Suspected pheochromocytoma patient having normal free metanephrine
Reading File
Finding Sources
Finding Sources
Searching PubMed
pheochromocytoma normal metanephrine diagnosis
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Finding Sources
Reading File
I now have everything needed for a thorough, well-sourced answer. Here is the comprehensive response:
Suspected Pheochromocytoma with Normal Plasma Free Metanephrines
Why This Matters
Plasma free metanephrines (metanephrine + normetanephrine) are the first-line screening test for pheochromocytoma, with sensitivity approaching 99% and specificity of 85-89%. A negative result is therefore highly reassuring - but the clinical picture still determines the next step.
As Sabiston states: "The primary usefulness of plasma free metanephrine testing is to exclude pheochromocytoma when the test result is negative."
When to Accept a Negative Result
If the pretest probability is low (e.g., incidentally found hypertension, nonspecific symptoms) and there are no confounding factors, a normal plasma metanephrine result is sufficient to effectively rule out pheochromocytoma. Observation with consideration for repeat testing is appropriate.
When to Keep Investigating Despite Normal Plasma Metanephrines
Several scenarios warrant continued workup:
1. Pre-analytical/Technical Causes of False-Negative Results
- Interfering medications taken before the test (some can lower catecholamine output)
- Sample drawn during a normotensive or asymptomatic interval - pheochromocytomas may secrete episodically
- Improper sample handling or laboratory assay variability
2. "Silent" or Minimally Secreting Pheochromocytoma
Sabiston explicitly warns: "A growing number of pheochromocytomas identified incidentally on imaging may be minimally secreting; these so-called 'silent pheos' may require a high clinical index of suspicion for diagnosis." These can have normal metanephrines.
3. Paragangliomas - Especially Head and Neck
From the National Kidney Foundation Primer: "Paragangliomas may be biochemically silent, especially when originating in the neck and base of the skull." These tumors may not produce detectable catecholamine metabolites in plasma.
4. SDHx-Mutation-Related Tumors
SDHB/SDHD/SDHC-mutant paragangliomas more often produce dopamine rather than norepinephrine/epinephrine. In these cases, measuring plasma methoxytyramine (the dopamine metabolite) is critical - it will be missed by a standard metanephrine panel.
Recommended Next Steps (Diagnostic Algorithm)
Following the Sabiston/Tietz framework when suspicion persists despite normal plasma metanephrines:
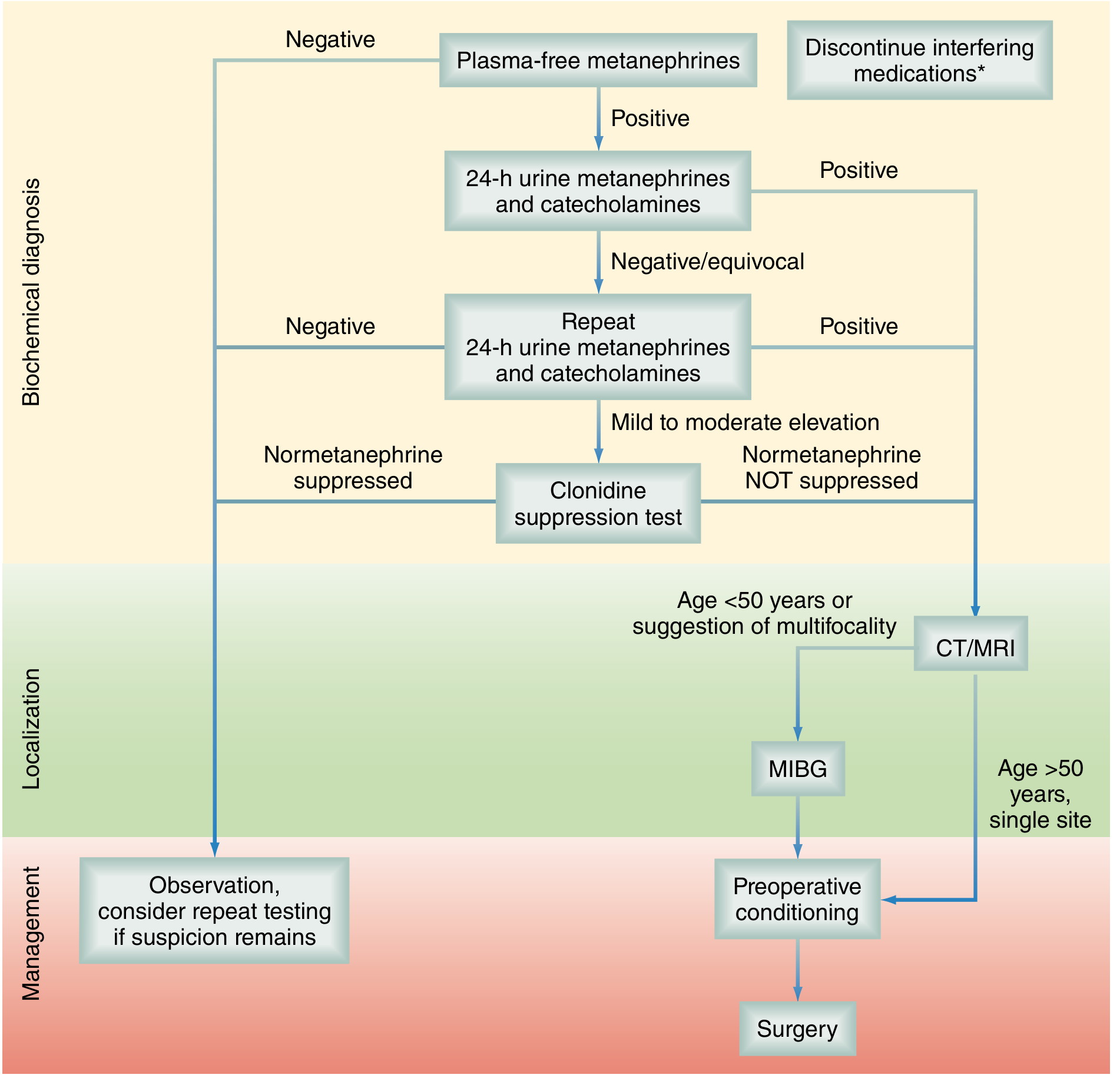
Step 1: 24-hour Urine Catecholamines and Fractionated Metanephrines
- This has lower sensitivity (88%) but very high specificity (99.6%)
- Cutoffs are set at ~2x the upper reference range for maximum specificity
- A positive result in any single fraction (norepinephrine, epinephrine, dopamine) is considered positive
- Repeat the collection twice - two negative 24-hr urines exclude pheo in almost all cases
| Test | Sensitivity | Specificity | Cutoff |
|---|---|---|---|
| Plasma free metanephrine | 99% | 85-89% | 0.3 nmol/L |
| Plasma free normetanephrine | 99% | 85-89% | 0.6 nmol/L |
| Urinary total metanephrines | 71% | 99.6% | 6.6 µmol/day |
| Urinary norepinephrine | 50% | 99.6% | 1005 nmol/day |
| Urinary epinephrine | 29% | 99.6% | 191 nmol/day |
(From Sabiston Textbook of Surgery, 14e, Table 75.4)
Step 2: Add Plasma Methoxytyramine
- For dopamine-secreting SDHx tumors and head/neck paragangliomas, this is the key marker
Step 3: Clonidine Suppression Test (for equivocal results / elevated normetanephrine but borderline)
- Indication: Patients with mildly elevated plasma normetanephrine (borderline/equivocal) - NOT useful for isolated metanephrine elevation
- Protocol (Tietz): Clonidine 4.3 µg/kg orally; measure plasma normetanephrine at baseline and 3 hours later
- Positive for pheo: Normetanephrine fails to fall by >40% AND remains above 112 pg/mL (0.61 nmol/L) - clonidine suppresses sympathetic-nerve-derived norepinephrine but not tumor-derived catecholamines
- Negative: Suppression to below 112 pg/mL OR fall of >40%
Step 4: Anatomic Imaging (if biochemistry points positive)
- CT abdomen/pelvis (first choice for anatomic definition)
- MRI (slightly more sensitive, better for extra-adrenal/multifocal)
Step 5: Functional Imaging (if multifocal or malignant disease suspected)
- 68Ga-DOTATATE PET/CT - currently the best option (lesion detection 97.6%), superior to MIBG
- MIBG scan (sensitivity 77-90%, high specificity) - still used when PET unavailable
- 18F-DOPA or 18F-dopamine PET/CT - better than MIBG, especially for SDHx tumors
Common Confounders to Rule Out (Before Attributing False-Negative)
These conditions cause symptoms mimicking pheo but can also interfere with assays:
- Sympathomimetics (in OTC cold remedies) - raise catecholamines
- Tricyclic antidepressants / psychotropic drugs - elevate catecholamines (more relevant for false-positives)
- Acetaminophen - interferes with the plasma free metanephrine assay
- Phenoxybenzamine - frequently started empirically, can confound results
- MAOIs - artificially raise urinary metanephrines
- Acute physical/psychological stress, critical illness, acute pain - can give misleading results in either direction
- Testing during asymptomatic intervals in a paroxysmal secretor
Clinical Bottom Line
| Scenario | Action |
|---|---|
| Low clinical suspicion + normal plasma metanephrines | Diagnosis effectively excluded; observe |
| High clinical suspicion + normal plasma metanephrines | Proceed to 24-hr urine (x2); add methoxytyramine |
| Equivocal urine results (normetanephrine mildly elevated) | Clonidine suppression test |
| Isolated metanephrine elevation | Clonidine test not useful; proceed to imaging |
| Normal biochemistry but adrenal mass on imaging | Consider SDHx genetic testing, 68Ga-DOTATATE PET |
| Head/neck location suspected | Plasma methoxytyramine, MRI, functional imaging |
A "wait and re-test" strategy at 6 months is also valid when the pretest probability remains moderate but all current testing is negative - progressive increases in metanephrine levels over time justify proceeding to imaging even if an individual result is borderline.
Sources: Sabiston Textbook of Surgery 14e, pp. 1571-1573 | Tietz Textbook of Laboratory Medicine 7e | Current Surgical Therapy 14e
This is a shared conversation. Sign in to Orris to start your own chat.