — 5th ICS, midclavicular line | Over the left ventricle |
Additional Sounds
Ejection Sound (Ejection Click)
- Timing: High-pitched, early systolic sound coinciding with the upstroke of the carotid pulse
- Causes: Bicuspid aortic valve, bicuspid pulmonic valve, or dilation of the aortic/pulmonary root
- Key feature of pulmonic ejection sound: It is the only right-sided sound that decreases with inspiration (opposite of most right-sided sounds)
Opening Snap (OS)
- Timing: Early diastole, shortly after S2 (very short A2–OS interval)
- Cause: Sudden opening of a stenotic mitral valve
- Clinical significance: Classic for rheumatic mitral stenosis
- The shorter the A2–OS interval, the higher the left atrial pressure (more severe MS)
Pericardial Knock
- High-pitched diastolic sound, slightly later than OS
- Occurs in constrictive pericarditis due to abrupt cessation of ventricular expansion
Quick Mnemonics
| Sound | Mnemonic / Key Phrase |
|---|---|
| S1 | "Mitral Tricuspid" Mark The start of systole |
| S2 | "Aortic Pulmonic" — end of systole |
| S3 | "Kentucky" — S3 sounds like "lub-dub-ta" — heart failure in adults |
| S4 | "Tennessee" — "ta-lub-dub" — stiff, non-compliant ventricle |
Summary Table
| Sound | Timing | Cause | Heard with | Clinical Significance |
|---|---|---|---|---|
| S1 | Start of systole | Mitral + tricuspid valve closure | Diaphragm | Normal |
| S2 | End of systole | Aortic + pulmonic valve closure | Diaphragm | Normal; splitting patterns are key |
| S3 | Early diastole | Rapid ventricular filling vibration | Bell | Normal in young; HF in adults |
| S4 | Late diastole (pre-systole) | Atrial contraction into stiff ventricle | Bell | LV hypertrophy, ischemia; absent in AF |
| Ejection sound | Early systole | Bicuspid/stenotic valve opening | Diaphragm | Bicuspid aortic/pulmonic valve |
| Opening snap | Early diastole (after S2) | Mitral valve opening in stenosis | Diaphragm | Rheumatic mitral stenosis |
| Pericardial knock | Mid-diastole | Constrictive pericarditis | Diaphragm | Constrictive pericarditis |
Sources: Guyton and Hall Textbook of Medical Physiology; Ganong's Review of Medical Physiology, 26th Ed.; Harrison's Principles of Internal Medicine, 22nd Ed.
Explain mechanism
The previous conversation already covered the mechanisms of heart sounds in detail from the textbooks. Let me give you a focused, deeper explanation of the mechanism behind each heart sound.
Mechanism of Heart Sounds
Understanding What Generates Sound
Heart sounds are not caused by the valves slapping together — that is a common misconception. They are produced by:
- Sudden deceleration of blood when valves close or ventricular walls stop blood movement
- Vibration of taut valve leaflets and chordae tendineae under sudden tension
- Reverberation of blood bouncing between the valve and the adjacent cardiac/vascular walls
- These vibrations spread through adjacent tissues to the chest wall and are detected by the stethoscope
Mechanism of S1 (First Heart Sound)
Step-by-step sequence:
Ventricular systole begins
↓
Ventricular pressure rises above atrial pressure
↓
Blood surges BACK toward the atria → pushes AV valves shut
↓
Valve leaflets bulge toward the atria
↓
Chordae tendineae become taut → ABRUPTLY halt the bulging
↓
Elastic recoil of chordae + leaflets → blood bounces BACK into ventricle
↓
Blood, valve leaflets, and ventricular walls vibrate
↓
Vibrations travel through chest wall → heard as "LUB"
Key structural contributors:
- Mitral valve leaflets + chordae tendineae (dominant component — M1)
- Tricuspid valve leaflets + chordae tendineae (T1, slightly delayed)
- Ventricular myocardium and adjacent great vessel walls amplify the vibration
Why is S1 low-pitched and long?
The AV valves are relatively lax and large — the mitral has a large surface area with two leaflets, the tricuspid has three. Lax structures vibrate slowly → lower frequency (~25–45 Hz) and longer duration (~0.14 sec).
Mechanism of S2 (Second Heart Sound)
Step-by-step sequence:
End of ventricular ejection
↓
Ventricular pressure drops below aortic/pulmonary artery pressure
↓
Blood in the aorta/PA surges BACK toward the ventricle
↓
Semilunar valve cusps catch this backflow → valve snaps shut
↓
Cusps bulge BACK toward the ventricle
↓
Elastic recoil → blood bounces BACK into the aorta/PA
↓
Blood reverberates between arterial wall and semilunar valve
↓
Vibrations travel up the arterial walls → heard as "DUB"
Key structural contributors:
- Aortic valve cusps → A2 component (normally heard first)
- Pulmonic valve cusps → P2 component (slightly delayed, especially on inspiration)
- Arterial walls (aorta and pulmonary artery) act as the resonating chambers
Why is S2 higher-pitched and shorter than S1?
Two reasons:
- Semilunar valves are tauter than AV valves → vibrate at a higher frequency (~50 Hz)
- The aortic and pulmonary arterial walls are stiffer and more elastic than the ventricular chambers → higher elastic coefficient → faster, shorter vibration (~0.11 sec)
Mechanism of S2 Splitting — Why Inspiration Widens the Gap
This is one of the most commonly tested mechanisms in cardiology:
INSPIRATION
↓
Negative intrathoracic pressure
↓
↑ Venous return to RIGHT heart
↓
RV stroke volume ↑ → RV takes longer to eject → P2 delayed
↓
Simultaneously: ↑ lung vascular capacitance → ↓ pulmonary venous
return to LEFT heart → LV stroke volume ↓ → aortic valve closes EARLIER (A2 earlier)
↓
A2–P2 interval WIDENS → audible splitting on inspiration
On expiration, both effects reverse → A2 and P2 move closer together → single S2.
Abnormal Splitting Mechanisms:
| Type | Mechanism |
|---|---|
| Wide splitting (RBBB) | Electrical delay to RV → delayed RV contraction → P2 further delayed |
| Wide splitting (Pulmonary stenosis) | RV must work harder against obstruction → prolonged ejection → P2 very late |
| Fixed splitting (ASD) | Left-to-right shunt continuously volume-overloads the RV → P2 is always delayed regardless of respiration; respiratory changes in venous return are equalized across the ASD |
| Paradoxical splitting (LBBB) | Electrical delay to LV → delayed LV contraction → A2 occurs AFTER P2; on inspiration P2 moves later and approaches A2 → gap NARROWS (opposite of normal) |
| Narrow/single S2 (Pulmonary HTN) | ↑ PA pressure makes pulmonic valve snap shut rapidly → P2 becomes loud and early, merging with A2 |
Mechanism of S3 (Third Heart Sound)
Early diastole: Mitral valve opens
↓
Blood rushes rapidly from atrium into ventricle (passive filling phase)
↓
Ventricle rapidly distends and decelerates the inflowing blood
↓
Abrupt cessation of ventricular wall motion
↓
Blood oscillates back and forth between ventricular walls
(like water rushing into a paper bag — it reverberates)
↓
Low-frequency vibration of ventricular walls
↓
Heard as a soft, low-pitched "ta" after S2
Why does S3 only appear in the MIDDLE third of diastole?
In the very early diastole, the ventricle is not yet filled enough to have sufficient elastic tension for reverberation — the walls are too flaccid. Only once enough blood has entered does deceleration of the inflow produce enough tension to cause oscillation.
Why is it pathological in adults?
In a healthy young ventricle, the wall is compliant and absorbs the inflow smoothly. In heart failure or a volume-overloaded ventricle, the wall is stiffer or the atrial pressure is higher, producing more forceful rapid filling → louder, more prominent reverberation → audible S3 (gallop).
Mechanism of S4 (Fourth Heart Sound)
Late diastole: Atrial contraction (P wave on ECG)
↓
Atrium contracts forcefully
↓
Blood is pushed into a STIFF, non-compliant ventricle
↓
The ventricle resists sudden filling
↓
Sudden deceleration of atrial blood → vibrates the ventricular wall
↓
Very low-frequency sound just before S1 ("ta-lub-dub")
Why only in stiff ventricles?
In a normal, compliant ventricle, atrial contraction fills the ventricle gradually without a sudden halt — no reverberation occurs. When the ventricle is hypertrophied, ischemic, or fibrotic, it is stiff → the blood is suddenly decelerated → vibration occurs.
Why is S4 absent in atrial fibrillation?
S4 depends entirely on coordinated atrial contraction. In AF, there is no organized atrial systole — only chaotic electrical activity — so the atrial kick is absent and S4 cannot be generated.
Comparative Summary of Mechanisms
| Sound | Trigger | What Vibrates | Pitch | Duration |
|---|---|---|---|---|
| S1 | AV valve closure + chordae recoil | Valve leaflets, chordae, ventricular walls | Low | ~0.14 s |
| S2 | Semilunar valve closure + arterial recoil | Valve cusps, aorta/PA walls | Higher than S1 | ~0.11 s |
| S3 | Abrupt deceleration of rapid ventricular filling | Ventricular walls oscillating | Very low | ~0.10 s |
| S4 | Atrial contraction into stiff ventricle | Ventricular walls | Very low | Brief |
Sources: Guyton and Hall Textbook of Medical Physiology; Ganong's Review of Medical Physiology, 26th Ed.; Harrison's Principles of Internal Medicine, 22nd Ed.
A2 p2
A2 and P2 — The Two Components of S2
What Are A2 and P2?
The second heart sound (S2) is not a single event — it has two distinct components:
| Component | Full Name | Caused By |
|---|---|---|
| A2 | Aortic component | Closure of the aortic valve |
| P2 | Pulmonic component | Closure of the pulmonic valve |
Normally, A2 occurs before P2 because the left ventricle finishes ejection slightly before the right ventricle.
Why Does A2 Come Before P2?
Left ventricle has HIGHER pressure than right ventricle
↓
LV ejects blood FASTER and FINISHES ejection earlier
↓
Aortic valve closes FIRST → A2
↓
RV continues ejecting slightly longer (lower pressure system)
↓
Pulmonic valve closes SECOND → P2
↓
A2 precedes P2 by 20–30 ms (normally)
At normal heart rates, A2 and P2 are so close together that they sound like a single "dub." The gap becomes audible (splitting) mainly during inspiration.
Physiologic Splitting — Why Inspiration Widens A2–P2
This is the most important concept with S2:
INSPIRATION
│
├─► Negative intrathoracic pressure
│ ↓
│ ↑ Venous return to RIGHT heart
│ ↓
│ RV fills more → needs more time to eject → P2 DELAYED
│
└─► Increased pulmonary vascular capacitance
↓
↓ Pulmonary venous return to LEFT heart
↓
LV fills less → finishes ejection sooner → A2 EARLIER
↓
A2–P2 gap WIDENS → AUDIBLE SPLITTING on inspiration
EXPIRATION → Both effects reverse → A2 and P2 merge → single S2
Auscultation — Where to Hear Each Component
| Component | Best Heard At | Why |
|---|---|---|
| A2 | 2nd right intercostal space (aortic area) | Sound conducted up the aorta |
| P2 | 2nd left intercostal space (pulmonic area) | Sound conducted up the pulmonary artery |
| Both | Left sternal border | Useful for detecting splitting |
Normal rule:
A2 > P2 at the base — the aortic component is normally louder because the aortic pressure (~120 mmHg) is much higher than pulmonary pressure (~25 mmHg), producing a sharper valve snap.
A2 Intensity — What Affects It
| A2 Louder | A2 Softer |
|---|---|
| Systemic hypertension (↑ aortic diastolic pressure → valve snaps hard) | Aortic stenosis (calcified, immobile leaflets) |
| Hyperdynamic states (fever, thyrotoxicosis) | Aortic regurgitation (valve cannot close properly) |
| Thin chest wall | Obesity, emphysema, pericardial effusion |
P2 Intensity — What Affects It
| P2 Louder | P2 Softer |
|---|---|
| Pulmonary arterial hypertension (↑ PA pressure → forceful snap) | Pulmonary stenosis (thickened, stiff valve) |
| Large ASD with ↑ pulmonary flow | Low cardiac output states |
| Dilated pulmonary artery | — |
Clinical rule for P2:
P2 is considered abnormally loud when it:
- Is louder than A2 at the base (2nd ICS)
- Can be palpated as a tap at the 2nd left interspace
- Can be heard at the apex (normally P2 is not audible at the apex)
All three indicate pulmonary hypertension until proven otherwise.
Splitting Patterns — Complete Classification
1. Normal (Physiologic) Splitting
- A2 → P2 gap: widens on inspiration, disappears on expiration
- Heard in: Normal individuals, especially young people
- The gap is ~20–30 ms on expiration, widens to ~60 ms on inspiration
2. Wide Splitting (A2 ←—→ P2, always wide, increases on inspiration)
Both components are audible in both phases of respiration, but the gap still widens further on inspiration.
| Cause | Mechanism |
|---|---|
| Right bundle branch block (RBBB) | Electrical delay to RV → delayed RV contraction → P2 very late |
| Pulmonary stenosis | RV must overcome obstruction → prolonged ejection → P2 delayed |
| Severe mitral regurgitation | LV empties rapidly into low-pressure LA → aortic valve closes earlier → A2 very early |
| VSD | Volume overload of RV → prolonged RV ejection |
3. Fixed Splitting (A2 → P2 gap: wide and UNCHANGED with respiration)
The hallmark of Atrial Septal Defect (ASD):
ASD → left-to-right shunt → RV always volume overloaded
↓
P2 is always delayed (RV always has extra volume to eject)
↓
On INSPIRATION: venous return ↑ to RA, BUT the ASD allows equalization
of pressure → no extra augmentation of RV filling
↓
The A2–P2 gap remains FIXED regardless of respiration
Fixed splitting = ASD until proven otherwise.
4. Paradoxical (Reversed) Splitting (P2 → A2, gap widens on EXPIRATION)
Normal order is reversed — P2 comes BEFORE A2:
LBBB (or other causes of delayed LV activation)
↓
LV contracts LATE → aortic valve closes LATE → A2 delayed
↓
Now P2 occurs BEFORE A2 (order reversed)
↓
On INSPIRATION: P2 moves later (normal mechanism) →
P2 moves TOWARD A2 → gap NARROWS
On EXPIRATION: P2 moves earlier → P2 moves AWAY from A2 → gap WIDENS
↓
Splitting heard on EXPIRATION (opposite of normal)
| Cause | Mechanism |
|---|---|
| Left bundle branch block (LBBB) | Delayed LV activation → delayed A2 |
| Severe aortic stenosis | Prolonged LV ejection → delayed A2 |
| HOCM | Dynamic LV outflow obstruction → delayed A2 |
| RV pacing | Electrical activation of LV is secondary and delayed |
| Acute myocardial ischemia | LV dysfunction → slower ejection → delayed A2 |
5. Narrow / Single S2 (A2 and P2 fused)
| Cause | Mechanism |
|---|---|
| Pulmonary arterial hypertension | ↑ PA pressure → pulmonic valve snaps shut quickly and loudly, P2 moves earlier, merging with A2 |
| Severe aortic stenosis | A2 becomes very soft (calcified valve) — effectively inaudible, only P2 heard |
| Severe pulmonary stenosis | P2 very soft and so late it is inaudible |
Summary Comparison Table
| Pattern | Expiration | Inspiration | Classic Cause |
|---|---|---|---|
| Normal | Single S2 | Split (A2–P2) | Healthy individual |
| Wide splitting | Split | Wider split | RBBB, pulmonary stenosis |
| Fixed splitting | Split (wide) | Split (same width) | ASD |
| Paradoxical | Split (P2–A2) | Single or narrower | LBBB, severe AS |
| Single/narrow | Single | Single | Pulmonary HTN, severe AS |
Sources: Harrison's Principles of Internal Medicine, 22nd Ed.; Guyton and Hall Textbook of Medical Physiology; Ganong's Review of Medical Physiology, 26th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.