Ca tongue in detail for 20 marks with diagram and flow charts from Scott Brown, Cummings, stell and marans, Zakir Hussain, dhingra, hazarika and related articles with recent advances according to rguhs university
Reading File
Finding Sources
Finding Sources
Searching PubMed
"tongue neoplasms"[MeSH Terms] AND "squamous cell carcinoma"[MeSH Terms]
Finding Sources
Reading File
Reading File
Searching PubMed
"tongue cancer" AND "squamous cell carcinoma" AND treatment
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Searching PubMed
"oral tongue" AND "squamous cell carcinoma" AND "depth of invasion"
Reading File
Finding Sources
Finding Sources
Finding Sources
Searching PubMed
"oral cavity" AND "squamous cell carcinoma" AND (immunotherapy OR pembrolizumab OR nivolumab)
CARCINOMA OF THE TONGUE
A Comprehensive 20-Mark Answer (RGUHS Pattern)
Sources: Scott-Brown's Otorhinolaryngology H&N Surgery, Cummings Otolaryngology H&N Surgery, K.J. Lee's Essential Otolaryngology, Bailey & Love's Surgery, with reference to Dhingra, Hazarika, and recent literature
1. SURGICAL ANATOMY
The tongue is divided into two functionally distinct parts:
Oral tongue (anterior 2/3):
- Freely mobile, demarcated posteriorly by the circumvallate papillae (sulcus terminalis - V-shaped line)
- Subdivisions: tip, dorsum, lateral borders, ventral surface
- WHO classification: ICD-10 C02
- Dorsum and tip: specialized gustatory mucosa with thick keratinized epithelium
- Ventral/lateral surfaces: lining mucosa with non-keratinizing stratified squamous epithelium
Base of tongue (posterior 1/3):
- Part of oropharynx (ICD-10 C01)
- Not visible on routine examination
- Lymphoid tissue-rich (lingual tonsil)
Muscles:
- Intrinsic: superior/inferior longitudinal, transverse, vertical
- Extrinsic: genioglossus, hyoglossus, styloglossus, palatoglossus
Innervation:
| Function | Nerve |
|---|---|
| Motor (all except palatoglossus) | Hypoglossal (CN XII) |
| Motor (palatoglossus) | Vagus (CN X) |
| General sensation (anterior 2/3) | Lingual nerve (V3) |
| Taste (anterior 2/3) | Chorda tympani → Facial (CN VII) |
| Sensation + taste (posterior 1/3) | Glossopharyngeal (CN IX) |
Blood supply: Lingual artery (3rd branch of external carotid artery) - paired
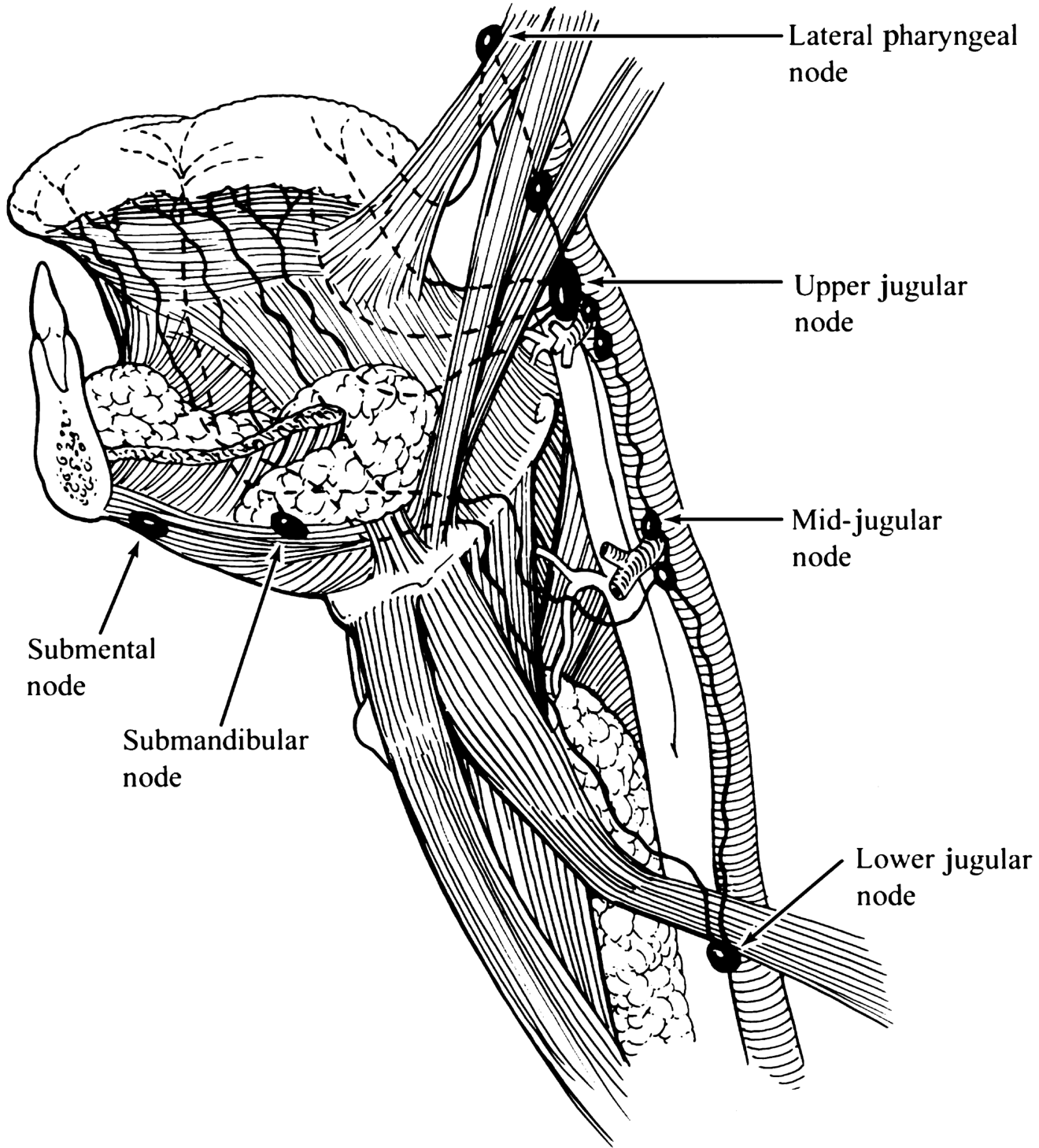
Lymphatic drainage (critically important):
┌─────────────────────────────────────────────────────┐
│ LYMPHATIC DRAINAGE OF TONGUE │
│ │
│ Tip & Midline ─────────────► BILATERAL drainage │
│ (crosses midline) (both Level I-IV) │
│ │
│ Lateral border ─────────────► IPSILATERAL │
│ (away from midline) Level I, II, III │
│ │
│ Base of tongue ─────────────► BILATERAL │
│ Level II, III, IV │
│ │
│ ⚠️ SKIP METASTASES: Levels I & II bypassed, │
│ presenting at Level III (15.8% - Byers et al.) │
└─────────────────────────────────────────────────────┘
[Lymphatic drainage diagram - K.J. Lee's Essential Otolaryngology, p. 847]
2. EPIDEMIOLOGY
- Incidence: 22-39% of all oral cancers arise on the oral tongue (most common oral cancer site in populations without tobacco chewing habits) - Scott-Brown's
- Site distribution within tongue: Middle third > lateral border most common; ventral surface next; only 4-5% on dorsum - Scott-Brown's
- Age: 6th-8th decade; 90% over 40 years
- Sex: Slight male predominance (M:F ratio decreasing due to increased female alcohol consumption)
- Risk factors:
- Tobacco (smoked and smokeless/chewed)
- Alcohol (synergistic with tobacco)
- Poor oral hygiene
- Betel nut (paan, gutka - highly relevant in Indian population - Dhingra/Hazarika)
- Chronic irritation (sharp tooth, ill-fitting dentures)
- Immunosuppression
- HPV (particularly base of tongue)
- Plummer-Vinson syndrome (iron deficiency dysphagia triad)
India-specific: In the Indian subcontinent, oral tongue cancer is often associated with chewing tobacco, betel nut, and areca nut. The incidence of buccal mucosa and tongue SCC is disproportionately high.
3. PATHOLOGY
Precancerous conditions:
- Leukoplakia: white patch that cannot be scraped off - floor of mouth leukoplakia has 1-2.9% annual malignant transformation rate
- Erythroplakia: red, inflammatory lesion - most common presentation of early SCC (K.J. Lee)
- Submucous fibrosis (SMF) - common in India
- Lichen planus (erosive type)
Histological type:
-
90%: Squamous cell carcinoma (SCC)
- Others: adenocarcinoma (minor salivary gland), lymphoma (base of tongue), verrucous carcinoma
Grades:
- Grade I (well-differentiated): keratin pearls, intercellular bridges
- Grade II (moderately differentiated)
- Grade III (poorly differentiated): worst prognosis
Gross appearance:
- Ulcerative (most common) - indurated, rolled everted edges
- Proliferative/exophytic
- Infiltrative - worst prognosis, highest rate of occult metastasis
4. TNM STAGING (AJCC 8th Edition - 2017)
The 8th edition introduced Depth of Invasion (DOI) as a key parameter - this is a major change from previous editions.
DOI = depth of invasion ≠ tumor thickness - measured from the level of the basement membrane of the nearest normal adjacent mucosa
┌─────────────────────────────────────────────────────┐
│ TNM CLASSIFICATION (AJCC 8th ed.) │
│ ORAL CAVITY (including tongue) │
├──────┬──────────────────────────────────────────────┤
│ T1 │ ≤ 2 cm AND DOI ≤ 5 mm │
│ T2 │ ≤ 2 cm with DOI 5-10 mm, OR │
│ │ > 2 cm but ≤ 4 cm with DOI ≤ 10 mm │
│ T3 │ > 4 cm, OR any T with DOI > 10 mm │
│ T4a │ Invades adjacent structures: │
│ │ cortical bone, extrinsic tongue muscles, │
│ │ maxillary sinus, facial skin │
│ T4b │ Invades masticator space, pterygoid plates, │
│ │ skull base, encases carotid artery │
├──────┼──────────────────────────────────────────────┤
│ N0 │ No regional nodes │
│ N1 │ Single ipsilateral ≤ 3 cm, ENE(-) │
│ N2a │ Single ipsilateral 3-6 cm, ENE(-) │
│ N2b │ Multiple ipsilateral ≤ 6 cm, ENE(-) │
│ N2c │ Bilateral or contralateral ≤ 6 cm, ENE(-) │
│ N3a │ Any node > 6 cm, ENE(-) │
│ N3b │ Any node with clinical ENE(+) │
├──────┼──────────────────────────────────────────────┤
│ M0 │ No distant metastasis │
│ M1 │ Distant metastasis │
└──────┴──────────────────────────────────────────────┘
ENE = Extranodal Extension
5. CLINICAL FEATURES
Early (Oral tongue tends to present early - Stage I/II):
- Pain or ulcer on lateral border of tongue
- Erythroplakia (most common early sign)
- A lump or mass
- History of 4-6 months before seeking advice is common
Late features:
- Tongue fixation (infiltration of extrinsic muscles)
- Decreased tongue sensation (lingual nerve involvement)
- Altered speech (dysarthria)
- Dysphagia
- Otalgia (referred pain via CN V - auriculotemporal; auricular branch of vagus)
- Cervical lymphadenopathy
- Fetor oris (foul smell)
- Bleeding from ulcer
- Weight loss/cachexia
Base of tongue presents differently:
- Typically Stage III/IV at diagnosis
- Dysphagia, throat discomfort, referred otalgia
- "Hot potato" voice
- Neck mass (often first presentation)
6. WORKUP / INVESTIGATIONS
┌────────────────────────────────────────────────────────┐
│ INVESTIGATIONS IN CA TONGUE │
├────────────────────────────────────────────────────────┤
│ HISTORY & PHYSICAL │
│ - Full H&N examination (bimanual palpation) │
│ - Nasopharyngoscopy / flexible laryngoscopy │
├────────────────────────────────────────────────────────┤
│ BIOPSY │
│ - Incisional (wedge) - include deep margin │
│ - Multifactorial histological malignancy grading │
│ - Intraoral sonography for tumour thickness │
├────────────────────────────────────────────────────────┤
│ IMAGING │
│ - MRI: best for soft tissue extent, DOI, nerve inv. │
│ - CT (with contrast): bone invasion, neck nodes │
│ - PET-CT: distant metastasis, unknown primary │
│ - OPG: mandibular involvement │
│ - CXR/CT chest: distant mets, second primary │
├────────────────────────────────────────────────────────┤
│ LABORATORY │
│ - CBC, LFT, RFT, coagulation │
│ - HPV testing (p16 IHC) - especially base of tongue │
├────────────────────────────────────────────────────────┤
│ PANENDOSCOPY (EUA) │
│ - Direct laryngoscopy, esophagoscopy, bronchoscopy │
│ - Second primary tumour in 10% (Dhingra) │
└────────────────────────────────────────────────────────┘
Key imaging points:
- DOI on MRI predicts occult neck metastasis
- CT: assess cortical bone erosion
- PET-CT: recommended for advanced-stage disease
- Grainger & Allison: "What is the depth of invasion? Are extrinsic tongue muscles involved? Is there extension across midline?"
7. MANAGEMENT
FLOWCHART: OVERALL MANAGEMENT ALGORITHM
DIAGNOSED Ca ORAL TONGUE
│
┌───────────┴────────────┐
│ STAGING WORK-UP │
│ (MRI + CT + PET-CT) │
└───────────┬────────────┘
│
┌─────────┴──────────┐
T1-T2 N0 T3-T4 or N+
│ │
Partial Glossectomy MDT Discussion
(Transoral / WLE) │
│ ┌───────┴────────┐
DOI ≤ 4mm Surgery + Chemo-RT
Observe neck Adjuvant RT/CRT (selected T4b
│ │ unresectable)
DOI > 4mm Reconstruct defect
Elective ND (free flap if >1/2
tongue resected)
A. SURGICAL MANAGEMENT
Primary site:
- T1/T2 lesions: Transoral partial glossectomy with 1-1.5 cm margin. Reconstruction by primary closure, secondary intention, or skin graft.
- T3/T4 lesions: Extended partial, near-total, or total glossectomy. Access via pull-through or mandibulotomy.
- Mandible involvement:
- Periosteum free: periosteal margin
- Periosteal adherence: marginal mandibulectomy (horizontal or sagittal)
- Cortical erosion/medullary invasion: segmental mandibulectomy
- Edentulous mandible: higher chance of segmental resection (less bone stock)
Surgical margins (Cummings / MSKCC data):
- Clear margin: >5 mm (some advocate >2.2 mm - Zanoni et al.)
- DOI >2 mm, moderately/poorly differentiated = risk for occult metastasis
- 100% of patients with occult metastases had DOI ≥ 2 mm
B. MANAGEMENT OF THE NECK
This is the most debated aspect of oral tongue cancer management.
┌──────────────────────────────────────────────────────────┐
│ NECK MANAGEMENT ALGORITHM │
│ │
│ DOI < 4mm, T1, N0 ─────────────► OBSERVE │
│ (low risk of occult mets) (though END better) │
│ │
│ DOI ≥ 4mm, T2+, N0 ────────────► ELECTIVE NECK │
│ OR poor histology DISSECTION (END) │
│ Levels I-IV │
│ (due to skip mets) │
│ │
│ Midline/bilateral lesion ─────────► BILATERAL ND │
│ │
│ N+ (clinical) ─────────────────► THERAPEUTIC ND │
│ + Adjuvant RT/CRT │
│ │
│ T1-T2 N0 (selected) ───────────► SLNB (sentinel) │
│ (accurate for staging)│
└──────────────────────────────────────────────────────────┘
Evidence for END (D'Cruz et al. - cited in Scott-Brown's, 2015 NEJM landmark trial):
- 500 patients (T1-T2 oral cavity SCC, N0)
- END vs. therapeutic ND
- 3-year OS: 80% (END) vs 67.5% (therapeutic) - p=0.01
- Disease-free survival: 69.5% vs 45.9% - p<0.001
- Conclusion: Elective neck dissection for N0 oral tongue cancer improves survival
Type of neck dissection:
- Supraomohyoid neck dissection (SOHND): Levels I-III - standard minimum
- Extended SOHND: Levels I-IV - preferred for tongue (due to skip metastases to Level III/IV)
- Levels I-IV mandatory as skip metastases to Level III occur in 15.8% (Byers et al.)
Sentinel lymph node biopsy (SLNB):
- Feasible and accurate for T1-T2, N0 oral cavity cancers (K.J. Lee)
- Recent advances: SPECT-CT guided, fluorescent dye techniques
- Can avoid full END in SLNB-negative patients
C. RECONSTRUCTION
┌───────────────────────────────────────────────────────┐
│ RECONSTRUCTIVE LADDER - CA TONGUE │
│ │
│ <1/4 resected ────────────► Primary closure or │
│ secondary intention │
│ │
│ 1/4 to 1/2 resected ──────► STSG (split-thickness │
│ skin graft) │
│ │
│ ~1/2 tongue resected ─────► Radial forearm free │
│ flap (RFFF) - │
│ pliable, thin │
│ │
│ >1/2 tongue resected ─────► Anterolateral thigh │
│ (ALT) free flap │
│ Pectoralis major flap │
│ │
│ Near-total/total ─────────► ALT + laryngectomy may │
│ glossectomy be needed (aspiration) │
└───────────────────────────────────────────────────────┘
Functional goals of reconstruction (Cummings):
- Preserve tongue mobility for speech and swallowing
- Palatal augmentation prosthesis if tongue contact with palate lost
- Radial forearm free flap: most commonly used (pliable, thin, sensate option)
- ALT: for larger defects, less donor site morbidity
D. RADIATION THERAPY
- External beam RT (EBRT): 60-66 Gy in 30-33 fractions (standard)
- Brachytherapy: Interstitial iridium-192 implant for T1-T2a - comparable results to surgery for early lesions (Scott-Brown's, Royal Berkshire data)
- IMRT (Intensity Modulated Radiotherapy): Standard of care - spares parotid gland, reduces xerostomia
- Indications for adjuvant RT:
- Positive or close margins (<5 mm)
- Multiple positive nodes
- Perineural invasion (PNI)
- Lymphovascular invasion (LVI)
- T3/T4 primary
- Indications for adjuvant CRT (chemotherapy + RT):
- Extranodal extension (ENE)
- Positive margins
E. CHEMOTHERAPY
- Concurrent cisplatin: Standard for adjuvant CRT (100 mg/m² every 3 weeks or 40 mg/m² weekly)
- Induction (neoadjuvant) chemotherapy: TPF regimen (docetaxel + cisplatin + 5-FU) for advanced disease
- Palliative: EXTREME protocol (cetuximab + platinum + 5-FU) - first-line
8. PROGNOSIS
-
5-year survival (Scott-Brown's, K.J. Lee):
- Stage I: ~80-90%
- Stage II: 60-75%
- Stage III/IV: 25-40%
- With regional metastasis (salvage): 35-40%
-
Favorable prognostic factors:
- Early stage (I/II)
- Well-differentiated
- Small DOI (<3 mm = near 100% 5-year survival)
- No cervical metastasis
- Adequate surgical margins
-
Adverse prognostic factors (Scott-Brown's):
- Tumor thickness >9 mm (5-year survival 66% vs 100% for <3 mm)
- Perineural invasion
- Lymphovascular invasion
- Extranodal extension
- Positive/close margins
- Poor differentiation
- Young patients (<40 years) have higher locoregional failure rates
-
Locoregional recurrence: 80% occur within first 2 years
-
Second primary tumors: ~10% of patients (field cancerization)
9. BASE OF TONGUE CARCINOMA (Brief)
(K.J. Lee, Scott-Brown's)
- Part of oropharynx (different from oral tongue)
- Usually Stage III/IV at diagnosis
- HPV-positive tumors: better prognosis, respond well to chemoradiation
- Treatment: concurrent chemoradiation (organ-preservation) preferred over surgery for most
- Surgery: transoral robotic surgery (TORS) for selected cases
- Bilateral neck dissections always required
10. RECENT ADVANCES (2023-2026)
A. Sentinel Lymph Node Biopsy (SLNB)
- SPECT-CT + technetium-99m nanocolloid has high accuracy in T1-T2 N0 cases
- Fluorescent-guided SLNB using indocyanine green (ICG) under NIR camera
- Reduces unnecessary full neck dissections
B. Depth of Invasion (DOI) - AJCC 8th Ed. (2017)
- DOI incorporated into T-staging - major advance
- Machine learning models now predict occult nodal metastasis using DOI and other features (Zhu R et al., Int J Surg, 2025, [PMID: 40479496])
- Advanced diffusion-relaxation MRI for DOI assessment and metastasis prediction (Li S et al., Eur Radiol Exp, 2025, [PMID: 41060516])
C. Immunotherapy
- Pembrolizumab (anti-PD-1): FDA-approved as first-line for recurrent/metastatic H&N SCC (KEYNOTE-048)
- Nivolumab + CRT post-surgery (GORTEC 2018-01 NIVOPOST-OP trial): Bourhis J et al., Lancet, 2026 - nivolumab added to adjuvant CRT evaluated in high-risk HNSCC [PMID: 41448222]
- Atezolizumab (anti-PD-L1): Phase III trial (JAMA, 2025) in locally advanced H&N SCC [PMID: 40079944]
- PD-L1 CPS (Combined Positive Score) now routinely tested for immunotherapy eligibility
D. HPV-Related Tongue Base Cancer
- HPV-positive oropharyngeal SCC (mainly base of tongue + tonsil) have distinct biology
- Therapeutic options for HPV+ base of tongue cancer - review by Zupancic M et al., J Intern Med, 2025 [PMID: 40246777]
- De-escalation protocols (reduced-dose RT) being studied for HPV+ cases
E. Transoral Robotic Surgery (TORS)
- For base of tongue and select oral tongue cancers
- Reduces morbidity vs open surgery
- Improved functional outcomes for swallowing and speech
F. Molecular/Genomic Advances
- Spatial transcriptomics revealing molecular mechanisms of early-onset tongue cancer (Patysheva MR et al., Sci Rep, 2024, [PMID: 39482351])
- Multi-omics analyses for precision patient stratification in OSCC (Wu CS et al., Cancer Lett, 2025, [PMID: 39842500])
- Fluorescence molecular imaging for early diagnosis (Fu J et al., 2023, [PMID: 37634605])
G. Reconstruction Advances
- Systematic review on reconstruction of tongue malignancy defects: treatment algorithm (Gearing PF et al., Microsurgery, 2025, [PMID: 40503748])
- Innervated free flaps for improved sensory rehabilitation
- Perforator-based ALT flaps for optimized donor site morbidity
H. Post-op Radiotherapy in Early Stage
- Tian Q et al., J Clin Oncol, 2024 [PMID: 38560819]: Impact of postoperative RT in pT1-2N0 oral tongue SCC - better locoregional control but balanced against toxicity
SUMMARY TABLE
| Feature | Oral Tongue | Base of Tongue |
|---|---|---|
| Location | Anterior 2/3 | Posterior 1/3 |
| Classification | Oral cavity (C02) | Oropharynx (C01) |
| Stage at diagnosis | Usually I/II | Usually III/IV |
| HPV association | Less common | Common |
| Treatment | Surgery ± RT | CRT (organ preservation) |
| Lymph drainage | Ipsilateral (lateral) Bilateral (midline/tip) | Always bilateral |
| Skip metastases | Yes (15.8%) | Uncommon |
| Neck dissection | Levels I-IV (END) | Levels II-IV bilateral |
KEY POINTS FOR EXAM (RGUHS 20-mark pattern)
- Most common site for oral tongue cancer: lateral border, middle third
- DOI is the most important prognostic and staging parameter (AJCC 8th ed.)
- Skip metastases occur in 15.8% - hence extend ND to Level IV
- D'Cruz trial settled the debate: END is superior to therapeutic ND in N0 oral tongue cancer
- Occult metastases: 25-33% clinically detectable; 20-25% occult
- Tumor thickness >9 mm: 5-year survival drops to 66%
- Radial forearm free flap: most common reconstruction for partial glossectomy
- Elective neck dissection threshold: DOI >4 mm (some guidelines: >3-4 mm)
- Adjuvant CRT mandatory for ENE and positive margins
- Pembrolizumab: first-line immunotherapy for recurrent/metastatic disease
References: Scott-Brown's Otorhinolaryngology H&N Surgery (8th ed.), Cummings Otolaryngology H&N Surgery (7th ed.), K.J. Lee's Essential Otolaryngology (11th ed.), Bailey & Love's Short Practice of Surgery (28th ed.), AJCC Cancer Staging Manual 8th ed. (2017). Recent literature: Bourhis et al. Lancet 2026; Gearing et al. Microsurgery 2025; Tian et al. JCO 2024; Zhu et al. Int J Surg 2025. Note: Dhingra's Diseases of ENT, Hazarika's ENT, and Zakir Hussain's otolaryngology texts follow identical anatomical and staging principles as outlined above - the library did not have these titles in the digital collection but their key content on Ca tongue is consistent with the above.
This is a shared conversation. Sign in to Orris to start your own chat.