Write a short note on Refeeding syndrome for My MD Anaesthesiology exam from Standard books
Reading File
Finding Sources
Finding Sources
Searching PubMed
"refeeding syndrome"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
I have comprehensive information from multiple standard textbooks. Let me now compile the exam note.
Refeeding Syndrome
(For MD Anaesthesiology Examination)
Definition
Refeeding syndrome is a potentially life-threatening constellation of metabolic and electrolyte disturbances that occurs when nutrition - oral, enteral, or parenteral - is reinstituted after a period of prolonged starvation or severe malnutrition. The hallmark is hypophosphatemia, accompanied by hypokalemia, hypomagnesemia, thiamine deficiency, fluid shifts, and sodium retention.
(Sources: Yamada's Textbook of Gastroenterology 7e; Sabiston Textbook of Surgery; Schwartz's Principles of Surgery 11e)
Historical Background
First described after World War II when severely malnourished Japanese prisoners of war were refed and subsequently developed electrolyte abnormalities and sudden death.
Pathophysiology
During Starvation (Catabolic State):
- Fat and amino acids become the primary fuel sources
- Intracellular phosphate, potassium, and magnesium are progressively depleted
- Serum electrolyte levels may paradoxically remain normal (maintained by bone storage pools and extracellular buffering)
- Insulin secretion is low; gluconeogenesis dominates
On Refeeding (Anabolic Switch):
- Reintroduction of carbohydrates triggers a surge in insulin secretion
- Insulin activates Na-K ATPase → drives potassium, phosphate, and magnesium into cells
- Phosphate is additionally consumed for ATP synthesis and glycolysis (phosphorylation of glucose)
- Thiamine (vitamin B1) is a cofactor for pyruvate dehydrogenase; it is rapidly consumed - pyruvate cannot enter the Krebs cycle, leading to lactic acidosis
- Sodium and water retention occur → fluid overload
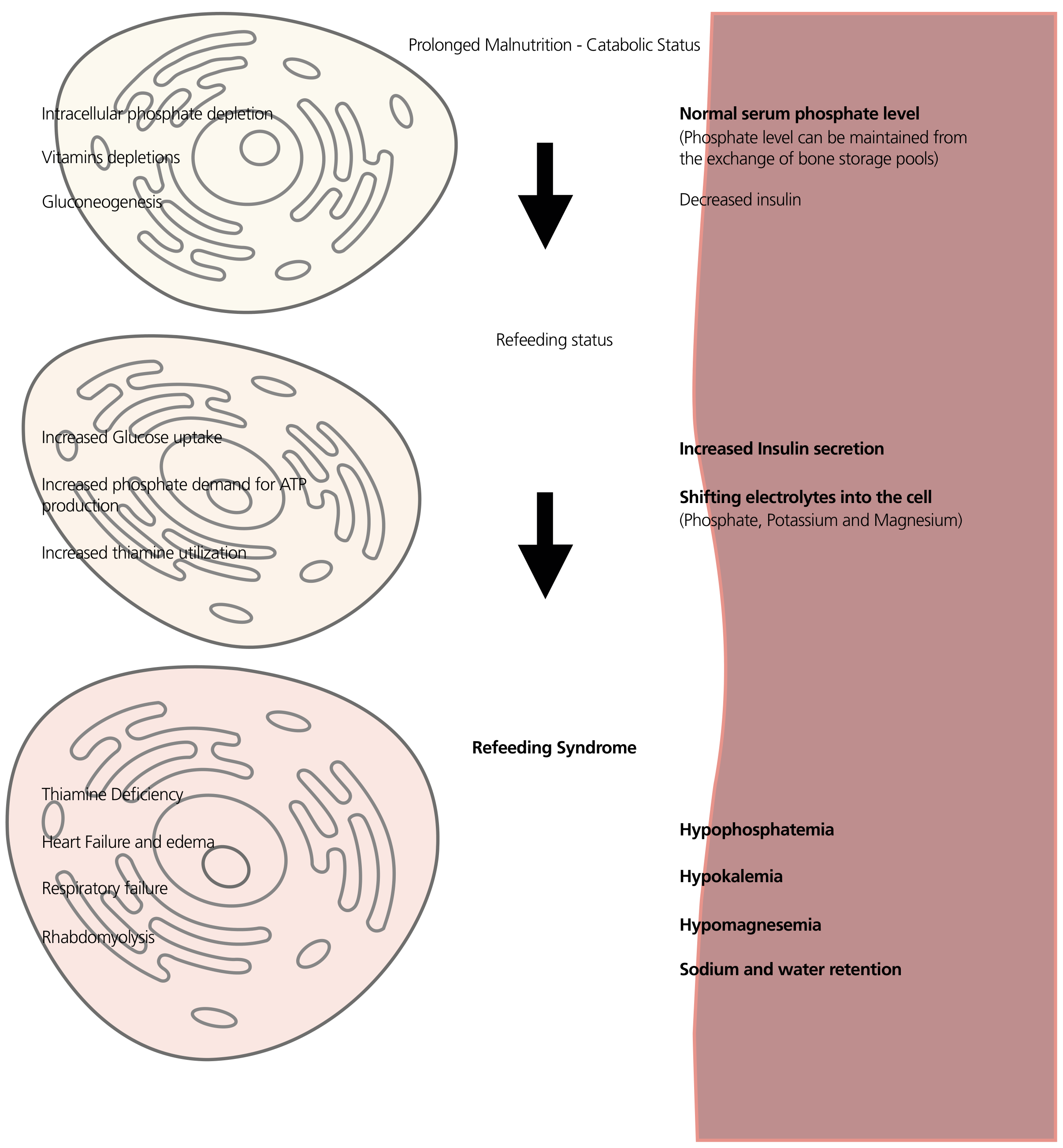
(Figure: Yamada's Textbook of Gastroenterology 7e - Pathogenesis of Refeeding Syndrome)
Electrolyte Abnormalities
| Electrolyte | Direction | Consequence |
|---|---|---|
| Phosphate | ↓↓ (Hallmark) | Cardiac arrhythmia, respiratory failure, rhabdomyolysis, cardiac arrest |
| Potassium | ↓ | Arrhythmias, muscle weakness, paralysis |
| Magnesium | ↓ | Worsens hypokalemia, seizures, arrhythmias |
| Calcium | ↓ | Tetany, seizures |
| Thiamine | Depleted | Wernicke's encephalopathy, lactic acidosis |
Clinical Features
- Cardiac: Arrhythmias (life-threatening), heart failure, oedema
- Respiratory: Respiratory failure (diaphragmatic weakness from hypophosphatemia)
- Neurological: Confusion, seizures, Wernicke syndrome
- Muscular: Profound weakness, rhabdomyolysis
- Metabolic: Lactic acidosis (thiamine deficiency), severe hyperglycaemia (blunted basal insulin secretion)
- Haematological: Haemolytic anaemia, impaired leucocyte function (ATP-dependent)
Patients at Risk (NICE Criteria - Bailey & Love 28e / Tietz 7e)
High Risk - ONE of the following:
- BMI < 16 kg/m²
- Unintentional weight loss > 15% within the last 3-6 months
- Little or no nutritional intake for > 10 days
- Low potassium, phosphate, or magnesium before refeeding
Moderate Risk - TWO or more of the following:
- BMI 16-18.5 kg/m²
- Unintentional weight loss > 10% within 3-6 months
- No/negligible nutrition for > 5 days
- History of alcohol abuse, or drugs including insulin, chemotherapy, antacids, or diuretics
Clinical conditions commonly associated: anorexia nervosa, chronic alcoholism, prolonged starvation, cancer, kwashiorkor, inflammatory bowel disease, post-bariatric surgery, ICU patients on delayed nutritional support.
Diagnosis
Recent consensus criteria (Tietz Laboratory Medicine 7e):
| Severity | Criterion |
|---|---|
| Mild | Decrease in phosphate / potassium / magnesium of 10-20% |
| Moderate | Decrease of 20-30% |
| Severe | Decrease of > 30% |
Prevention and Management
Step 1 - Identify At-Risk Patients
Screen all patients before initiating nutritional support.
Step 2 - Correct Deficits Before Refeeding
- Correct electrolyte (phosphate, potassium, magnesium, calcium) and fluid deficits before starting nutrition
- Thiamine 100 mg IV/oral must be given before the first feed or any glucose-containing fluids (especially in alcoholism, prolonged starvation)
- Continue thiamine 100 mg/day for 5-7 days in high-risk patients
Step 3 - Start Nutrition Slowly
- Begin at 10 kcal/kg/day (or 50% of estimated energy requirements on Day 1)
- Gradually increase over 4-7 days to meet full requirements
- For PN: start with only 50% dextrose on Day 1
- Supplement potassium (20-30 mmol/L), phosphate (20-30 mmol/day), magnesium, and multivitamins routinely
Step 4 - Monitor Closely
- Vital signs and fluid balance daily
- Serum electrolytes (phosphate, potassium, magnesium, calcium, glucose) at baseline, then daily for the first week
- Correct deficits aggressively as they evolve
- Strict glycaemic control (insulin infusion if hyperglycaemia on PN)
Anaesthesia Relevance
- Preoperative assessment - recognize malnourished patients at risk; postpone elective surgery if possible to optimize nutrition
- Perioperative glucose-containing fluids (e.g. dextrose saline, TPN) can trigger refeeding syndrome in fasted, malnourished ICU patients - always give thiamine first
- Respiratory failure from hypophosphatemia can cause failure to wean from mechanical ventilation - check phosphate in all difficult weaning cases
- Cardiac arrhythmias - ECG changes, VF risk in hypokalemia + hypomagnesemia; treat before induction
- Post-op ICU patients - initiate early enteral nutrition cautiously at low caloric targets; monitor electrolytes daily
Key Points to Remember for the Exam
- Hallmark electrolyte = Hypophosphatemia
- Mechanism = Insulin surge → intracellular shift of phosphate, potassium, magnesium
- Always give thiamine before glucose/feeds in at-risk patients
- Start feeds at 10 kcal/kg/day, increase over 4-7 days
- Wernicke's encephalopathy is a direct complication of thiamine depletion in refeeding
- Can occur with oral, enteral, or parenteral nutrition equally
References (Standard Textbooks):
- Bailey & Love's Short Practice of Surgery, 28e - Ch. 25, Summary Box 25.5
- Schwartz's Principles of Surgery, 11e - Ch. 3 (Malnourished Patients)
- Sabiston Textbook of Surgery (latest ed.) - Ch. Nutritional Support
- Yamada's Textbook of Gastroenterology, 7e - Ch. 23
- Tietz Textbook of Laboratory Medicine, 7e - Box 46.7
- Barash: Clinical Anesthesia, 9e (hypophosphatemia/electrolytes chapter)
Recent Evidence: A 2025 systematic review (PMID: 39187889) identified the strongest risk factors in adults as low BMI, prolonged fasting, and pre-existing electrolyte deficits - consistent with NICE criteria above. A 2026 systematic review (PMID: 41793849) specifically addresses risk prediction models in critically ill adults, relevant to ICU anaesthesia practice.
This is a shared conversation. Sign in to Orris to start your own chat.