ARDS in detail including ventilation strategies
Reading File
Finding Sources
Finding Sources
Searching PubMed
"acute respiratory distress syndrome" AND "mechanical ventilation"
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
I now have comprehensive material from multiple authoritative textbooks. Let me compile the complete ARDS review:
Acute Respiratory Distress Syndrome (ARDS) - Comprehensive Review
1. Definition and Classification (Berlin Criteria, 2012)
The Berlin Definition replaced the 1994 American-European Consensus Conference (AECC) criteria. It was developed by an international expert panel to address ambiguities in the older definition. ARDS is defined as a syndrome characterized by ALL of the following:
| Criterion | Requirement |
|---|---|
| Timing | Onset within 1 week of a known clinical insult, or new/worsening respiratory symptoms |
| Radiology | Bilateral pulmonary opacities on CXR or CT, not fully explained by effusions, atelectasis, or nodules |
| Origin | Respiratory failure not fully explained by cardiac failure or fluid overload |
| Oxygenation | PaO2/FiO2 (P:F ratio) ≤300 mmHg on PEEP or CPAP ≥5 cmH2O |
Severity Classification
| Severity | P:F Ratio (mmHg) | PEEP |
|---|---|---|
| Mild | 200 < P:F ≤ 300 | ≥5 cmH2O |
| Moderate | 100 < P:F ≤ 200 | ≥5 cmH2O |
| Severe | P:F ≤ 100 | ≥5 cmH2O |
The old "acute lung injury (ALI)" category is obsolete - these patients are now classified as mild ARDS. The P:F ratio must be measured on mechanical ventilation settings to remove variability introduced by varying degrees of ventilatory support.
- Fishman's Pulmonary Diseases and Disorders, p. 2492
- Current Surgical Therapy 14e, p. 3285
2. Epidemiology
-
Estimated incidence in the US: ~78.9 per 100,000 person-years (for P:F ≤300)
-
Approximately 190,600 cases per year in the United States
-
Incidence increases dramatically with age: up to 306 per 100,000 for ages 75-84 years
-
Overall mortality has improved with lung-protective ventilation but remains 30-40%
-
Incidence may have declined over time, possibly due to implementation of protective ventilation strategies
-
Fishman's Pulmonary Diseases and Disorders, p. 2492
3. Etiology and Risk Factors
Direct (Pulmonary) Causes:
- Pneumonia (bacterial, viral, fungal)
- Aspiration of gastric contents
- Pulmonary contusion
- Near-drowning
- Inhalation injury
Indirect (Extrapulmonary) Causes:
- Sepsis (most common cause overall)
- Severe trauma with shock
- Multiple blood transfusions / TRALI
- Pancreatitis
- Drug overdose / toxic ingestions
- Burns
4. Pathophysiology
ARDS evolves through distinct phases:
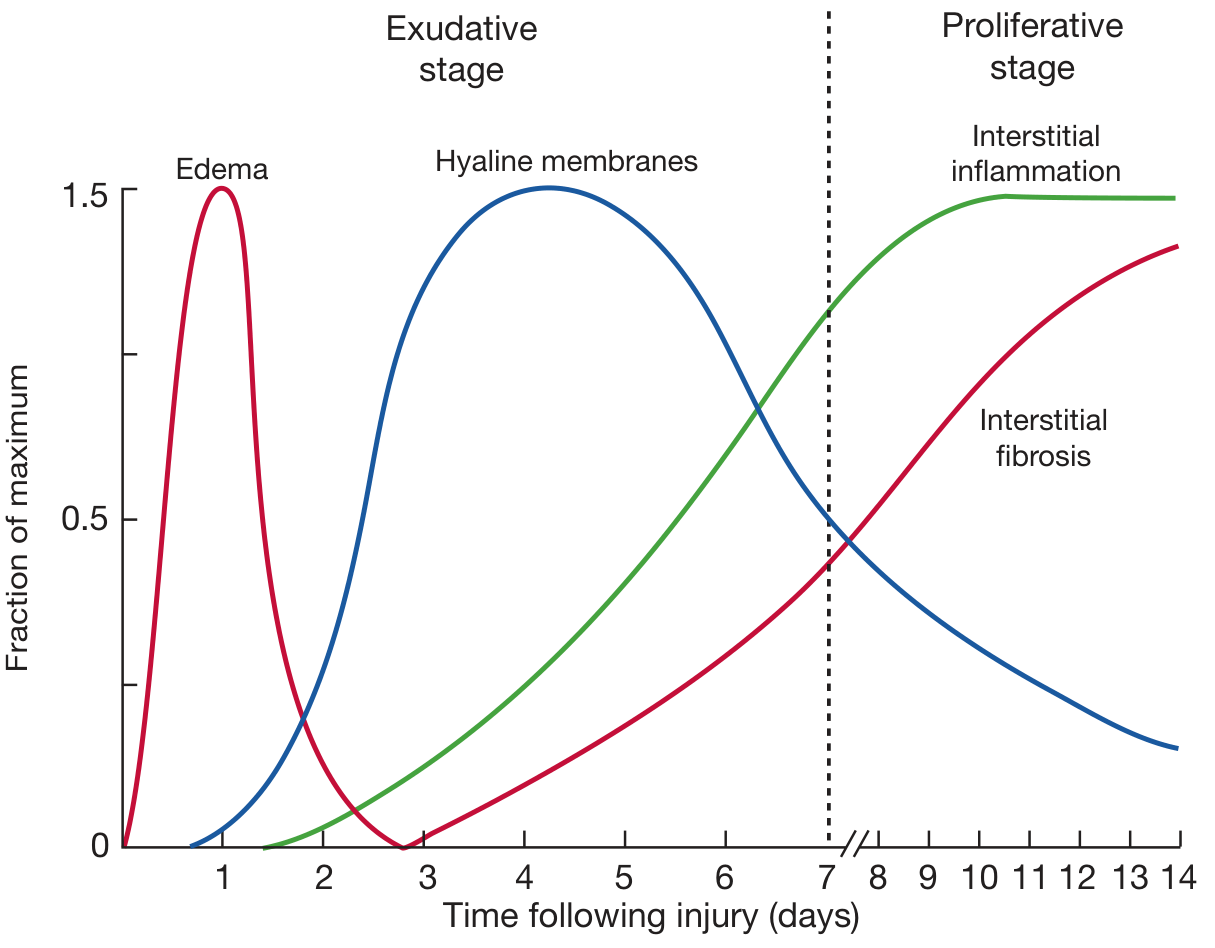
Schematic showing the time course of ARDS evolution (Fishman's Pulmonary Diseases)
Phase 1: Exudative Phase (Days 0-7)
Initiated by inflammatory cytokines, oxygen radicals, complement activation, platelet/immune cell activation, and protease generation. Pathological findings:
- Hours: Endothelial cell swelling, widened intercellular junctions, increased pinocytotic vesicles, basement membrane disruption
- Days 1-3: Interstitial and alveolar edema, capillary congestion, intra-alveolar hemorrhage
- Days 3-7: Hyaline membrane formation (condensed fibrin + plasma proteins), extensive type I pneumocyte necrosis, inflammatory cell infiltration
- Pathologic correlate: Diffuse alveolar damage (DAD) - found in ~45% of autopsied ARDS cases
Phase 2: Proliferative Phase (Days 7-14+)
- Marked interstitial and alveolar inflammation
- Type II pneumocyte proliferation (attempting to replace lost type I cells)
- Progressive interstitial fibrosis and disordered healing
- Surfactant dysfunction: increases alveolar surface tension → collapse → shunting → hypoxemia
Physiologic Consequences
- Reduced FRC from atelectasis
- Intrapulmonary shunting - deoxygenated blood bypasses flooded/collapsed alveoli
- Decreased compliance - "stiff lung," low compliance of 20-30 mL/cmH2O (normal ~80-100)
- "Baby lung" concept - aerated lung is heterogeneous and small; delivering standard tidal volumes (10-15 mL/kg) to this small open fraction causes alveolar overdistention and volutrauma
- Fishman's Pulmonary Diseases and Disorders, p. 2493
- Murray & Nadel's Textbook of Respiratory Medicine, p. 263
5. Clinical Features
- Acute onset of severe dyspnea and hypoxemia (refractory to supplemental O2)
- Bilateral infiltrates on CXR/CT (ground-glass opacification)
- CT shows heterogeneous consolidation - NOT uniformly diffuse as CXR suggests; most dense in dependent regions
- Decreased lung compliance
- Progressive respiratory failure requiring mechanical ventilation
- Elevated A-a gradient
- No clinical evidence of cardiogenic pulmonary edema
6. Ventilation Strategies
The overarching goal is to maintain adequate gas exchange while avoiding additional lung injury - termed ventilator-induced lung injury (VILI).
6.1 Lung-Protective Ventilation (ARDSNet Protocol)
The landmark ARMA trial (ARDSNet, 2000) randomized 861 patients to:
- Low VT: 6 mL/kg predicted body weight (PBW) + Pplat ≤30 cmH2O
- Traditional VT: 12 mL/kg PBW + Pplat ≤50 cmH2O
Result: Mortality 31% vs. 39.8% (P=0.007) - a landmark finding that transformed ARDS management.
Key parameters:
| Parameter | Target |
|---|---|
| Tidal Volume | 6 mL/kg predicted body weight (not actual) |
| Plateau Pressure (Pplat) | ≤30 cmH2O |
| Driving Pressure | ≤14 cmH2O |
| SpO2 target | 88-95% |
| pH target | 7.30-7.45 (permissive hypercapnia accepted) |
Permissive hypercapnia: Accepting elevated PaCO2 (up to 50-60+ mmHg) to allow low tidal volumes. Respiratory rate can be increased up to 35/min to partially compensate.
Why 6 mL/kg predicted BW? The baby lung concept: aerated lung parenchyma is functionally equivalent to a much smaller lung. Delivering standard volumes to this small fraction causes overdistention. Meta-analyses of multiple RCTs confirm the low VT approach reduces mortality.
- Murray & Nadel's Textbook of Respiratory Medicine, p. 3126
- Rosen's Emergency Medicine, p. 1237
6.2 PEEP Optimization
PEEP serves two roles in ARDS:
- Recruits collapsed alveoli → improves oxygenation, reduces shunt
- Prevents atelectrauma - cyclic opening/closing of alveoli during inspiration/expiration
PEEP strategies:
- ARDSNet FiO2/PEEP tables: Low PEEP table (titrated to FiO2) is the standard first-line approach
- Esophageal balloon-guided PEEP: Uses esophageal pressure as a pleural pressure surrogate to optimize transpulmonary pressure. Improves oxygenation but one major RCT showed no mortality benefit over FiO2-guided PEEP
- High vs. low PEEP trials (ALVEOLI, LOV, EXPRESS): High PEEP improved oxygenation but did NOT reduce mortality in unselected ARDS
Pitfall: Higher PEEP applied to already-aerated (non-recruitable) alveoli causes overdistention. The degree of recruitability varies greatly between patients. PEEP benefits depend heavily on recruitability.
- Murray & Nadel's Textbook of Respiratory Medicine, p. 264
6.3 Driving Pressure
Driving Pressure (DP) = Pplat - PEEP
-
Reflects distending pressure of the available lung
-
DP = VT / respiratory system compliance (Crs)
-
DP ≤14 cmH2O is the target; re-analysis of ARDS RCTs showed DP was the single strongest mechanical variable predicting 60-day mortality
-
Limitation: DP underestimates transpulmonary pressure in patients with high chest wall elastance (e.g., obesity, ascites). For those patients, transpulmonary driving pressure (DP minus the esophageal pressure swing) is more accurate
-
Murray & Nadel's Textbook of Respiratory Medicine, p. 264
6.4 Recruitment Maneuvers
- Sustained inflations at high pressure (e.g., 35-40 cmH2O for 30-40 seconds) to open collapsed alveoli
- Closing pressures are lower than opening pressures, so recruited alveoli stay open with adequate PEEP
- Useful for treating acute hypoxemia, but frequent/aggressive recruitment with high PEEP led to hemodynamic and respiratory complications in the ART trial (2017), which actually showed increased mortality with aggressive recruitment - so routine use is NOT recommended
6.5 Mode of Ventilation
Both volume-controlled (VC) and pressure-controlled (PC) ventilation are used in ARDS:
- VC ventilation guarantees tidal volume delivery but pressure varies with compliance changes
- PC ventilation limits peak pressure but tidal volume varies; useful when limiting peak pressure is a priority
- No strong evidence favors one mode over the other; the key parameters (low VT, Pplat ≤30) apply regardless of mode
Pressure-support ventilation (PSV) for spontaneously breathing patients: Risk of "P-SILI" (patient self-inflicted lung injury) when high respiratory drive generates excessive transpulmonary pressures, worsening VILI. Moderate-to-severe ARDS patients typically require full controlled ventilation initially.
7. Adjunctive Therapies
7.1 Prone Positioning
Most evidence-supported adjunct for moderate-severe ARDS (P:F <150)
Mechanism:
- Homogenizes ventilation from dorsal to ventral (reduces V/Q mismatch)
- Redistributes atelectasis away from dependent zones
- Reduces the dorsal-to-ventral transpulmonary pressure gradient
- Decreases VILI by making ventilation distribution more uniform
PROSEVA Trial (2013): Randomized 466 patients with ARDS and P:F <150 mmHg:
- Prone ≥16 hours/day vs. supine
- 28-day mortality: 16% (prone) vs. 32.8% (supine) - dramatic mortality benefit
- All patients received low VT ventilation; most received NMB and vasopressors
Practical requirements:
-
Minimum 16 consecutive hours prone per session
-
Neuromuscular blockade to facilitate proning and prevent patient dislodgement
-
Meticulous attention to: endotracheal tube, central lines, arterial lines, eye pressure (retinal ischemia risk), pressure ulcers on nose, ears, face
-
Absolute contraindications: Spinal instability or unstable fractures
-
Not contraindications (though challenging): Vasopressors, renal replacement therapy, obesity
-
Fishman's Pulmonary Diseases and Disorders, p. 2500
-
Washington Manual of Medical Therapeutics, p. 290
7.2 Neuromuscular Blockade (NMB)
Conflicting trial evidence:
| Trial | Patients | Intervention | Result |
|---|---|---|---|
| ACURASYS (2010) | P:F <120, early ARDS | Cisatracurium 48h + heavy sedation vs. placebo + heavy sedation | 90-day mortality 31.6% vs. 40.7% (benefit) |
| ROSE (2019) | P:F <150, moderate-severe ARDS | Cisatracurium 48h + heavy sedation vs. light sedation (no routine NMB) | No difference: 42.5% vs. 42.8% |
Interpretation: The ROSE trial used lighter sedation in controls (vs. heavy sedation in ACURASYS controls). Heavy sedation alone worsens outcomes. The ACURASYS benefit may have been from lighter sedation in the treatment arm, or from more prone positioning in that arm. NMB is NOT routinely recommended for all moderate-to-severe ARDS but may benefit patients with:
-
Severe ventilator dyssynchrony
-
High respiratory drive contributing to VILI
-
Reverse triggering
-
Murray & Nadel's Textbook of Respiratory Medicine, p. 3159
7.3 Conservative Fluid Management
- FACTT Trial (ARDSNet): In patients without shock, a conservative fluid strategy (targeting lower CVP/PAOP) reduced duration of mechanical ventilation compared to liberal strategy
- No mortality difference, but more ventilator-free days
- Goal: Minimize pulmonary edema while maintaining adequate organ perfusion
- Not applicable to patients in shock (who require resuscitation)
7.4 Corticosteroids
-
Theoretical benefit: Anti-inflammatory in exudative phase; anti-fibrotic in proliferative phase
-
Evidence is mixed overall
-
COVID-19 ARDS (special case): A meta-analysis of 7 trials (n=1703 critically ill COVID-19 patients) showed glucocorticoids reduced 28-day mortality vs. standard care/placebo
-
For non-COVID ARDS, routine corticosteroid use remains controversial and is not a standard recommendation outside of specific underlying etiologies (e.g., organizing pneumonia)
-
Washington Manual of Medical Therapeutics, p. 290
7.5 Extracorporeal Membrane Oxygenation (VV-ECMO)
Indications (when conventional therapy fails):
| Indication | Threshold |
|---|---|
| Severe hypoxemic failure with ≥50% predicted mortality | P:F <150 on FiO2 ≥0.9 + Murray score 2-3 |
| High mortality risk (≥80%) | P:F <100 on FiO2 ≥0.9 + Murray score 3-4 |
| Refractory CO2 retention | Peak plateau >30 cmH2O |
| Bridge to lung transplantation | - |
| Massive air leak (bronchopleural fistula) | - |
EOLIA Trial (2018): Early VV-ECMO vs. conventional therapy in severe ARDS - no statistically significant mortality difference at 60 days (35% vs. 46%, P=0.07), though a Bayesian re-analysis suggested probable benefit. ECMO is best reserved for carefully selected patients at specialized centers as rescue therapy.
Contraindications (relative):
-
Mechanical ventilation with high settings (FiO2 >0.9, Pplat >30 cmH2O) for ≥7 days
-
CNS hemorrhage
-
Severe immunosuppression (ANC <400/mm3)
-
Nonrecoverable condition
-
Current Surgical Therapy 14e, p. 3289
7.6 Inhaled Vasodilators (Inhaled NO, Prostacyclins)
- Improve V/Q matching by selectively vasodilating ventilated lung units
- Improve oxygenation transiently but no proven mortality benefit
- May be used as a bridge to other rescue therapies
8. Ventilator-Induced Lung Injury (VILI) - Key Mechanisms
| Mechanism | Description |
|---|---|
| Volutrauma | Alveolar overdistention from excessive tidal volumes; causes stress fractures of endothelium, epithelium, and basement membrane |
| Barotrauma | Injury from excessive pressures (pneumothorax, pneumomediastinum, subcutaneous emphysema) |
| Atelectrauma | Repetitive opening and closing of collapsed alveoli during each breath cycle |
| Biotrauma | Mechanical stretch triggers inflammatory mediator release (IL-6, IL-8, TNF) → systemic inflammation → multiorgan failure |
| Oxygen toxicity | High FiO2 generates reactive oxygen species; though less clear in humans, minimizing FiO2 is still recommended |
Mechanical Power is an emerging concept that integrates all sources of VILI energy delivery into a single metric (including respiratory rate, tidal volume, driving pressure, and PEEP). A 2026 systematic review (PMID: 42153811) confirmed that mechanical power is associated with mortality in critically ill ventilated patients.
9. Summary: Ventilation Strategy Quick Reference
ARDS Lung-Protective Ventilation (Mode: Volume-Controlled AC)
─────────────────────────────────────────────────────
VT: 6 mL/kg PREDICTED body weight
Pplat: ≤30 cmH2O
Driving P: ≤14 cmH2O
RR: Start 14-20/min; increase for hypercapnia (max 35/min)
PEEP: FiO2/PEEP table (ARDSNet); titrate to oxygenation
FiO2: Lowest needed to maintain SpO2 88-95%
I:E ratio: 1:2 (adjust for dyssynchrony / iPEEP)
Permissive hypercapnia: Accept PaCO2 up to 50-60+ mmHg if pH >7.20
RESCUE THERAPIES (for P:F <150 despite the above):
1. Prone positioning ≥16h/day (strongest evidence: 50% ↓ mortality)
2. Inhaled NO / prostacyclins (oxygenation bridge)
3. Recruitment maneuver (use cautiously; avoid routine use)
4. VV-ECMO at experienced center
10. Complications
- Barotrauma (pneumothorax, pneumomediastinum)
- Ventilator-associated pneumonia (VAP)
- Pulmonary hypertension and cor pulmonale
- Multiorgan dysfunction (biotrauma-mediated)
- Post-ARDS pulmonary fibrosis
- ICU-acquired weakness (especially with prolonged NMB)
- Psychological sequelae (PTSD, depression, cognitive impairment)
Key References:
- Fishman's Pulmonary Diseases and Disorders (Chapter 141)
- Murray & Nadel's Textbook of Respiratory Medicine (Chapters 11, 31, 134)
- Rosen's Emergency Medicine (Chapter 2)
- Washington Manual of Medical Therapeutics (Chapter 8)
- Current Surgical Therapy 14e (Chapter 16)
- ARMA Trial: ARDS Network. N Engl J Med. 2000;342:1301-1308
- PROSEVA Trial: Guérin et al. N Engl J Med. 2013;368:2159-2168
- Berlin Definition: Ranieri VM et al. JAMA. 2012;307:2526-2532
Recent Evidence Alert: A 2026 systematic review (PMID: 42153811) confirmed mechanical power is associated with mortality in mechanically ventilated patients, supporting efforts to minimize all components of VILI energy delivery. A 2026 systematic review on ARDS complications (PMID: 41906154) is now available in Critical Care.
This is a shared conversation. Sign in to Orris to start your own chat.