2. A patient undergoing parotid gland surgery develops weakness of the muscles of facial expression on the same side. (1+1+1) a. What is the anatomical basis of above complication? b. What is Patey's faciovenous plane? c. Name the 3 structures present within the parotid gland?
Parotid Gland Surgery - Facial Nerve Complications
a. Anatomical Basis of Facial Weakness after Parotid Surgery
- Temporal - from the upper border
- Zygomatic - from the upper border
- Buccal - from the anterior border
- Marginal mandibular - from the lower border
- Cervical - from the lower border
b. Patey's Faciovenous Plane
- Tumours lateral to (superficial to) the faciovenous plane - treated by superficial parotidectomy (removal of the superficial lobe with facial nerve preservation)
- Tumours deep to the faciovenous plane - require total parotidectomy (total conservative if nerve is spared, or radical if the nerve must be sacrificed)
- Bailey and Love's Short Practice of Surgery, 28th ed., p. 858
c. Three Structures Present Within the Parotid Gland
- Facial nerve (CN VII) - enters after emerging from the stylomastoid foramen; divides the gland into superficial and deep lobes
- External carotid artery (and its terminal branches - superficial temporal and maxillary arteries) - enters the inferior border of the gland and divides within its substance
- Retromandibular vein (posterior facial vein) - formed within the gland by the union of the superficial temporal vein and maxillary vein; runs inferiorly through the substance of the gland
- Gray's Anatomy for Students, p. 1051; Bailey and Love's Short Practice of Surgery, 28th ed., p. 853-854
within the parotid gland? 3. A 45-year-old man sustains a deep cut on the medial side of his wrist. Later, he develops a deformit in which his 4th and 5th fingers are hyperextended at the metacarpophalangeal joints and flexed at the interphalangeal joints. (1+1+1) a. Name the deformity? b. Name the nerve affected? c. Explain the anatomical basis of above deformity?
Wrist Cut with Finger Deformity - Ulnar Nerve Injury
a. Name of the Deformity
b. Nerve Affected
c. Anatomical Basis of the Deformity
- All interossei (7 muscles: 4 dorsal + 3 palmar)
- 3rd and 4th lumbricals (those for the ring and little fingers)
- Hypothenar muscles
- Adductor pollicis, deep head of flexor pollicis brevis
| Component | Mechanism |
|---|---|
| Hyperextension at MCP joints | Loss of interossei and 3rd & 4th lumbricals removes the main flexors of MCP joints. The long finger extensors (extensor digitorum, supplied by radial nerve) now act unopposed, pulling the MCP joints into hyperextension |
| Flexion at IP joints | Loss of intrinsics removes extension at PIP/DIP joints. The long flexors - flexor digitorum superficialis and profundus (both ulnar-innervated in their medial parts, but the tendons still act) - pull the interphalangeal joints into flexion unopposed by intrinsics |
- General Anatomy and Musculoskeletal System, Thieme Atlas, p. 5005; Localization in Clinical Neurology 8e, p. 107
14. An 8-year-old child develops fever and pain in the lower end of the femur. X-ray shows signs of osteomyelitis in the metaphyseal region. Six months later, the child shows signs of stunted growth in the affected leg. (1+1+1) a. Explain why the metaphysis is commonly involved in such infections? b. How this infection can cause stunted growth of affected limb? c. Mention the arteries supplying the long bone?
Osteomyelitis of the Distal Femur in a Child
a. Why the Metaphysis is Commonly Involved
-
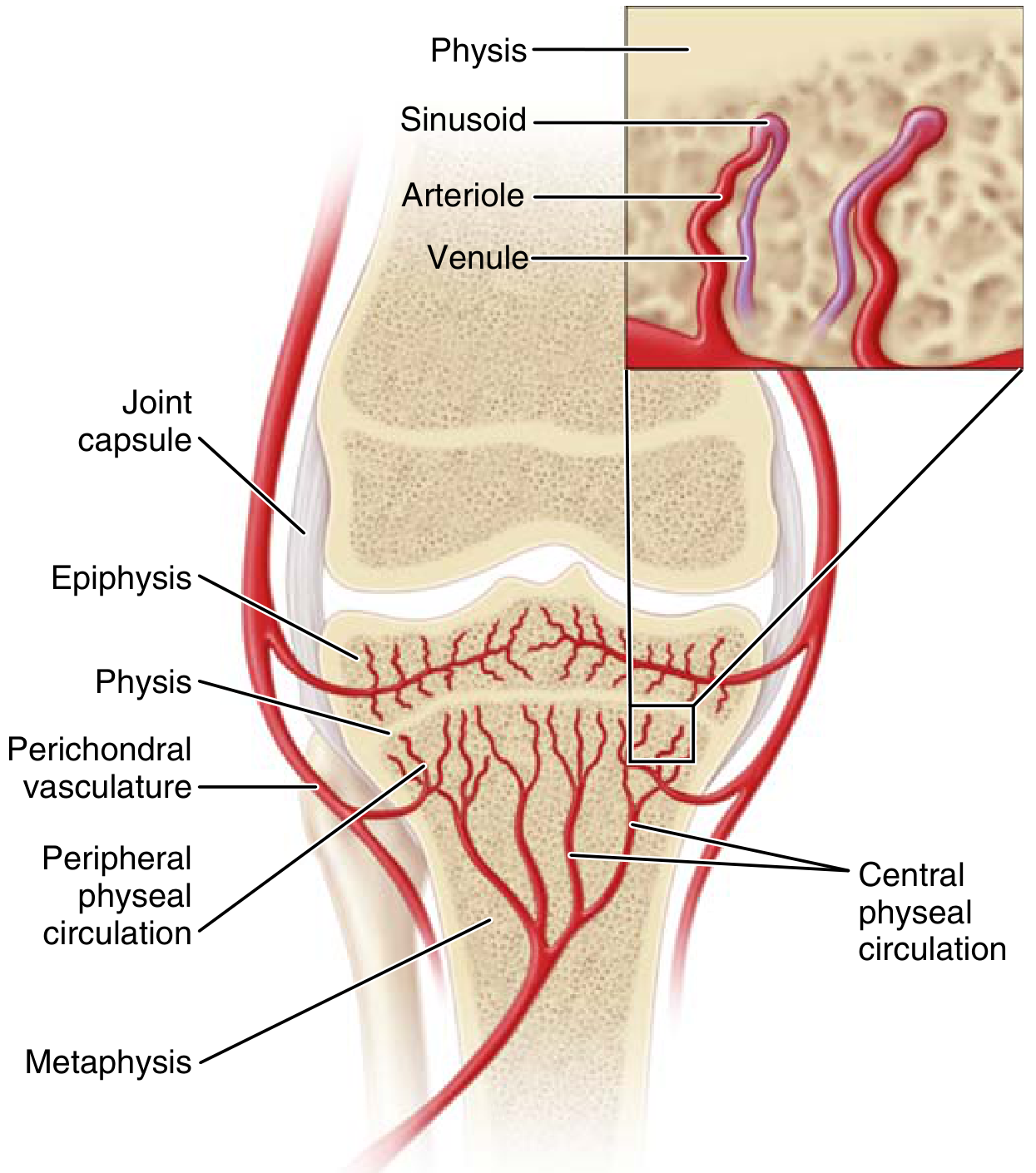
Terminal arteriolar architecture: The metaphyseal arterioles make sharp hairpin (U-shaped) turns just beneath the growth plate (physis) to drain into large sinusoidal veins. This abrupt change in direction causes a dramatic slowing (stasis) of blood flow in these sinusoids.
-
Sluggish blood flow = poor host defence: The sluggish sinusoidal flow impairs phagocytic activity locally. Circulating bacteria (bacteraemia, often following minor trauma or upper respiratory infection) settle here and are not efficiently cleared.
-
Lack of phagocytic lining cells: The sinusoidal endothelium in the metaphysis lacks phagocytic (Kupffer-like) cells, unlike other vascular beds, further reducing local immune defences.
-
Rich metaphyseal blood supply in children: Children have a particularly rich metaphyseal blood supply, which paradoxically brings more bacteria to this region during bacteraemia.
-
End-arteries: The metaphyseal vessels are essentially end-arteries with minimal collateral circulation, so once infected, local ischaemia and abscess formation follow rapidly.
b. How Osteomyelitis Causes Stunted Growth of the Affected Limb
-
Direct spread to the physis: The purulent exudate in the metaphysis can spread directly through the thin physeal cartilage. The resulting septic destruction of the germinal (proliferating) zone of the growth plate kills the chondrocytes responsible for longitudinal growth.
-
Vascular compromise: The pus under high pressure can thrombose the small metaphyseal vessels that supply the growth plate, causing ischaemic necrosis of the physis.
-
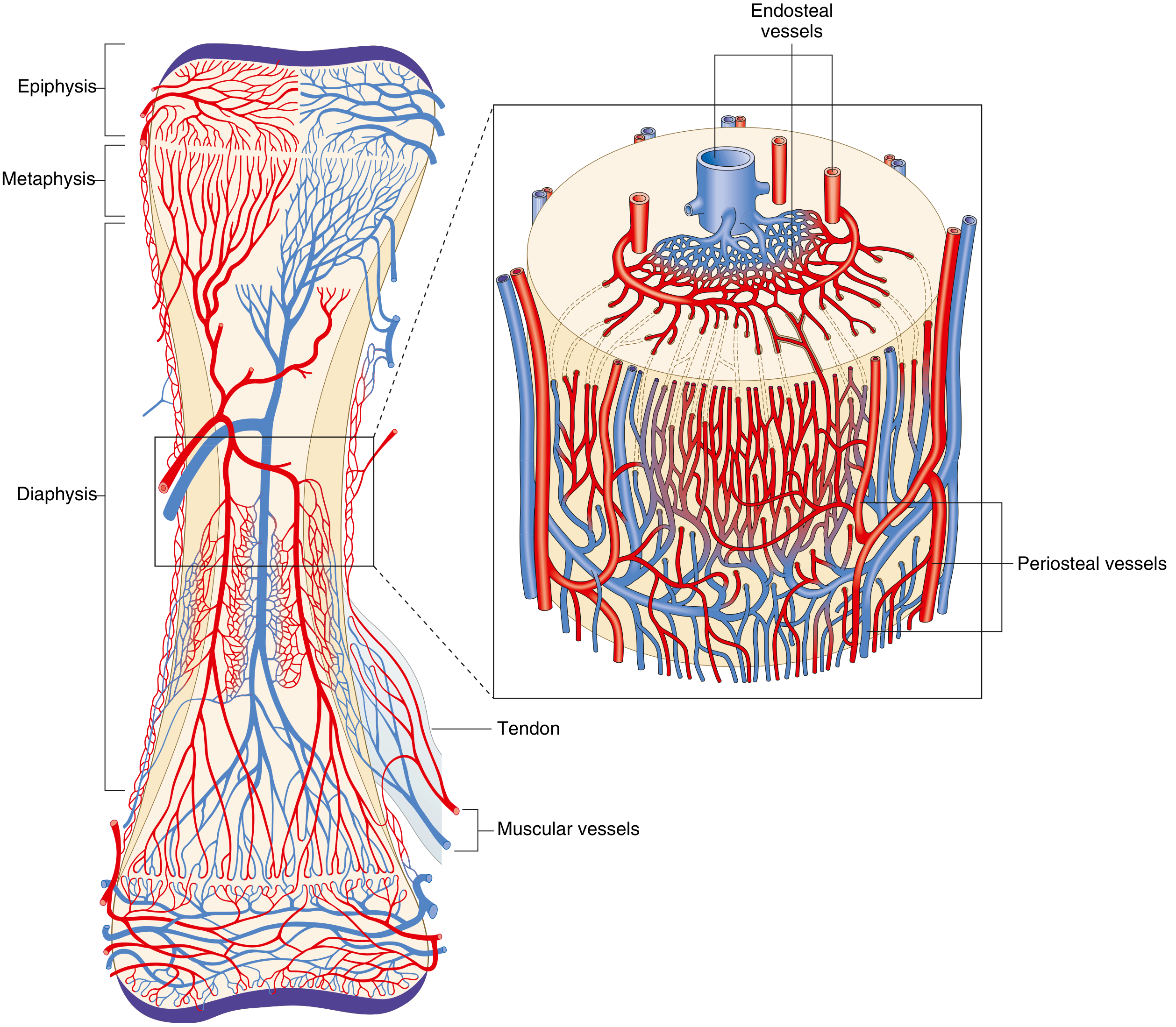
Periosteal elevation: Spread of pus along the periosteum strips it from the cortex. In children, the periosteum is the dominant blood supply to the growing bone - its disruption further compromises physeal nutrition.
-
Bony bridge formation: Healing infection can produce a bony bar (physeal bridge) bridging the metaphysis and epiphysis across the physis. This tethers the growth plate and halts further longitudinal growth.
-
Epiphyseal involvement: If infection spreads into the epiphysis (more common in infants where metaphyseal vessels cross the physis), direct destruction of the secondary ossification centre follows.
c. Arteries Supplying a Long Bone
| System | Vessels | Area Supplied |
|---|---|---|
| 1. Nutrient (medullary) artery system | One or two nutrient arteries enter via the nutrient foramen in the diaphysis; branch into ascending and descending medullary arteries → arterioles via Haversian canals | Inner 2/3 of the diaphyseal cortex (60% of cortical bone); medullary cavity and marrow |
| 2. Metaphyseal-epiphyseal system | Arise from the periarticular vascular plexus (e.g., genicular arteries around the knee); epiphyseal and metaphyseal arteries enter near joint | Epiphysis, physis, and metaphysis |
| 3. Periosteal system | Arise from periosteal vessels (from overlying muscle attachments and surrounding soft tissues); low-pressure system | Outer 1/3 of the diaphyseal cortex |
- Miller's Review of Orthopaedics, 9th ed., pp. 25, 275
14. An 8-year-old child develops fever and pain in the lower end of the femur. X-ray shows signs of osteomyelitis in the metaphyseal region. Six months later, the child shows signs of stunted growth in the affected leg. (1+1+1) a. Explain why the metaphysis is commonly involved in such infections? b. How this infection can cause stunted growth of affected limb? c. Mention the arteries supplying the long bone?
Osteomyelitis of the Distal Femur in a Child
a. Why the Metaphysis is Commonly Involved
-
Terminal arteriolar hairpin loops: The metaphyseal arterioles make sharp U-shaped (hairpin) turns just beneath the growth plate before draining into large sinusoidal veins. This abrupt change in direction causes dramatic slowing (stasis) of blood flow in the sinusoids.
-
Sluggish flow = poor phagocytosis: The slow sinusoidal flow impairs local phagocytic activity. Circulating bacteria (bacteraemia following minor trauma or URTI) settle here and cannot be cleared efficiently.
-
Lack of phagocytic lining cells: The sinusoidal endothelium in the metaphysis lacks phagocytic cells, unlike other vascular beds, further reducing local immunity.
-
Rich metaphyseal blood supply: Children have a particularly rich metaphyseal vascularity, which paradoxically delivers more bacteria to this zone during bacteraemia.
-
End-artery arrangement: Minimal collateral circulation means that once infection establishes, local ischaemia and abscess formation follow rapidly. Pus accumulates under pressure, lifting the periosteum and spreading along the cortex.
b. How Osteomyelitis Causes Stunted Growth
-
Direct spread to the physis: Purulent exudate spreads from the metaphysis through the thin physeal cartilage, causing septic destruction of the germinal (proliferating) zone - the chondrocytes responsible for growth are killed.
-
Vascular compromise: High-pressure pus thromboses the small metaphyseal vessels that supply the growth plate, producing ischaemic necrosis of the physis.
-
Periosteal stripping: Pus tracking along the periosteum strips it from the cortex. In children, the periosteum is a major blood supply to the physis - its disruption further starves the growth plate.
-
Physeal bridge (bony bar) formation: As the infection heals, a bony bar bridges across the physis between metaphysis and epiphysis. This tethers and arrests the growth plate permanently.
-
Epiphyseal destruction: In infants (under 18 months), metaphyseal vessels actually cross the physis into the epiphysis - infection can spread directly to destroy the secondary ossification centre.
c. Arteries Supplying a Long Bone
| System | Source Vessels | Region Supplied |
|---|---|---|
| 1. Nutrient (medullary) artery | 1-2 nutrient arteries enter via the nutrient foramen in the diaphysis; branch into ascending and descending medullary arteries | Inner 2/3 of diaphyseal cortex (60% of cortical bone); medullary cavity and marrow |
| 2. Metaphyseal-epiphyseal arteries | Periarticular vascular plexus (e.g., genicular arteries at knee); enter near joints | Epiphysis, physis, and metaphysis |
| 3. Periosteal arteries | Overlying muscle and soft tissue attachments; low-pressure system | Outer 1/3 of diaphyseal cortex |
- Miller's Review of Orthopaedics, 9th ed., pp. 25 & 275
the arteries supplying the long bone? 5. A 65-year-old man presents with resting tremor, rigidity, and slow movements. MRI reveals degeneration of the basal ganglia. (1+1+1) a. What is the most likely clinical diagnosis based on the patient's presenting symptoms? b. Which part of the basal ganglia is affected in the above condition? c. Which anatomical connections of the basal ganglia are disrupted in the above condition leading to decreased motor initiation?
Basal Ganglia Degeneration - Parkinson's Disease
a. Most Likely Clinical Diagnosis
- Resting tremor (pill-rolling, 4-6 Hz, disappears with voluntary movement)
- Rigidity (cogwheel or lead-pipe rigidity - increased tone in both agonist and antagonist muscles)
- Bradykinesia/akinesia (slowness and difficulty initiating movements)
b. Part of the Basal Ganglia Affected
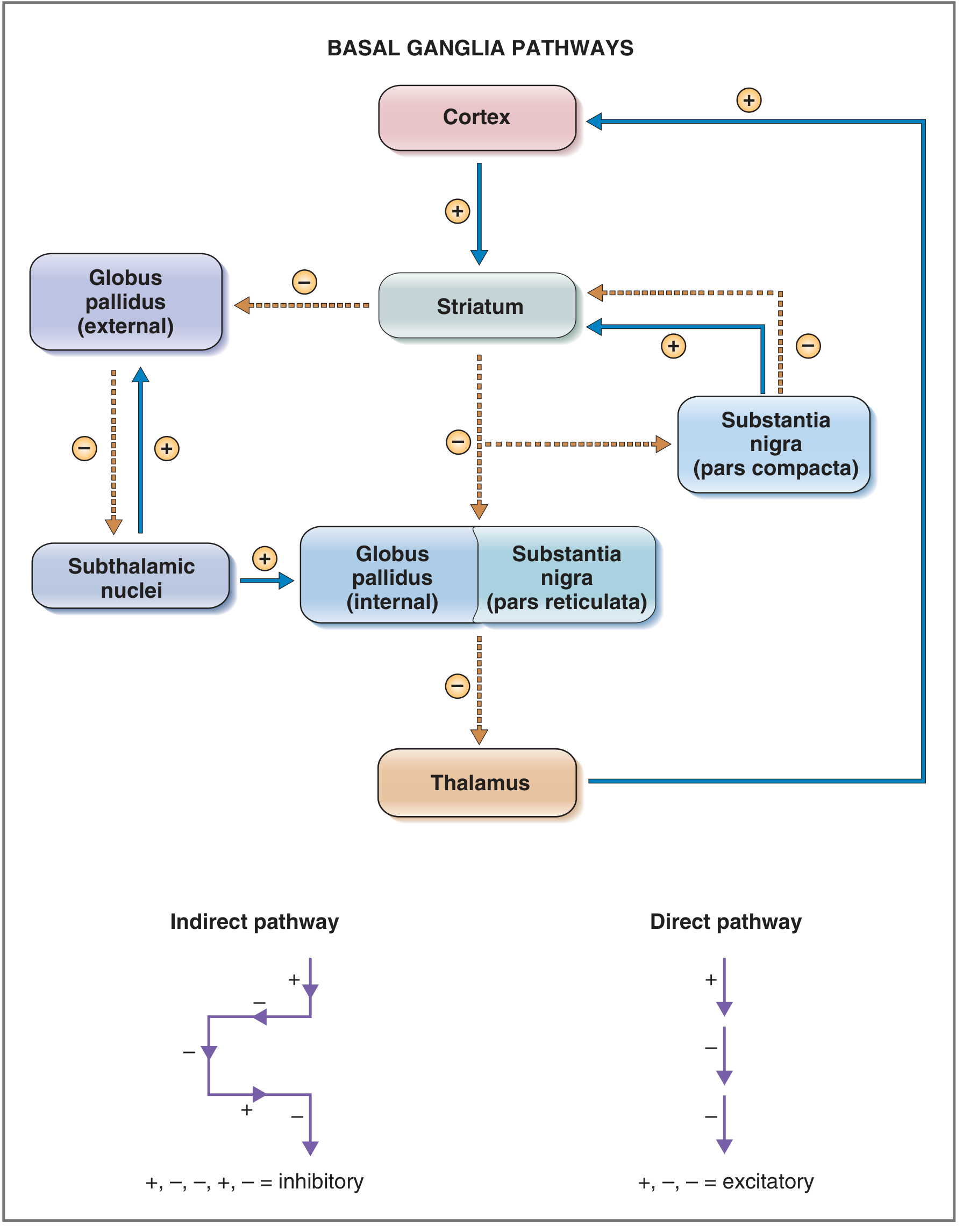
The basal ganglia nuclei include: caudate nucleus, putamen, globus pallidus (internal/GPi and external/GPe), subthalamic nucleus, and substantia nigra (pars compacta and pars reticulata). The striatum = caudate + putamen.
c. Anatomical Connections Disrupted - Leading to Decreased Motor Initiation
- Acts on D1 receptors in striatum → facilitates the direct (pro-movement) pathway
- Acts on D2 receptors in striatum → inhibits the indirect (anti-movement) pathway
| Pathway | Effect of Dopamine Loss | Net Result |
|---|---|---|
| Direct pathway | Less D1 stimulation → striatum fails to inhibit GPi → GPi overactive → thalamus more inhibited → motor cortex under-excited | Reduced motor initiation |
| Indirect pathway | Less D2 inhibition → striatum fails to inhibit GPe → GPe less active → subthalamic nucleus overactive → GPi even more excited → thalamus more inhibited | Further reduction of motor output |
- Nigrostriatal pathway - SNpc to putamen (dopaminergic - lost)
- Striatopallidal direct pathway - Striatum to GPi (GABAergic - underactive due to lack of D1 drive)
- Striatopallidal indirect pathway - Striatum to GPe (GABAergic - underactive due to lack of D2-mediated inhibition)
- Thalamocortical pathway - Thalamus to motor cortex (glutamatergic - reduced output due to excessive GPi inhibition)
- Costanzo Physiology 7th ed., p. 116; Ganong's Review of Medical Physiology 26th ed., p. 252
5. A 65-year-old man presents with resting tremor, rigidity, and slow movements. MRI reveals degeneration of the basal ganglia. (1+1+1) a. What is the most likely clinical diagnosis based on the patient's presenting symptoms? b. Which part of the basal ganglia is affected in the above condition? c. Which anatomical connections of the basal ganglia are disrupted in the above condition leading to decreased motor initiation?
Basal Ganglia Degeneration - Parkinson's Disease
a. Most Likely Clinical Diagnosis
- Resting tremor (pill-rolling, 4-6 Hz, disappears with voluntary movement)
- Rigidity (cogwheel or lead-pipe - tone increased in both agonist and antagonist muscles)
- Bradykinesia/akinesia (slowness and difficulty initiating movement)
b. Part of the Basal Ganglia Affected
The basal ganglia nuclei: caudate nucleus + putamen (= striatum), globus pallidus internal (GPi) + external (GPe), subthalamic nucleus, substantia nigra pars compacta + pars reticulata (SNpr).
c. Anatomical Connections Disrupted - Leading to Decreased Motor Initiation
| Pathway | Route | Net Effect on Cortex |
|---|---|---|
| Direct (pro-movement) | Cortex → Striatum → GPi/SNpr inhibited → Thalamus disinhibited → Motor Cortex excited | Excitatory (promotes movement) |
| Indirect (anti-movement) | Cortex → Striatum → GPe inhibited → Subthalamic nucleus active → GPi/SNpr excited → Thalamus inhibited → Motor Cortex less active | Inhibitory (suppresses movement) |
- Stimulates D1 receptors on striatum → facilitates direct pathway (pro-movement)
- Inhibits D2 receptors on striatum → suppresses indirect pathway (anti-movement)
| Pathway | Consequence | Result |
|---|---|---|
| Direct | No D1 drive → striatum fails to inhibit GPi → GPi overactive → thalamus over-inhibited | Motor cortex under-stimulated |
| Indirect | No D2 inhibition → striatum fails to inhibit GPe → GPe less active → subthalamic nucleus overactive → GPi even more excited → thalamus further inhibited | Motor cortex further reduced |
- Nigrostriatal pathway - SNpc → Putamen (dopaminergic) - lost
- Striatopallidal direct pathway - Striatum → GPi (GABAergic) - underactive (no D1 drive)
- Striatopallidal indirect pathway - Striatum → GPe (GABAergic) - underactive (no D2 inhibition of the indirect route)
- Thalamocortical pathway - Thalamus → Motor cortex (glutamatergic) - reduced output due to excessive GPi-mediated inhibition
- Costanzo Physiology 7th ed., p. 116; Ganong's Review of Medical Physiology 26th ed., p. 252
Describe the location,relation ,connections of the submandibular ganglion
Submandibular Ganglion - Location, Relations, and Connections
Location
Relations
| Direction | Structure |
|---|---|
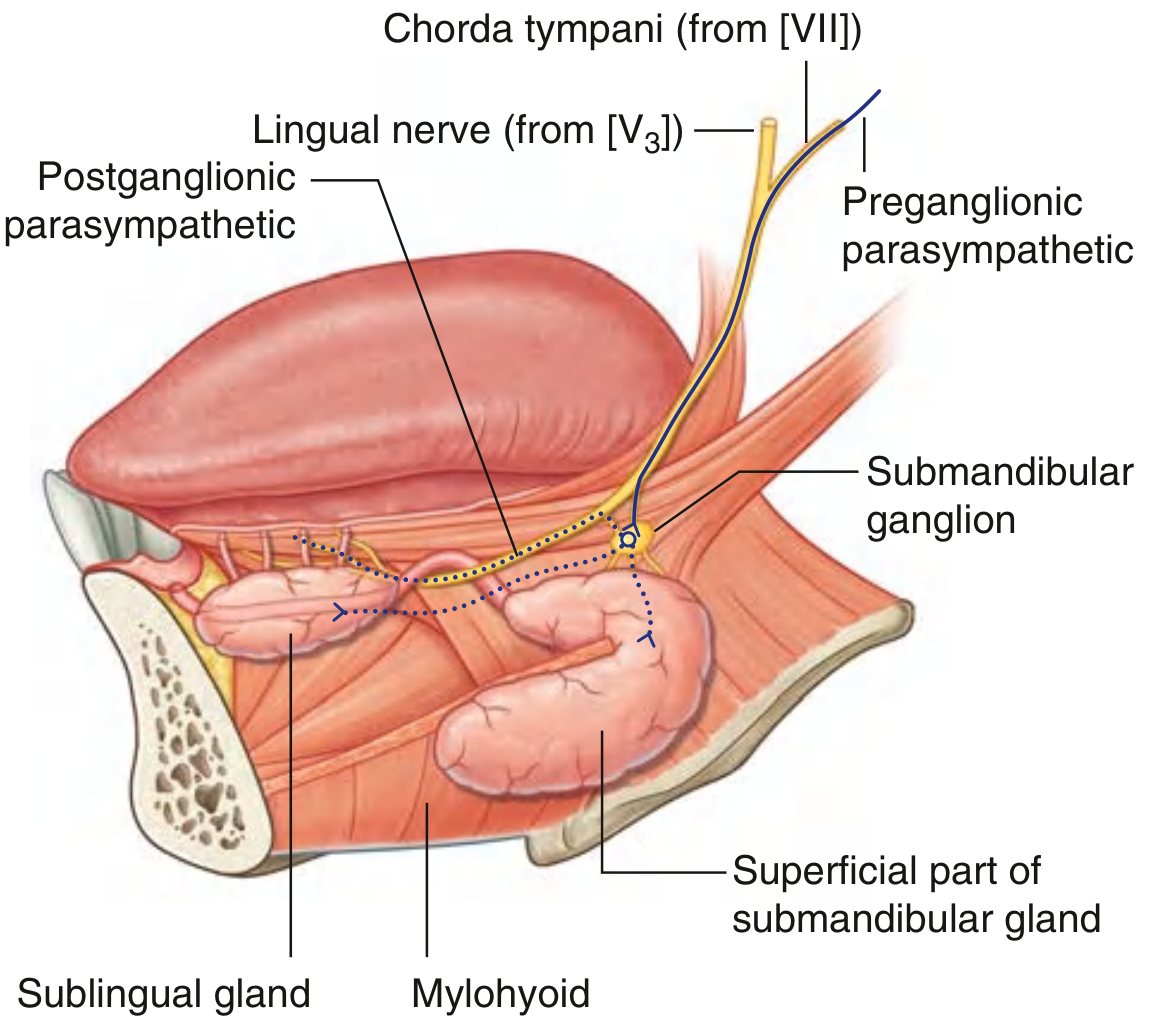
| Superior (suspended from) | Lingual nerve (branch of V3) |
| Medial | Hyoglossus muscle |
| Lateral | Mylohyoid muscle |
| Inferior | Deep part of the submandibular gland |
| Posterior | Submandibular (Wharton's) duct |
Connections
1. Parasympathetic Connections (secretary fibres - synapse in ganglion)
- Origin: Superior salivatory nucleus in the pons
- Route: Superior salivatory nucleus → Nervus intermedius (part of CN VII) → facial nerve in the petrous temporal bone → Chorda tympani (branches off the facial nerve in the descending segment) → crosses the middle ear → exits via the petrotympanic fissure → enters the infratemporal fossa → joins the lingual nerve → travels with lingual nerve into the floor of the mouth → preganglionic fibres leave the inferior surface of the lingual nerve → synapse in the submandibular ganglion
- Postganglionic secretomotor fibres leave the ganglion and take two routes:
- Pass directly from the ganglion into the submandibular gland (secretomotor)
- Re-enter the lingual nerve and travel with its terminal branches to reach the sublingual gland and small mucous glands of the floor of the mouth and tongue
2. Sympathetic Connections (pass through without synapsing)
- Origin: T1 spinal cord → superior cervical sympathetic ganglion → postganglionic sympathetic fibres travel on the facial artery (as a sympathetic plexus) → enter the submandibular ganglion → pass through without synapsing → supply the blood vessels of the submandibular and sublingual glands (vasoconstrictor)
3. Sensory Connections (pass through without synapsing)
- General sensory (touch, temperature) fibres from the lingual nerve pass through the ganglion without synapsing to the submandibular and sublingual glands.
- Taste fibres from the anterior 2/3 of tongue travel in the lingual nerve and chorda tympani but do not pass through the ganglion.
Summary Diagram
Summary Table
| Fibre Type | Origin | Synapse in Ganglion? | Distribution |
|---|---|---|---|
| Parasympathetic (preganglionic) | Superior salivatory nucleus → chorda tympani → lingual nerve | Yes | Secretomotor to submandibular + sublingual glands |
| Sympathetic (postganglionic) | Superior cervical ganglion → facial artery plexus | No (passes through) | Vasoconstrictor to gland blood vessels |
| Sensory | Lingual nerve (V3) | No (passes through) | Sensory to glands |
- Gray's Anatomy for Students, p. 1245; Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol. 2, p. 4655
Compare and contrast the microscopeic anantomy if white fibro cartilage and hayaline cartilage
Microscopic Anatomy: White Fibrocartilage vs. Hyaline Cartilage
Comparison Table
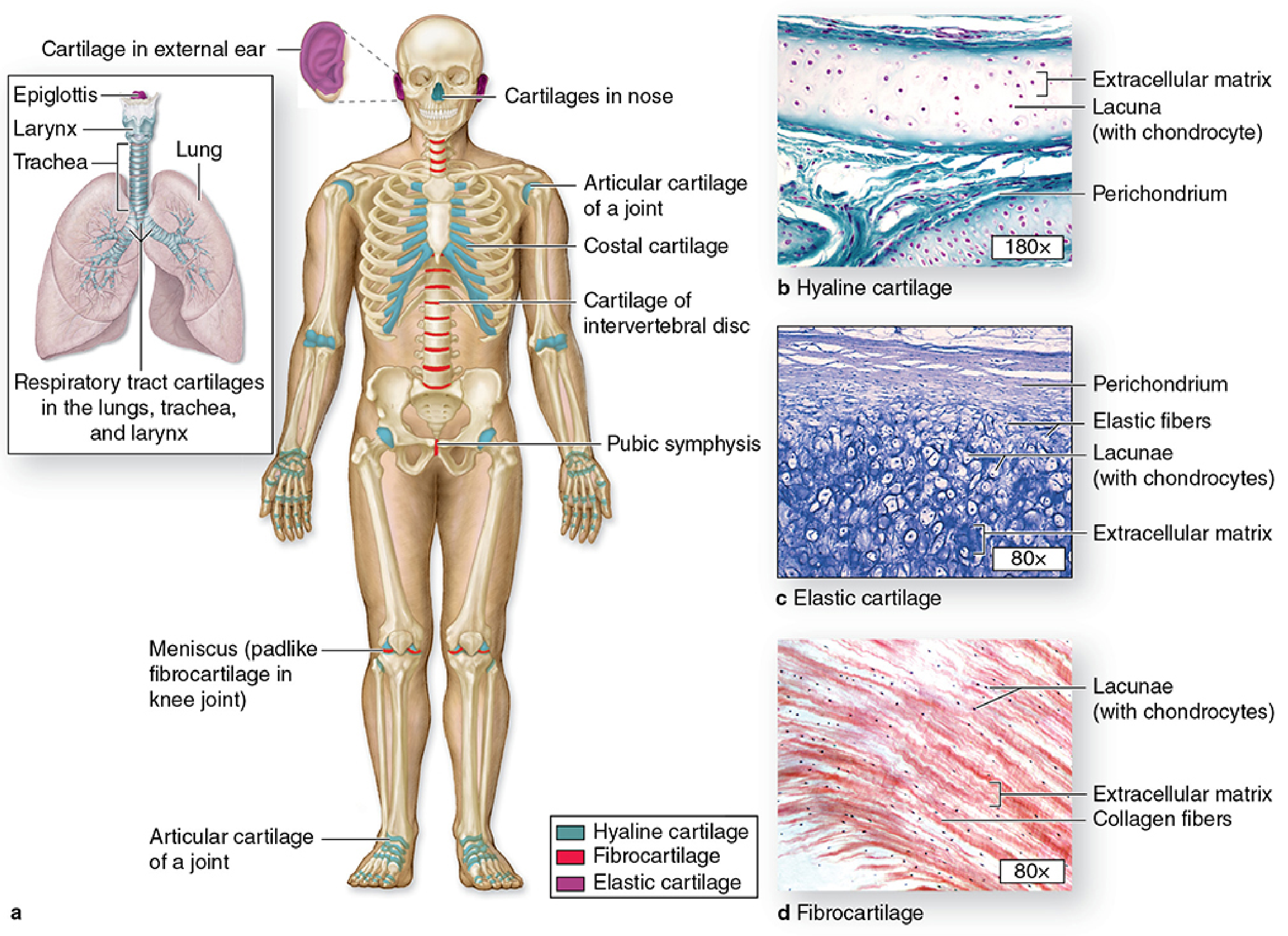
| Feature | Hyaline Cartilage | White Fibrocartilage |
|---|---|---|
| Gross appearance | Glassy, bluish-white, translucent | Opaque, dull white, tough |
| Matrix appearance (H&E) | Homogeneous, amorphous, glassy (basophilic due to GAGs) | Fibrous, eosinophilic (acidophilic) due to abundant collagen; less ground substance |
| Collagen type | Predominantly type II collagen (thin fibrils, not visible with routine stains - masked by ground substance) | Type I collagen (thick bundles, clearly visible) AND type II collagen |
| Collagen visibility | Fibres not visible by light microscopy (masked by proteoglycans) | Collagen bundles clearly visible as coarse pink/red wavy bundles between chondrocytes |
| Ground substance (GAGs) | Abundant - hyaluronan, chondroitin sulfate, keratan sulfate; aggrecan is the dominant proteoglycan | Sparse; relatively low proteoglycan content → less water binding |
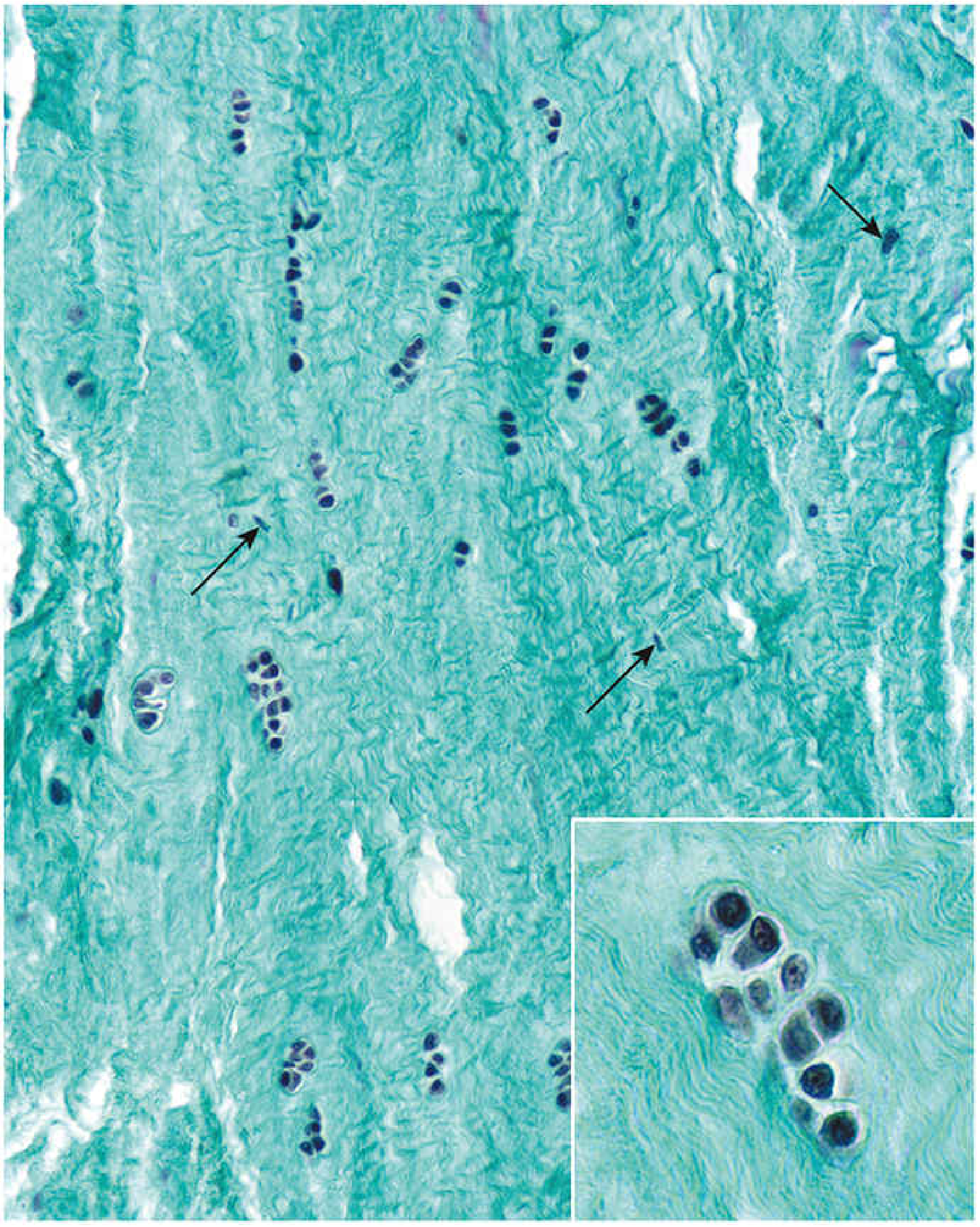
| Cells | Chondrocytes in lacunae - round, plump; arranged singly or in isogenous groups (clusters of 2-8) | Chondrocytes in lacunae arranged singly, in rows, or in isogenous groups; ALSO fibroblasts with flattened/elongated nuclei between collagen bundles |
| Isogenous groups | Prominent - chondrocytes divide and form clusters | Present but less prominent; chondrocytes often arranged in linear rows along collagen bundles |
| Territorial/capsular matrix | Well-defined - darker-staining capsular matrix surrounds each lacuna/isogenous group; territorial and interterritorial matrix zones clearly distinct | Less distinct zoning; little amorphous matrix around cells |
| Perichondrium | Present (except on articular surfaces of synovial joints) - two layers: outer fibrous and inner chondrogenic | Absent - no perichondrium |
| Vascularity | Avascular | Avascular |
| Calcification | Calcifies with age (except articular cartilage) | Does not calcify readily |
| Staining reaction | Basophilic/metachromatic matrix (positive PAS, Alcian blue) due to high GAG content | Acidophilic matrix due to low GAG and abundant type I collagen |
| Mechanical properties | Resistant to compression; smooth, lubricated surface for gliding | Resistant to both compression AND tensile/shearing forces; very tough |
| Locations | Articular surfaces, costal cartilages, trachea and bronchi, nose, larynx, epiphyseal growth plates | Intervertebral discs, pubic symphysis, menisci of knee, articular discs of TMJ and sternoclavicular joint, insertions of tendons into bone |
Key Microscopic Features - Expanded
Hyaline Cartilage
- The matrix is the defining feature: homogeneous and amorphous - glassy under light microscopy
- Type II collagen fibrils are present but are same refractive index as ground substance, so they are invisible on routine H&E
- Three matrix zones around each chondrocyte: capsular matrix (immediately around cell, richest in proteoglycans), territorial matrix (around each isogenous group, basophilic), and interterritorial matrix (between groups, less basophilic)
- Perichondrium is bilaminar: outer fibrous layer (type I collagen, fibroblasts) and inner chondrogenic layer (chondroblasts)
- Lacunae appear as clear spaces with shrunken chondrocytes (artifact of fixation)
White Fibrocartilage
- Appears as a mixture of dense regular connective tissue and hyaline cartilage
- Thick type I collagen bundles run parallel in the matrix and are clearly visible as coarse eosinophilic wavy bundles
- Two cell populations are visible in the same section:
- Chondrocytes - round nuclei, in lacunae with a small rim of basophilic matrix
- Fibroblasts - elongated/flattened nuclei, scattered between collagen bundles
- Chondrocytes may be in linear rows (running parallel to collagen bundles - classic feature of intervertebral disc) or in small isogenous groups
- There is very little amorphous ground substance visible - the matrix is predominantly fibrous
- No perichondrium
- The relative scarcity of proteoglycans makes the matrix more acidophilic (pink) on H&E, unlike the basophilic hyaline cartilage matrix
Summary: The Essential Differences
| Hyaline | Fibrocartilage | |
|---|---|---|
| Matrix | Glassy, amorphous, basophilic | Fibrous, eosinophilic |
| Dominant collagen | Type II (invisible) | Type I (visible) + Type II |
| Ground substance | Abundant | Sparse |
| Cell types | Chondrocytes only | Chondrocytes + fibroblasts |
| Perichondrium | Present (except articular) | Absent |
| Calcification | Yes (with age) | No |
- Histology: A Text and Atlas (Ross & Pawlina), p. 563-570; Junqueira's Basic Histology 17e, p. 331-341