pharangitis
Reading File
Finding Sources
Searching PubMed
pharyngitis diagnosis treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information to provide a thorough answer on pharyngitis.
Pharyngitis
Pharyngitis is inflammation of the pharynx and/or tonsils. It is one of the most common reasons for primary care visits, accounting for more than 7 million pediatric office visits annually in the United States alone.
Clinical Image
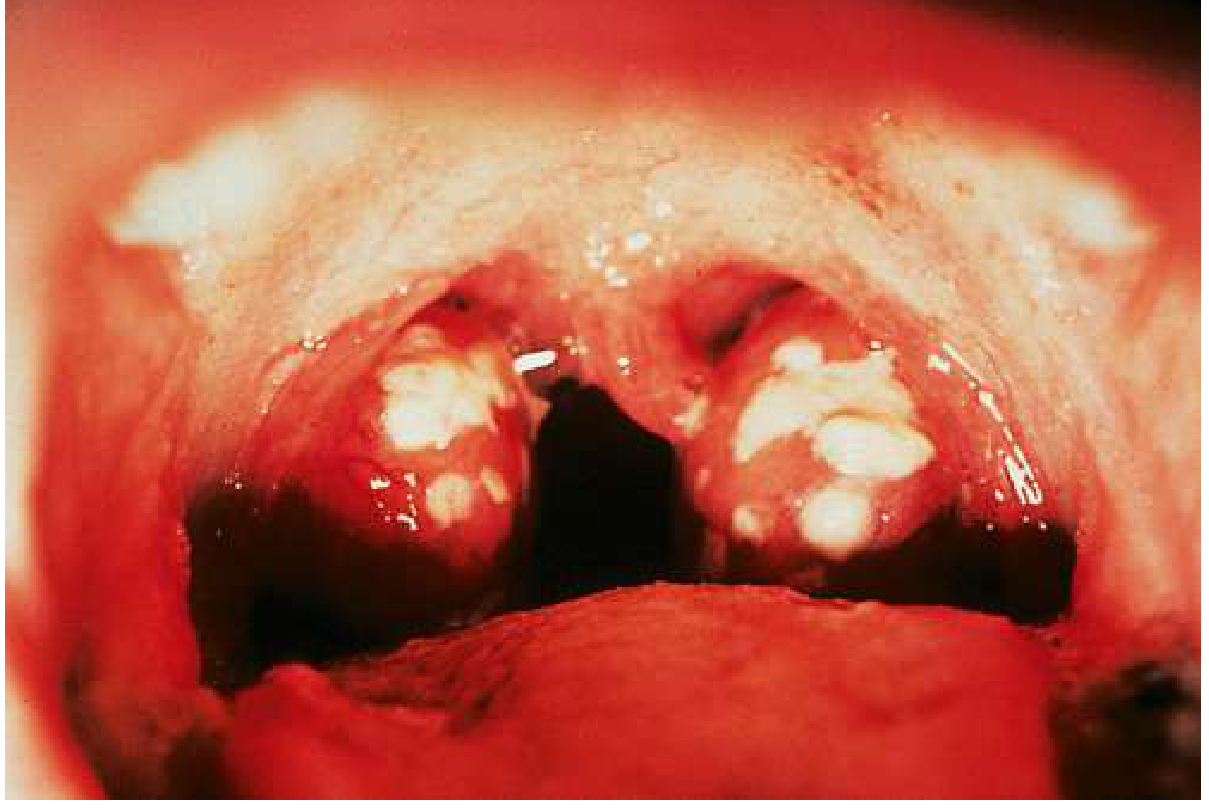
Bilateral tonsillar exudates with pharyngeal erythema - classic appearance of streptococcal pharyngitis
Etiology
Viral (most common) - 50-80% of cases:
| Virus | Notes |
|---|---|
| Adenovirus | Very common |
| Epstein-Barr virus (EBV) | Infectious mononucleosis |
| Rhinovirus | Common cold |
| Enterovirus (Coxsackievirus) | Hand-foot-mouth, herpangina |
| Influenza A & B | Seasonal |
| Parainfluenza | |
| HIV (acute retroviral syndrome) | 50-70% present with pharyngitis |
| CMV | Mimics EBV mono |
| RSV, Measles, Coronavirus |
Bacterial:
- Group A beta-hemolytic Streptococcus (GABHS / S. pyogenes) - the most important bacterial cause; 20-40% of pediatric cases, 5-15% of adult cases
- Group C and G streptococci
- Fusobacterium necrophorum (Lemierre's syndrome precursor)
- Neisseria gonorrhoeae (sexually transmitted)
- Mycoplasma pneumoniae
- Diphtheria (rare in vaccinated populations)
- Haemophilus influenzae type b (uvulitis, unimmunized patients)
Symptoms
- Sore throat, odynophagia
- Fever, chills
- Submandibular or anterior cervical lymphadenopathy
- Headache
- Abdominal pain, nausea/vomiting (especially in children)
- Absence of cough in bacterial pharyngitis (cough and hoarseness favor viral etiology)
Physical exam findings: tonsillopharyngeal erythema, tonsillar hypertrophy, exudates (does NOT reliably distinguish viral from bacterial), soft palate petechiae, edematous uvula.
Diagnosis - The Modified Centor Score
This scoring system helps decide who to test and treat for GABHS:
| Criterion | Points |
|---|---|
| Tonsillar exudates | +1 |
| Tender anterior cervical lymphadenopathy | +1 |
| Absence of cough | +1 |
| Fever (history of or >38°C) | +1 |
| Age 3-14 years | +1 |
| Age 15-44 years | 0 |
| Age ≥45 years | -1 |
- Score 0-1: GABHS unlikely - no testing or antibiotics
- Score 2+: Test with rapid antigen detection test (RADT) and/or culture
- Overt viral features (cough, rhinorrhea, oral ulcers, conjunctivitis): skip testing entirely
Testing approach:
- Rapid antigen detection test (RADT): sensitivity 80-90%, highly specific
- Rapid nucleic acid testing: sensitivity 97.5%, specificity 95% - preferred over RADT
- Throat culture: gold standard, sensitivity 90-95%, but requires 18-48 hours
- In children/adolescents: if RADT is negative, send backup culture
- In adults: backup culture usually not needed (low GABHS incidence + low rheumatic fever risk)
Treatment
Viral pharyngitis:
- Supportive care: analgesics (NSAIDs, acetaminophen), lozenges, salt-water gargles
- 85% of patients resolve spontaneously within 1 week
- EBV: avoid contact sports until splenomegaly resolves; avoid ampicillin/amoxicillin (causes maculopapular rash)
- A single dose of corticosteroid can be considered for severe tonsillar enlargement threatening the airway
GABHS pharyngitis - antibiotic therapy:
| Medication | Dose | Route | Duration |
|---|---|---|---|
| Penicillin V (first line) | Adult: 500 mg twice daily; Child: 250 mg twice daily | PO | 10 days |
| Amoxicillin (first line) | 50 mg/kg once daily (max 1000 mg) | PO | 10 days |
| Benzathine penicillin G | <27 kg: 600,000 units; ≥27 kg: 1.2 million units | IM | Single dose |
| Cephalexin (penicillin allergy w/o anaphylaxis) | 500 mg twice daily | PO | 5-10 days |
| Clindamycin (penicillin allergy) | 300 mg three times daily | PO | 10 days |
| Azithromycin (penicillin allergy) | 500 mg day 1, then 250 mg days 2-5 | PO | 5 days |
| Clarithromycin | 250 mg twice daily | PO | 10 days |
Key treatment notes:
- GABHS remains 100% susceptible to penicillin (no resistance documented)
- Clindamycin resistance in the US is up to 15%; macrolide resistance is also rising
- Antibiotics reduce the duration of symptoms modestly but, more importantly, prevent rheumatic fever and reduce spread
- Antibiotics do not prevent post-streptococcal glomerulonephritis
- Delaying treatment by a few days to await culture results is acceptable - still prevents rheumatic fever
Complications
Suppurative (local):
- Peritonsillar abscess (quinsy)
- Retropharyngeal/parapharyngeal abscess
- Lemierre's syndrome (Fusobacterium - septic thrombophlebitis of the internal jugular vein)
- Sinusitis, otitis media
Non-suppurative (immune-mediated):
- Acute rheumatic fever - prevented by antibiotic treatment
- Post-streptococcal glomerulonephritis - NOT prevented by antibiotics
- Streptococcal toxic shock syndrome (uncommon)
- Scarlet fever (from pyrogenic exotoxin-producing strains)
Special Situations
Infectious Mononucleosis (EBV):
- Posterior cervical lymphadenopathy + exudative pharyngitis + splenomegaly
- Monospot test: insensitive in children <2 years; may be negative in first week
- Treatment: supportive; avoid contact sports; do NOT use ampicillin/amoxicillin
Acute HIV:
- Presents similarly to EBV pharyngitis in 50-70% of cases
- Distinguish by: high-risk behaviors, absence of exudate, prominent rash, mucocutaneous ulceration
Peritonsillar Abscess:
- Presents with severe unilateral throat pain, trismus, muffled "hot potato" voice, uvular deviation to contralateral side
- Requires needle aspiration or incision and drainage plus antibiotics
Sources: Goldman-Cecil Medicine International Edition; Tintinalli's Emergency Medicine: A Comprehensive Study Guide
This is a shared conversation. Sign in to Orris to start your own chat.