GAS gangrene
Reading File
Finding Sources
Finding Sources
Searching PubMed
"gas gangrene" AND "Clostridium"
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive information from multiple authoritative textbooks. Here is the full, detailed answer:
Gas Gangrene (Clostridial Myonecrosis)
Gas gangrene is one of the most fulminant, life-threatening infections in humans - a true surgical emergency that is invariably fatal if untreated.
Definition and Synonyms
Gas gangrene is also known as clostridial myonecrosis. It refers to a rapidly progressive, necrotizing infection of muscle and soft tissue caused by histotoxic Clostridium species, characterized by gas in the tissues, widespread necrosis, and systemic shock.
Etiology
| Organism | Notes |
|---|---|
| C. perfringens | ~90% of traumatic cases; most important |
| C. septicum | Associated with spontaneous (non-traumatic) gangrene; linked to occult GI malignancy |
| C. novyi | Seen in injection drug users (black-tar heroin) |
| C. histolyticum | Less common |
| C. sordellii (now Paeniclostridium) | Postpartum, post-abortion, injection drug use |
| C. tertium, C. fallax, C. bifermentans | Rare |
Note: Nonclostridial organisms are found in approximately 85% of "gas gangrene" infections overall - mixed aerobic/anaerobic infections are common. However, Clostridium species cause the most dramatic and deadliest cases. - Campbell's Operative Orthopaedics 15th Ed 2026
Pathogenesis
Requirements for Development
- Anaerobic environment - devitalized tissue, ischemia, foreign bodies, low oxidation-reduction potential
- Wound contamination with spores or vegetative organisms
- Delay in surgical management - even a few hours allows bacterial multiplication and toxin production
Toxins of C. perfringens
C. perfringens produces at least 12 toxins; the two most critical are:
| Toxin | Mechanism |
|---|---|
| α-toxin (phospholipase C / lecithinase) | Hemolytic; destroys platelets and PMNs; causes widespread capillary damage; forms intravascular platelet-neutrophil aggregates that impede inflammatory cell trafficking to the wound; depresses myocardial contractility and reduces vascular resistance |
| θ-toxin (perfringolysin O) | Contributes to tissue destruction and oxygen deprivation |
The combined effect of α-toxin and θ-toxin produces:
- Rapid, irreversible ischemic muscle necrosis
- A characteristic paucity of leukocytes in infected tissue (despite leukocyte accumulation in adjacent vessels)
- Systemic absorption leading to shock
C. septicum produces its own α-toxin (unrelated to C. perfringens α-toxin), causing cell death and changes in microvascular perfusion.
Classification
1. Traumatic Gas Gangrene
The most common type. Organisms are introduced into devitalized tissue.
Predisposing conditions:
- Crush-type injuries
- Laceration of large/medium arteries
- Open fractures of long bones contaminated with soil or clothing
- Penetrating abdominal wounds (gut flora contamination)
- Post-surgical (especially bowel/biliary tract surgery - ~30% of cases)
- Amputation of ischemic limb
- Injection drug use (subcutaneous/intramuscular injections)
- Hip surgery or adrenaline injections near fecal flora sources
Incubation period: As short as 6 hours, usually < 4 days (mean < 24 hours)
2. Spontaneous (Non-traumatic) Gas Gangrene
- Caused mainly by C. septicum
- Arises via hematogenous seeding of normal muscle from a GI tract portal of entry
- Associated with: colonic malignancy, inflammatory bowel disease, diverticulitis, necrotizing enterocolitis, leukemia, neutropenic enterocolitis after chemotherapy
- Key point: Spontaneous gas gangrene due to C. septicum should prompt a search for an occult GI malignancy
Clinical Features
Progression (Characteristic Sequence)
- Sudden, excruciating pain at the wound site - the earliest and most reliable symptom
- Brawny edema and induration of surrounding tissue
- Skin progresses: pale → bronze/tense → dark red/purple discoloration → violaceous/hemorrhagic bullae
- Wound discharge: thin serosanguineous, "dishwater" appearance, foul-sweet odor, with gas bubbles
- Crepitus on palpation (gas in soft tissues)
- Rapid systemic toxemia: fever, tachycardia, hypotension, tachypnea, altered consciousness
- Refractory hypotension (unresponsive to fluid resuscitation)
- Brisk intravascular hemolysis (~15% of patients are bacteremic)
- Renal failure and multiorgan failure
"The margin between healthy and necrotic tissue often advances several inches per hour despite appropriate antibiotic therapy." - Harrison's Principles of Internal Medicine 22E (2025)
"The infection can progress 10 cm per hour." - Campbell's Operative Orthopaedics 15th Ed 2026
Critically important surgical finding: Infected muscle does not bleed or contract when stimulated - this is pathognomonic of myonecrosis.
Clinical Photos
Gas gangrene of the forearm - note the massive brawny edema, skin discoloration progressing from red to violaceous, with bullae formation:

Histopathology
Characteristic histologic triad:
- Widespread muscle necrosis
- Paucity of leukocytes in infected tissue (key differentiating feature from other infections)
- Leukocyte accumulation in adjacent vessels (due to α and θ toxin blockade of inflammatory cell trafficking)
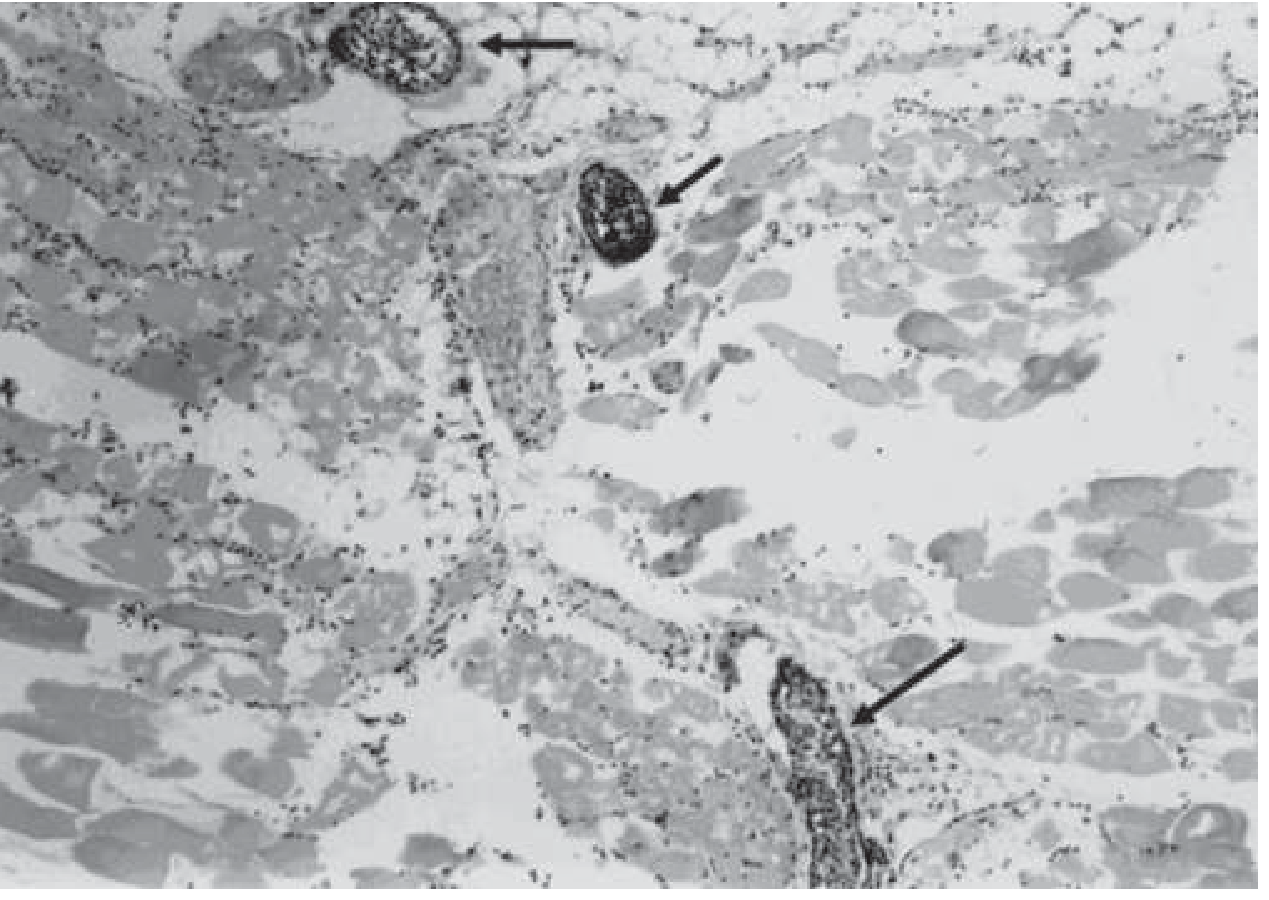
Histopathology of experimental gas gangrene due to C. perfringens demonstrating widespread muscle necrosis, paucity of leukocytes in infected tissues, and accumulation of leukocytes in adjacent vessels (arrows). - Harrison's Principles of Internal Medicine 22E
Diagnosis
Clinical
- Sudden severe pain + gas in tissue + rapidly progressive wound = gas gangrene until proven otherwise
- Do not delay surgery to obtain imaging if clinical suspicion is high
Gram Stain (most important rapid test)
- Large gram-positive (or gram-variable) rods (boxcar-shaped)
- Absence of inflammatory cells - this is the key finding
- Widespread soft tissue necrosis visible
Imaging
- X-ray: Gas in soft tissues (feathery pattern along muscle planes)
- CT/MRI: Most useful for determining extent of infection and fascial plane involvement; can help guide surgical approach
- Needle aspiration/punch biopsy: May yield etiologic diagnosis in ~20% of cases; never replaces surgical exploration
Blood Cultures
- Especially important in spontaneous gas gangrene - bacteremia usually precedes cutaneous manifestations by several hours
Nucleic Acid Testing
- Too low sensitivity to be relied upon
Treatment
Gas gangrene is a surgical emergency. All three pillars are required simultaneously.
1. Surgery (Most Important)
- Emergent, wide surgical debridement - the single best life-saving intervention
- All devitalized tissue must be widely resected back to healthy, viable, bleeding muscle
- Fasciotomy for compartment syndrome
- Amputation of the extremity may be necessary to control spread
- Closure of traumatic wounds should be delayed 5-6 days until infection-free
- Do not delay surgery for imaging or cultures
2. Antibiotics
| Drug | Role |
|---|---|
| Penicillin G | First-line; effective based on in vitro sensitivity |
| Clindamycin | Combined with penicillin; preferred because it inhibits bacterial protein/toxin production, is insensitive to bacterial load or growth phase, and modulates host immune response |
| Duration | 10-14 days |
"In the penicillin-allergic patient, clindamycin may be used alone." - Harrison's 22E
- For polymicrobial infections: β-lactam/β-lactamase inhibitor combinations or carbapenems + clindamycin
- Other active agents: metronidazole, tetracyclines, chloramphenicol, aminoglycosides
- Note: Emerging clindamycin resistance in C. perfringens has been reported (Canada, Taiwan, UK, Spain); all isolates remain universally susceptible to penicillin
3. Hyperbaric Oxygen (HBO)
- Used as an adjunct at specialized centers
- Rationale: raises tissue pO₂, inhibiting anaerobic bacterial growth
- Should never delay surgery or antibiotics
- Evidence remains controversial; used when surgery has already controlled the primary infection
Prevention
- Avoid prolonged tourniquet application
- Prompt surgical exploration of traumatic wounds
- Debridement of devitalized tissue, removal of foreign bodies, drainage of hematomas
- Early definitive surgical management (time from injury to OR is critical - peacetime survival better than wartime due to faster access to care)
Prognosis
| Factor | Effect on Prognosis |
|---|---|
| Extremity involvement | Better (vs. trunk/visceral) |
| Younger age | Better |
| Single limb involvement | Better |
| Early aggressive surgical debridement | Better |
| Shock at presentation | Worse (40% mortality) |
| Advanced age | Worse |
| Leukopenia | Worse |
| Hemolysis | Worse |
| Bacteremia | Mortality exceeds 50% |
| Trunk/visceral involvement | Worse |
- Overall mortality: ~20-40% historically; recent reports show survival rates >90% with aggressive management
- Without treatment: invariably fatal
- Death most often occurs within 48 hours when suppuration, gas, and toxemia are all present
Comparison with Anaerobic Cellulitis
| Feature | Gas Gangrene (Myonecrosis) | Anaerobic Cellulitis |
|---|---|---|
| Gas in tissue | Present (moderate) | Present (more prominent) |
| Pain | Severe | Mild |
| Swelling | Severe | Moderate |
| Muscle involvement | Yes - primary | No |
| Systemic toxicity | Severe | Mild |
| Prognosis | Grave | Better |
Key Pearls
- Gram stain showing gram-positive rods WITHOUT neutrophils = gas gangrene (toxins prevent leukocyte migration)
- Spontaneous gas gangrene by C. septicum = rule out occult colon cancer
- Incubation can be as short as 6 hours after trauma
- The absence of leukocytes both clinically (no pus) and histologically is pathognomonic
- Penicillin + clindamycin is the preferred antibiotic combination; clindamycin's superiority relates to toxin inhibition
- Surgery cannot wait - radical amputation may be the only life-saving option
- Muscle that is non-bleeding and non-contracting on surgical exploration confirms myonecrosis
Sources:
- Harrison's Principles of Internal Medicine 22E (2025), Ch. 159
- Goldman-Cecil Medicine (International Edition, 2022)
- Campbell's Operative Orthopaedics 15th Ed (2026)
- Sherris & Ryan's Medical Microbiology, 8th Ed
Recent literature: A 2024 comprehensive review (PMID 39065232) and a 2025 review (PMID 40819362) confirm the current management approach remains surgery + penicillin/clindamycin, with hyperbaric oxygen as adjunct therapy. No major guideline changes since the core framework established by Stevens et al.
This is a shared conversation. Sign in to Orris to start your own chat.