Explain about trachea in detail as per anatomy syllabus of BAMS
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Reading File
I now have comprehensive information from multiple authoritative sources. Let me compile a detailed, well-structured answer:
Trachea - Detailed Anatomy (BAMS Syllabus)
1. Introduction and Definition
The trachea (windpipe) is a midline, cartilaginous, fibromuscular tube that forms part of the lower respiratory tract (conducting portion). It serves as a conduit for air between the larynx above and the bronchi below, and also helps condition (warm, humidify, and clean) inspired air.
2. Extent and Vertebral Levels
| Point | Structure | Vertebral Level |
|---|---|---|
| Upper end | Begins at lower border of cricoid cartilage (continuous with larynx) | C VI |
| Lower end | Terminates at the carina (bifurcation into right and left main bronchi) | T IV/V (sternal angle level) |
- Begins at the lower border of the cricoid cartilage at vertebral level C VI
- Ends at the carina at the level of the sternal angle (angle of Louis), corresponding to vertebral level T IV/V
3. Measurements (Dimensions)
| Parameter | Value |
|---|---|
| Length (adults) | 10-12 cm (average ~11.8 cm in males, range 10-13 cm) |
| External diameter (AP) | 2.3 cm in males; 2.0 cm in females |
| External diameter (transverse) | 1.8 cm in males; 1.4 cm in females |
| Paediatric diameter | 3 mm at birth |
| Number of cartilaginous rings | 16-20 (approximately 18-22 rings; ~2 rings per cm) |
| Wall thickness | Approximately 3 mm |
The trachea has an ovoid/D-shaped cross section - it is not perfectly circular because the posterior wall is flat (membranous wall).
4. Course and Direction
The trachea:
- Begins anteriorly in the neck and slopes posteriorly as it enters the mediastinum
- Lies in the midline, directly anterior to the esophagus
- Shows significant vertical mobility - moves upward during swallowing, and downward/forward on inspiration
- Passes through the superior thoracic aperture (thoracic inlet) to enter the superior mediastinum
5. Relations
Anterior Relations:
In the neck:
- Skin, superficial and deep cervical fascia
- Sternohyoid and sternothyroid muscles
- Thyroid isthmus (overlies 2nd to 4th tracheal cartilages - variable)
- Inferior thyroid veins
In the thorax (superior mediastinum):
- Left brachiocephalic vein
- Brachiocephalic (innominate) artery
- Arch of the aorta (crosses on the left)
- Left common carotid artery
- Deep part of the cardiac plexus
- Pretracheal lymph nodes
- Thymus gland (large and fleshy in infants)
Posterior Relations:
- Esophagus (directly posterior, lying anterior to the vertebral column)
- Postero-laterally: Recurrent laryngeal nerves run in the tracheo-esophageal groove
Lateral Relations:
- Lobes of the thyroid gland
- Carotid sheath and its contents (common carotid artery, internal jugular vein, vagus nerve)
- Paratracheal lymph nodes
- Azygos vein crosses on the right side in the superior mediastinum
- Arch of the aorta on the left side in the superior mediastinum
6. Structure of the Tracheal Wall
The wall of the trachea consists of four layers (from inner to outer):
a) Mucosa
- Epithelium: Pseudostratified ciliated columnar epithelium (respiratory epithelium) with numerous goblet cells
- Rests on a broad basement membrane
- The cilia beat the mucus blanket upwards toward the larynx (mucociliary escalator)
- Lamina propria: Rich in longitudinal elastin fibres; contains numerous seromucous glands producing watery mucus
b) Submucosa
- Slightly denser connective tissue than the lamina propria
- Contains neurovascular structures, tubular glands, and lymphoid patches
- Contains additional seromucous glands
c) Cartilaginous Layer (Hyaline Cartilage Rings)
- 16-20 C-shaped (horseshoe-shaped) rings of hyaline cartilage
- Open ends face posteriorly (toward the esophagus)
- Function: Keep the tracheal lumen patent (prevent collapse, especially during expiration)
- The gap between the free ends is bridged by:
- Trachealis muscle (smooth muscle with transverse and longitudinal fibres)
- Fibroelastic tissue (fibroelastic membrane)
- The first tracheal ring is broader and may be joined to the cricoid cartilage by the cricotracheal ligament
- The last ring (before carina) is thick and broad, forming a bridge between the two main bronchi
- With aging, cartilages may calcify or even ossify (develop bone tissue and marrow spaces)
d) Adventitia
- Outermost layer of loose connective tissue
- Blends with the fascia over the esophagus and loose areolar tissue of the mediastinum
- Binds the trachea to adjacent structures
7. Trachealis Muscle
- Smooth muscle located at the posterior (membranous) wall of the trachea
- Has transverse fibres (insert into the perichondrium at free margins of cartilage rings) and longitudinal fibres
- Function:
- Relaxes during swallowing - allows the esophagus to bulge slightly into the tracheal lumen to accommodate a food bolus
- Contracts strongly during coughing - narrows the tracheal lumen, increasing velocity of expelled air to dislodge foreign material
8. Bifurcation - The Carina
- The trachea bifurcates at the carina into the right and left main (primary) bronchi
- Level: T IV/V posteriorly (sternal angle/manubriosternal joint anteriorly)
- The carina is a spur/ridge of cartilage seen on bronchoscopy at the bifurcation
- The last tracheal ring has a downward-curving triangular process forming the posterior carina
| Main Bronchus | Angle at Carina | Length | Width | Clinical Note |
|---|---|---|---|---|
| Right | 25-30° (more vertical) | ~2.5 cm | Wider | Foreign bodies more commonly lodge here |
| Left | ~45° (more horizontal) | ~5 cm | Narrower | Crosses under arch of aorta |
9. Blood Supply
Arterial supply (segmental, enters the lateral walls):
| Region | Artery |
|---|---|
| Cervical trachea | Inferior thyroid artery (via tracheoesophageal branches - usually 3 branches supply the upper half) |
| Thoracic trachea | Bronchial arteries; supreme intercostal arteries |
| Carina and bronchial tree | Bronchial arteries (2 on left from aorta directly; 1 on right from 3rd right posterior intercostal artery) |
- Blood supply enters posterolaterally (segmental fashion)
- Branches form a lateral longitudinal anastomosis along tracheal walls
- Anterior branches further anastomose near the midline
- Clinical point: Circumferential dissection around the trachea should be minimized to avoid devascularization
Venous drainage: Inferior thyroid plexus (venous)
10. Nerve Supply
| Component | Source | Effect |
|---|---|---|
| Motor (smooth muscle) | Recurrent laryngeal nerve (branch of vagus X) | Motor to trachealis |
| Parasympathetic (efferent) | Vagus nerve (CN X) | Bronchoconstriction, glandular secretion, vasodilation |
| Sympathetic | Middle cervical ganglion (interconnects with recurrent laryngeal nerves) | Bronchodilation |
| Sensory (afferent) | Recurrent laryngeal nerve (vagal afferents) | Cough reflex, sensation from mucosa |
11. Lymphatic Drainage
- Lymphatics arise in a submucosal plexus and connect with a plexus in the outer fibrous membrane
- Pretracheal nodes → Paratracheal nodes (level VI) → Superior tracheobronchial nodes
- Para-tracheal nodes drain into vessels from the internal thoracic and brachiocephalic lymph nodes
- These form the bronchomediastinal trunks, which drain into:
- Right lymphatic duct (right side)
- Thoracic duct (left side)
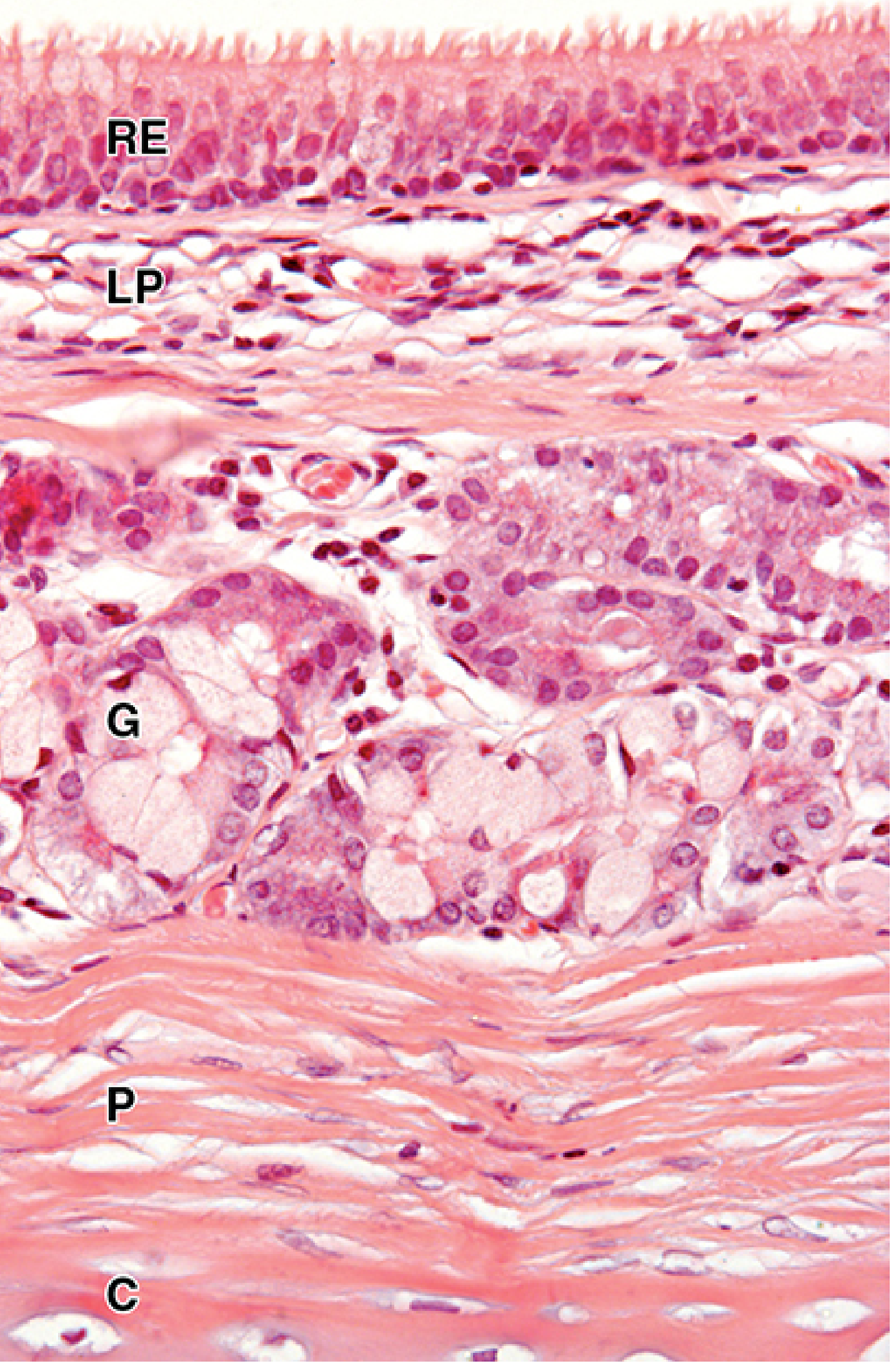
12. Histological Images
Tracheal wall histology (H&E stain) - RE = respiratory epithelium, LP = lamina propria, G = seromucous glands, P = perichondrium, C = hyaline cartilage:
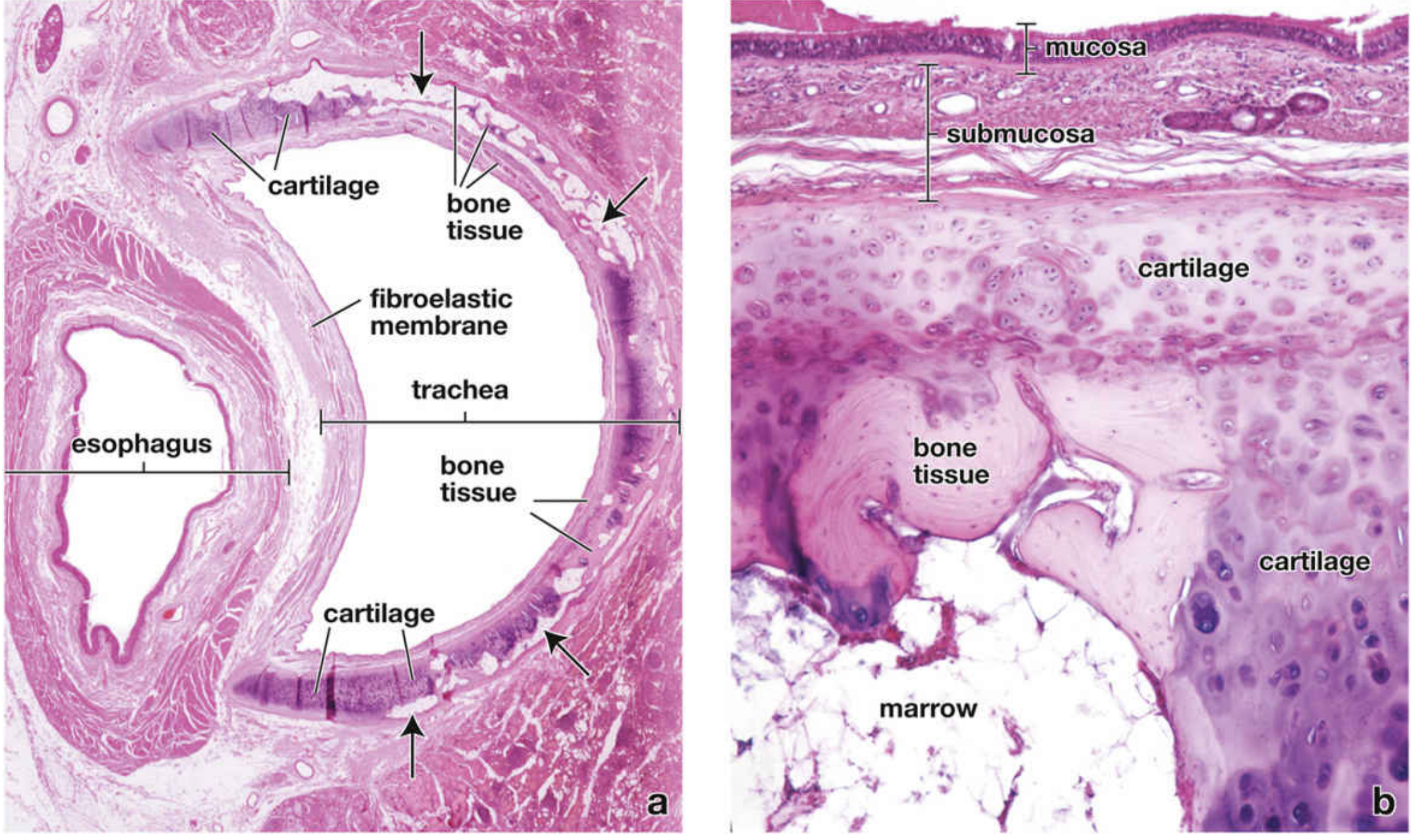
Trachea and esophagus cross-section showing C-shaped cartilage rings and fibroelastic membrane:
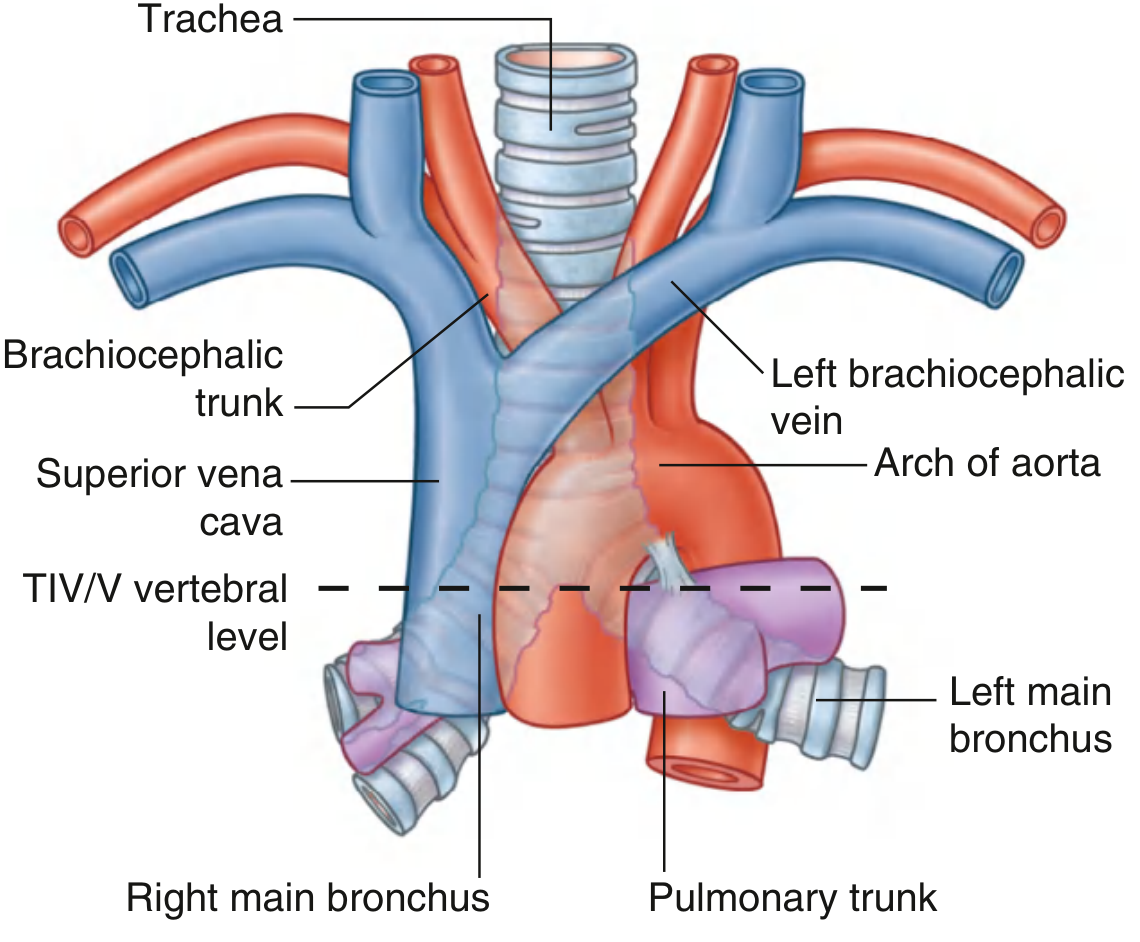
Trachea in the superior mediastinum, showing its bifurcation and vascular relations:
13. Applied Anatomy / Clinical Significance
-
Tracheotomy / Tracheostomy: Surgical opening of the trachea is performed through rings 2-4, below the thyroid isthmus. The inferior thyroid veins and thyroid isthmus must be carefully handled. In infants, the brachiocephalic vein may be higher and at risk.
-
Foreign body aspiration: More commonly enters the right main bronchus due to its more vertical angle, wider lumen, and it being more directly in line with the trachea.
-
Goitre (enlarged thyroid): Can deviate or compress the trachea, causing stridor and dyspnoea.
-
Bronchoscopy: Allows visualization of the tracheal lumen, carina, and main bronchi. The carina appears as a sharp ridge at the bifurcation.
-
Endotracheal intubation: Knowledge of tracheal dimensions and vertebral levels is essential to avoid inadvertent right main bronchus intubation.
-
Recurrent laryngeal nerve injury: During thyroid surgery or tracheal dissection, the RLN running in the tracheoesophageal groove is at risk, potentially causing hoarseness.
-
Cough reflex: Stimulation of tracheal mucosa triggers the cough reflex via vagal afferents, with the trachealis contracting to rapidly narrow the lumen and increase expiratory airflow velocity.
Sources:
- Gray's Anatomy for Students (neck and thorax sections)
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery (tracheal anatomy chapter)
- Junqueira's Basic Histology, 17e (tracheal histology)
- Histology: A Text and Atlas with Correlated Cell and Molecular Biology (tracheal microanatomy)
This is a shared conversation. Sign in to Orris to start your own chat.