USG for inguinal region
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Loading Image
Loading Image
Loading Image
Loading Image
Finding Sources
Here is a comprehensive overview of Ultrasound (USG) of the Inguinal Region:
Ultrasound of the Inguinal Region
Indications
USG of the inguinal region is used to evaluate:
- Inguinal hernia (indirect, direct, femoral)
- Inguinal lymphadenopathy
- Scrotal/groin swelling (hydrocele, varicocele, epididymal cyst)
- Undescended testis (cryptorchidism)
- Femoral artery aneurysm / vascular pathology
- Psoas abscess, soft tissue masses, lipoma
- Saphena varix
- Sportsman's hernia (groin pain in athletes)
- Incarceration/strangulation assessment in known hernia
Anatomy of the Inguinal Region
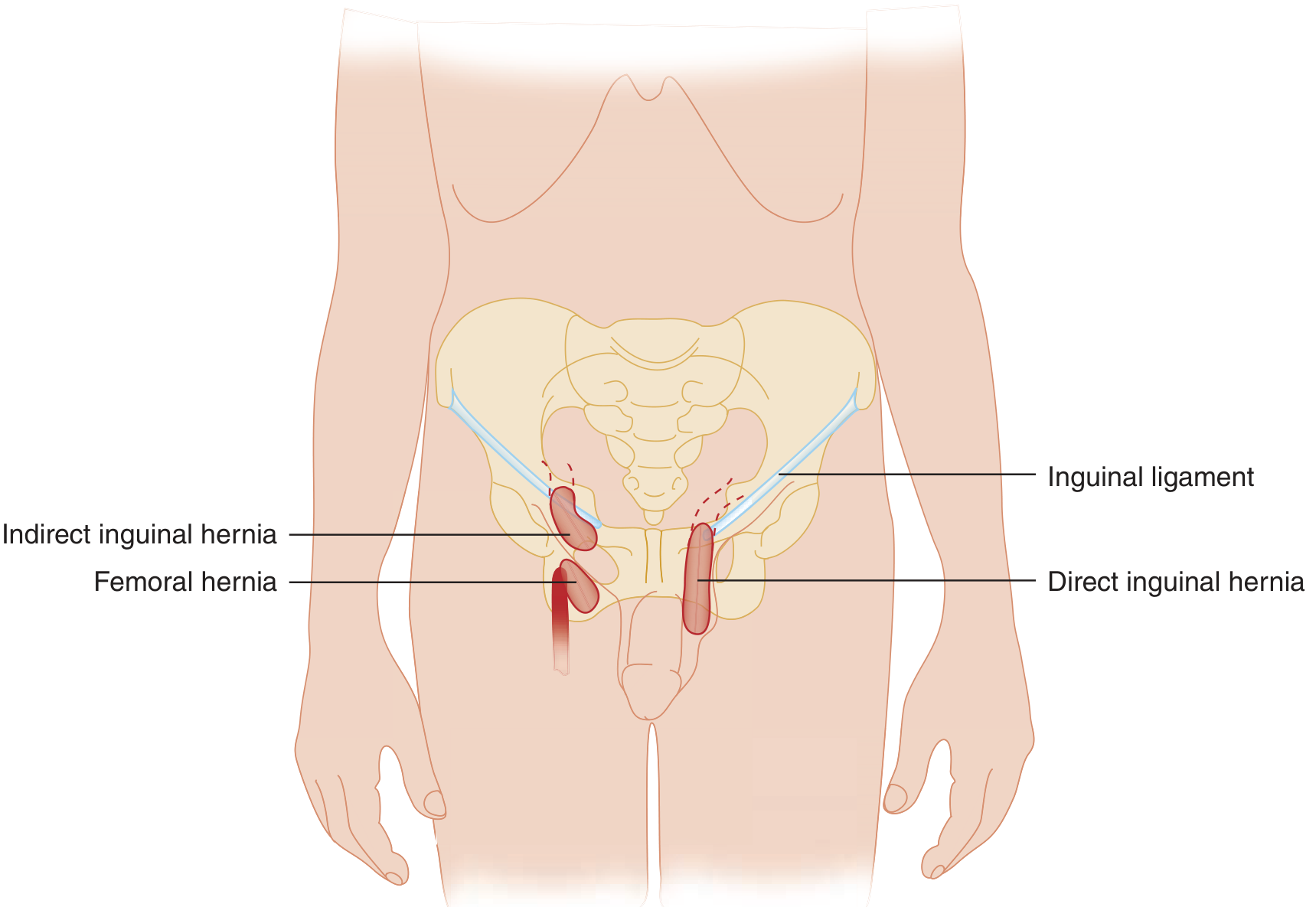
Key landmarks visible on USG:
- Inguinal ligament (hyperechoic band, ASIS to pubic tubercle)
- Inferior epigastric vessels — used to distinguish direct vs. indirect hernia
- Femoral artery and vein — lateral to medial order: Nerve, Artery, Vein, Empty space, Lymphatics (NAVEL)
- Spermatic cord (in males) / round ligament (in females)
- Inguinal canal — traversed by the spermatic cord / round ligament
Technique
- Probe: High-frequency linear probe (7.5–15 MHz); use curvilinear for obese patients
- Patient position: Supine; standing position helpful for hernias and varicocele
- Scan planes: Longitudinal and transverse
- Dynamic maneuvers: Valsalva maneuver and standing position are essential — movement of abdominal contents through the canal is required to confirm hernia
- DASH (Dynamic Abdominal Sonography for Hernia): a systematic real-time technique comparing both sides; good sensitivity in experienced hands compared to CT
USG Findings in Hernia
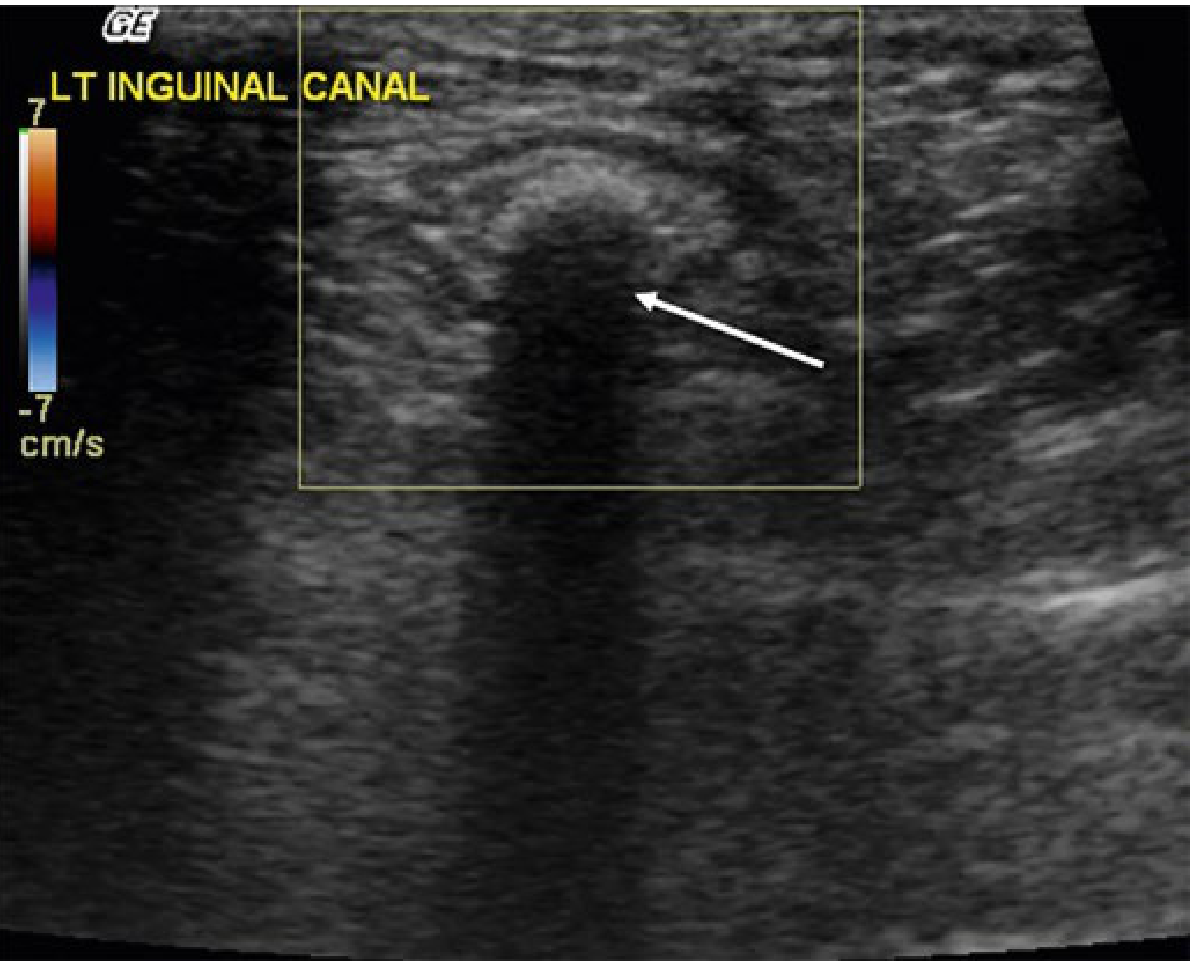
| Finding | Significance |
|---|---|
| Bowel loop in inguinal canal | Hernia (bowel hernia) |
| Echogenic fat in canal | Omental/fatty hernia |
| Posterior acoustic shadowing | Air in bowel lumen |
| Absence of peristalsis | Incarceration |
| Free fluid in hernia sac | Incarceration / early strangulation |
| Hyperechoic fat, bowel wall thickening | Strangulation |
| No color flow on Doppler | Vascular compromise |
Differentiating Hernia Type by US
- Indirect inguinal: Hernia sac lies lateral to the inferior epigastric vessels, traverses through the deep inguinal ring along the inguinal canal
- Direct inguinal: Protrudes medial to the inferior epigastric vessels through Hesselbach's triangle (floor of inguinal canal)
- Femoral: Lies below the inguinal ligament, medial to the femoral vein
USG Findings in Incarcerated Hernia

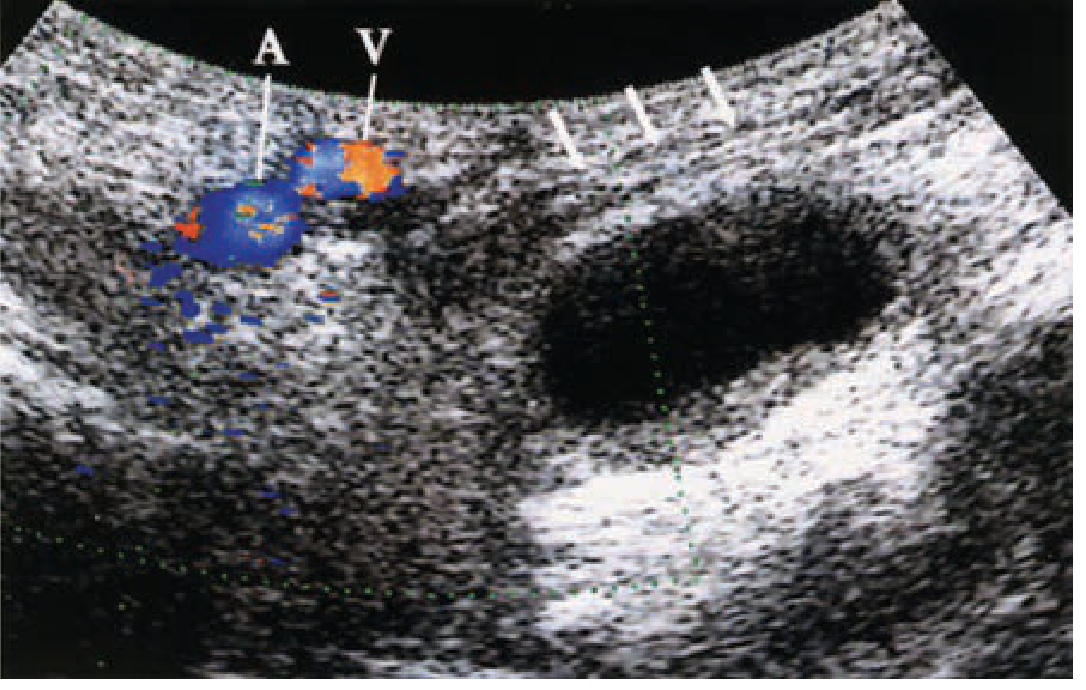
Doppler US in strangulation:
- Thin-walled veins are compressed before arteries → Doppler may still show arterial flow even in early strangulation
- Preserved arterial flow with venous obstruction → increased intravascular pressure → free fluid in the hernia sac on B-mode (sensitive sign)
- Doppler is insensitive for strangulation alone; B-mode free fluid is a better marker
Diagnostic Performance
| Modality | Sensitivity | Specificity |
|---|---|---|
| Ultrasound | 86% | 77% |
| CT | 80% | 65% |
| MRI | 95% | 96% |
| Herniography | Highest (invasive) | Highest |
- US is first-line in children (no radiation) and preferred in pregnancy
- US is operator- and body habitus-dependent; false negatives occur when Valsalva is not performed
- CT is best for occult or atypical hernias (Spigelian, obturator) and in the acute setting
- MRI is used when US is inconclusive, especially for sportsman's hernia (musculoskeletal cause)
Other Inguinal USG Findings
| Condition | USG Appearance |
|---|---|
| Inguinal lymphadenopathy | Round/oval hypoechoic nodes, loss of fatty hilum in malignancy, increased vascularity |
| Femoral artery aneurysm | Fusiform/saccular dilation with turbulent flow on Doppler |
| Saphena varix | Compressible cystic structure at saphenofemoral junction, fills on Valsalva |
| Psoas abscess | Hypoechoic fluid collection lateral to iliac vessels, tracking from lumbar spine |
| Varicocele (in canal) | Dilated tortuous veins >3 mm, fills on Valsalva |
| Undescended testis | Oval structure in inguinal canal, smaller than normal testis |
| Lipoma of cord | Echogenic, non-compressible mass in spermatic cord |
Clinical Pearls
- Always perform bilateral comparative scanning
- Valsalva and standing are mandatory dynamic maneuvers
- In females with inguinal hernia, ultrasound with Doppler should be done to assess for ovarian content and viability (risk of torsion)
- Free fluid in the hernia sac is the most useful B-mode sign of incarceration/strangulation
- Absence of peristalsis in a herniated bowel loop suggests incarceration; presence of peristalsis implies bowel resection is less likely at surgery
Sources: Tintinalli's Emergency Medicine, 9e; Rosen's Emergency Medicine; Schwartz's Principles of Surgery, 11e; Yamada's Textbook of Gastroenterology, 7e
This is a shared conversation. Sign in to Orris to start your own chat.