Skin anatomy physiology function and skin appendages
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Excellent. I now have comprehensive content from the textbooks. Let me compile the full, detailed response:
Skin: Anatomy, Physiology, Functions, and Appendages
1. Overview of the Integumentary System
The skin (cutis/integument) is the largest organ of the body, covering an external surface area of approximately 1.8 m² and constituting 15-20% of total body mass. Together with its derivatives (hair, nails, sweat glands, sebaceous glands), it forms the integumentary system.
Skin is broadly categorized as:
- Thick skin - palms of hands and soles of feet; hairless, thicker epidermis, greater abrasion resistance
- Thin skin - everywhere else; thinner epidermis, contains hair follicles
2. Structure: Layers of the Skin
Skin is divided into two primary layers (plus a deeper hypodermis):
A. Epidermis (5% of skin)
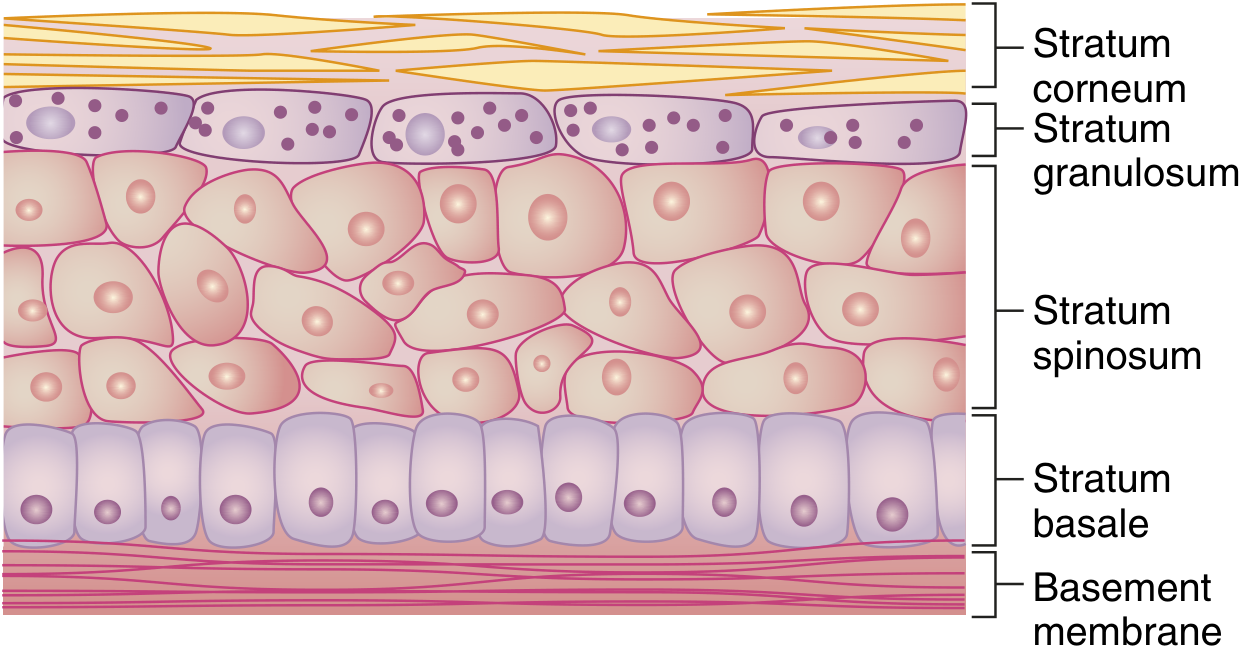
Composed of keratinized stratified squamous epithelium derived from ectoderm. It grows continuously but maintains normal thickness through desquamation. There are 5 layers (strata) from deep to superficial:
| Layer | Features |
|---|---|
| Stratum Basale (germinativum) | Deepest layer; single row of columnar/cuboidal cells; site of mitosis; contains melanocytes |
| Stratum Spinosum | "Prickle cell layer"; cells connected by desmosomes; contains Langerhans cells (APCs) |
| Stratum Granulosum | Cells contain keratohyalin granules; lamellar bodies released here form the water barrier |
| Stratum Lucidum | Present only in thick skin (palms, soles); translucent dead cells |
| Stratum Corneum | Most superficial; flat, anucleate, fully keratinized dead cells; protective barrier |
Keratinocytes are classified according to their depth and degree of differentiation - they proliferate in the basal layer, ascend, lose nuclei and organelles, and ultimately form the stratum corneum. - Bailey and Love's Short Practice of Surgery, 28th ed.
Epidermal cell replacement time: ~30 days (cells progress from basal layer to corneum in approximately 30 days, then shed).
Cells of the Epidermis
- Keratinocytes - predominant cell type (~90%); produce keratin
- Melanocytes - neural crest-derived dendritic cells in the basal layer; synthesize melanin (brown-black pigment) transferred to keratinocytes via membrane processes; protect against UV radiation. Ethnic differences in skin colour are determined by variations in melanin amount, combination, and distribution, not by differences in melanocyte number. - Bailey and Love's
- Langerhans cells - dendritic antigen-presenting cells in the stratum spinosum; part of the skin immune system
- Merkel cells - mechanoreceptors in the basal layer; associated with nerve endings; function in light touch discrimination
Epidermal Water Barrier
The lipid envelope (5 nm) - ceramides, cholesterol, free fatty acids - and the cell envelope (15 nm) - cross-linked structural proteins including loricrin (the major protein, ~80% of CE mass), involucrin, filaggrin, and cystatins - together form a "Teflon-like" barrier preventing transcutaneous water loss. Destruction over large areas (e.g., severe burns) can cause life-threatening fluid loss. - Histology: A Text and Atlas, 9e
B. Dermis (95% of skin)
Composed of dense irregular connective tissue derived from mesoderm. It is structurally divided into two layers:
| Layer | Description |
|---|---|
| Papillary dermis (superficial) | Delicate collagen and elastin fibres in ground substance; contains capillary and lymphatic networks; forms dermal papillae projecting into the epidermis |
| Reticular dermis (deep) | Coarse branching collagen fibres layered parallel to the skin surface; thicker, provides tensile strength |
The epidermis and dermis meet at the dermoepidermal junction (DEJ) - a basement membrane zone. In thick skin this creates an undulating surface with dermal papillae and rete ridges (epidermal ridges), which increases surface area and forms fingerprints.
Dermis contains:
- Collagen (type I - reticular; type III - papillary)
- Elastic fibres (elastin + fibrillin microfibrils)
- Ground substance (glycosaminoglycans, proteoglycans)
- Blood vessels, lymphatics
- Nerve fibres and sensory receptors
- Fibroblasts, mast cells, macrophages
- Skin appendages (hair follicles, sweat glands, sebaceous glands)
C. Hypodermis (Subcutaneous Layer)
- Deep to the dermis; equivalent to subcutaneous fascia
- Contains variable amounts of adipose tissue arranged in lobules separated by connective tissue septa
- Functions: energy storage, thermal insulation, mechanical cushioning, attachment of skin to underlying structures - Histology: A Text and Atlas, 9e
3. Functions of the Skin
The skin performs multiple vital functions:
1. Barrier / Protection
- Mechanical barrier - keratin and stratified epithelium resist abrasion and injury
- Permeability barrier - lipid envelope prevents transcutaneous water loss (TEWL); also prevents absorption of harmful external substances
- UV barrier - melanin absorbs and dissipates UV radiation, protecting DNA
- Chemical barrier - acid surface pH (~4.5-5.5) protects against pathogenic microorganisms
- Infection barrier - intact skin prevents microbial invasion; skin microbiome contributes to protection
2. Thermoregulation
- Sweat glands - eccrine sweating dissipates heat through evaporation
- Cutaneous blood vessels - vasodilation cools the body; vasoconstriction conserves heat
- Subcutaneous fat - acts as thermal insulator
- Hair erection (piloerection) via arrector pili muscles traps warm air in cold conditions
3. Sensory Function
Skin contains an array of sensory receptors conveying touch, pressure, vibration, pain, temperature, and itch to the CNS:
| Receptor | Location | Modality |
|---|---|---|
| Meissner's corpuscle | Dermal papillae; fingertips, lips | Fine/discriminative touch; rapidly adapting |
| Pacinian corpuscle | Deep dermis/hypodermis | Pressure and vibration; rapidly adapting |
| Merkel's disc | Stratum basale | Fine touch, texture; slowly adapting |
| Ruffini corpuscle | Reticular dermis | Stretch, torque, sustained pressure; rapidly adapting |
| Free nerve endings | Epidermis and dermis | Pain, temperature, itch |
| Krause end bulbs | Mucous membranes | Temperature (cold) |
4. Immune Function
- Langerhans cells process antigens and present to T-lymphocytes
- Skin-associated lymphoid tissue (SALT) participates in immune surveillance
- Provides immunologic information to effector cells in lymphatic tissue
5. Endocrine / Metabolic Functions
- Vitamin D synthesis - UV-B converts 7-dehydrocholesterol in the skin to cholecalciferol (vitamin D3)
- Secretes hormones, cytokines, and growth factors
- Converts precursor molecules into hormonally active substances
6. Excretion
- Eccrine sweat glands excrete water, electrolytes (Na⁺, Cl⁻, K⁺), urea, lactate
- Sebaceous glands secrete sebum
- Apocrine glands contribute to excretion
7. Absorption
- Lipid-soluble substances can be absorbed transdermally (basis of transdermal drug delivery systems - nicotine patches, steroid hormones, antiemetics)
4. Skin Appendages (Epidermal Derivatives)
Skin appendages are downgrowths of epidermal epithelium during development (ectodermal origin). They extend into the dermis and hypodermis.
A. Hair Follicles and Hair
Hair follicles are invaginations of the epidermis into the dermis in which a hair is formed. Present over almost the entire body except: palmar surfaces of hands, plantar surfaces of feet, lips, labia minora, glans penis, and nipples.
Hair distribution is influenced by sex hormones: facial hair appears at puberty in males; pubic and axillary hair at puberty in both sexes. Scalp hair thins with age due to reduced estrogen.
Structure of the Hair Follicle:
- Hair bulb - base of follicle; contains the dermal papilla (vascular connective tissue) and matrix cells (rapidly dividing stem cells that produce hair)
- Inner root sheath - surrounds and shapes the hair
- Outer root sheath - continuity with the epidermis
- Bulge region - in the isthmus; contains hair follicle stem cells important for hair cycling and wound repair
- Arrector pili muscle - smooth muscle; causes piloerection ("goose bumps")
Hair Growth Cycle:
- Anagen (growth phase) - matrix cells actively divide and differentiate
- Catagen (transition) - regression and apoptosis of lower follicle
- Telogen (resting/shedding) - hair shed; follicle rests before new anagen
Hair structure: keratinized thread with medulla (centre), cortex, and cuticle. Hair colour depends on melanin type - eumelanin (brown-black), phaeomelanin (red-yellow).
B. Nails
Nails are keratinized plates on the dorsal surface of the distal phalanges of fingers and toes.
Structure:
- Nail plate - hard, translucent keratinized structure
- Nail bed - epithelium under the nail plate
- Nail matrix (root) - beneath the proximal nail fold; site of nail formation (keratinisation of matrix cells)
- Lunula - whitish crescent-shaped area at the proximal nail; visible part of the matrix
- Hyponychium - junction of nail bed and fingertip skin
- Eponychium (cuticle) - proximal fold of skin overlying the nail matrix
- Paronychium - lateral nail folds
Functions: protection of fingertips, manipulation of small objects, scratching, cosmetic.
Growth rate: fingernails ~3-4 mm/month; toenails ~1-2 mm/month.
C. Sebaceous Glands
- Holocrine glands - entire cell disintegrates to release secretion (sebum)
- Found almost everywhere on the skin except palms and soles
- Open into hair follicle canal (pilosebaceous unit); independent sebaceous glands open directly on certain surfaces (lips, eyelids - Meibomian glands, areola - Montgomery glands)
- Secretion: Sebum - mixture of triglycerides, wax esters, squalene, cholesterol, free fatty acids
- Functions of sebum: lubricates and waterproofs skin and hair, antimicrobial properties (acidic pH), may have roles in vitamin E delivery and pheromone communication
- Stimulated by androgens (especially testosterone/DHT); active at puberty; overactivity leads to acne
- Inactive in childhood, become active at puberty
D. Sweat Glands (Sudoriferous Glands)
Two types:
1. Eccrine (Merocrine) Sweat Glands
- Most numerous sweat glands (~3-4 million on the body)
- Found over most of the body surface; greatest density on palms, soles, and forehead
- Not associated with hair follicles - open directly onto the skin surface
- Structure: simple coiled tubular gland; coiled secretory portion in deep dermis/hypodermis; straight/coiled duct rising to the surface
- Secretion: watery sweat - water, NaCl, KCl, urea, lactic acid, ammonia, IgA
- Functions:
- Thermoregulation (primary function) - evaporative cooling
- Minor excretory role
- Helps maintain acidic skin pH
- Innervated by cholinergic sympathetic nerve fibres (unusual - sympathetic but uses ACh)
2. Apocrine Sweat Glands
- Larger than eccrine glands
- Found in limited locations: axillae, areola of nipple, perianal region, external ear canal (ceruminous glands), eyelids (Moll's glands)
- Associated with hair follicles - drain into the upper portion of the follicle above the sebaceous gland
- Become active at puberty (androgen-dependent)
- Secretion: viscous, oily, protein-rich fluid containing carbohydrates, lipids, proteins, and pheromone-like compounds; odourless when secreted but odour develops when broken down by skin bacteria
- Function: pheromone secretion (sex attractant function - well-established in animals, possible in humans); emotional sweating (anxiety, fear, sexual excitement)
- Innervated by adrenergic sympathetic nerve fibres
| Feature | Eccrine | Apocrine |
|---|---|---|
| Distribution | Whole body | Axilla, areola, anogenital |
| Hair follicle | Independent | Associated |
| Onset | Birth | Puberty |
| Secretion | Watery (electrolytes, urea) | Viscous (lipids, proteins) |
| Function | Thermoregulation | Pheromones, emotional |
| Innervation | Cholinergic sympathetic | Adrenergic sympathetic |
E. Mammary Glands
Mammary glands are modified apocrine glands. They are epidermal appendages specialized for milk production (lactation) and are considered part of the integumentary system.
5. Sensory Receptors of the Dermis
The dermis contains encapsulated and unencapsulated nerve endings:
- Encapsulated mechanoreceptors: Meissner's corpuscles, Pacinian corpuscles, Ruffini corpuscles, Krause end bulbs
- Unencapsulated receptors: Merkel's discs (associated with Merkel cells in the epidermis), free nerve endings
Ruffini corpuscles are elongated fusiform encapsulated receptors (1-2 µm length) that respond to sustained mechanical stress, stretch, and torque. They are considered rapidly adapting (phasic) receptors that generate action potentials at the beginning and end of a stimulus. - Histology: A Text and Atlas, 9e
6. Summary Diagram
SKIN
├── Epidermis (5%)
│ ├── Stratum Corneum ← dead, keratinized cells
│ ├── Stratum Lucidum ← only in thick skin
│ ├── Stratum Granulosum ← lamellar bodies, water barrier
│ ├── Stratum Spinosum ← Langerhans cells, desmosomes
│ └── Stratum Basale ← stem cells, melanocytes, Merkel cells
│
├── Dermis (95%)
│ ├── Papillary layer ← delicate collagen, capillaries, receptors
│ └── Reticular layer ← coarse collagen, elastic fibres
│
├── Hypodermis
│ └── Adipose tissue, loose connective tissue
│
└── Appendages (epidermal origin)
├── Hair follicles + arrector pili
├── Nails
├── Sebaceous glands (holocrine; sebum; androgen-driven)
├── Eccrine sweat glands (thermoregulation; cholinergic)
└── Apocrine sweat glands (pheromones; adrenergic; puberty onset)
Sources:
- Histology: A Text and Atlas with Correlated Cell and Molecular Biology, 9e (Pawlina), pp. 1278-1342
- Bailey and Love's Short Practice of Surgery, 28th ed. - Functional Anatomy and Physiology of Skin; Surgical Anatomy of the Skin
- Rosen's Emergency Medicine, Surface Anatomy and Skin
Give me some pathology like bulla papule and so on
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive, authoritative content from Harrison's, Goldman-Cecil, Harriet Lane, and Symptom to Diagnosis. Here is the full response:
Skin Pathology: Morphology of Skin Lesions
Dermatology has its own vocabulary. The correct approach to any rash is to identify the primary lesion first - the typical element of the eruption - and then note secondary changes, configuration, distribution, and colour. The differential diagnosis of a rash should be based on the morphology of the lesion, which serves as the first pivotal point. - Goldman-Cecil Medicine
PRIMARY SKIN LESIONS
These arise directly from the disease process - they have not been modified by scratching, treatment, or time.
1. Macule
- Definition: Flat, circumscribed area of colour change, < 1-2 cm in diameter; NOT elevated or depressed; not palpable
- Pathology: Change in melanin, blood (haemoglobin), or exogenous pigment in the epidermis or superficial dermis; no structural change in skin surface
- Examples: Freckle (ephelid), cafe-au-lait spot, vitiligo, early measles rash, petechia (small)
- Key point: You can SEE it but cannot FEEL it
2. Patch
- Definition: A large macule, > 1-2 cm (some sources say > 0.5 cm); flat, non-palpable area of colour change
- Examples: Vitiligo patches, port-wine stain (nevus flammeus), Mongolian spot, large areas of tinea versicolor
- Key point: Differs from macule only in SIZE
3. Papule
- Definition: Small, solid, elevated, well-circumscribed lesion < 0.5-1 cm in diameter; palpable; raised above surrounding skin
- Pathology: May result from epidermal hyperplasia, dermal infiltration, or accumulation of metabolic products
- Examples: Warts (verruca vulgaris), molluscum contagiosum, closed comedone (whitehead), lichen planus (flat-topped violaceous papule), acne lesions, insect bites
- Key point: You can SEE it AND FEEL it; it is SOLID (no fluid)
4. Plaque
- Definition: Large (> 1 cm), flat-topped, raised lesion - essentially a large papule or confluence of papules
- Pathology: Same processes as papule but larger; edges may be distinct (psoriasis) or gradually blend (eczema)
- Examples: Psoriasis (well-demarcated silvery-scaled plaques), eczematous dermatitis, mycosis fungoides, discoid lupus erythematosus
- Key point: Think of it as a "raised plateau" - large surface area, flat top
5. Nodule
- Definition: Solid, firm lesion raised above the skin surface, 0.5-5 cm in diameter; extends deeper into the dermis or subcutaneous tissue than a papule
- Pathology: Dermal or subcutaneous infiltration (inflammatory cells, neoplastic cells, deposits)
- Examples: Lipoma, rheumatoid nodule, erythema nodosum, dermatofibroma, large melanocytic nevus, lymphoma cutis
- Key point: DEEPER than a papule; can be felt rolling under the fingers
6. Tumor / Mass
- Definition: Solid, raised growth > 5 cm in diameter (some sources: > 2 cm); extends into the dermis/subcutis
- Examples: Large cutaneous malignancies, large lipoma, pilomatrixoma
- Key point: Distinguished from nodule by SIZE only
7. Vesicle
- Definition: Small, fluid-filled blister < 0.5-1 cm in diameter; raised above surrounding skin; fluid often visible and translucent
- Pathology: Intraepidermal oedema (spongiosis), acantholysis, or subepidermal separation; roof = epidermis; content = clear serous fluid
- Examples:
- Herpes simplex / herpes zoster (varicella) - grouped vesicles on erythematous base
- Allergic contact dermatitis (poison ivy/oak)
- Dyshidrotic eczema (pompholyx) - vesicles on palms and soles
- Early chickenpox
- Key point: Fluid-filled; SMALL (< 1 cm); translucent
8. Bulla
- Definition: A large vesicle (fluid-filled blister) > 0.5-1 cm in diameter; elevated, often tense or flaccid
- Pathology: Subepidermal (tense bullae - BP, EBA) or intraepidermal (flaccid bullae - pemphigus vulgaris) blister formation
- Sub-types by location:
- Intraepidermal - flaccid, easily ruptured (e.g., pemphigus vulgaris - acantholysis above the basal layer)
- Subepidermal - tense, more durable (e.g., bullous pemphigoid - IgG + complement at BMZ)
- Examples:
- Bullous pemphigoid - tense bullae, elderly, autoimmune (anti-BP180/BP230)
- Pemphigus vulgaris - flaccid bullae, mucosal involvement, Nikolsky sign positive
- Epidermolysis bullosa - inherited fragility
- Impetigo (bullous type) - honey-coloured rupturing bullae, Staph. aureus
- Burns, severe contact dermatitis
- Key point: Fluid-filled; LARGE (> 1 cm); may be tense or flaccid
| Vesicle | Bulla | |
|---|---|---|
| Size | < 1 cm | > 1 cm |
| Content | Clear fluid | Clear/serosanguineous |
| Examples | Herpes, contact derm | Pemphigoid, pemphigus |
9. Pustule
- Definition: Well-circumscribed, elevated lesion filled with purulent material (pus = dead neutrophils + bacteria/debris); any size
- Pathology: Intraepidermal or subepidermal collection of neutrophils
- Key point: Presence of pustules does NOT necessarily indicate infection - sterile pustules occur in many inflammatory conditions
- Examples:
- Infected: Folliculitis, impetigo, furuncle
- Sterile: Psoriasis (pustular psoriasis), acne vulgaris, rosacea, palmoplantar pustulosis
10. Wheal (Urtica / Hive)
- Definition: Transient (typically < 24 hours), raised, well-circumscribed lesion with an erythematous periphery and central pallor; an inflamed oedematous papule or plaque formed by superficial local oedema
- Pathology: Mast cell degranulation → histamine release → transient vasodilation and increased vascular permeability in the dermis → localised oedema
- Examples: Urticaria (hives), allergic reactions, dermatographism
- Key point: TRANSIENT - comes and goes within hours; oedematous; itchy
11. Cyst
- Definition: Encapsulated, fluctuant lesion filled with soft semi-solid or liquid material (not just fluid); has an epithelial lining
- Examples: Epidermal inclusion cyst, sebaceous cyst, pilar cyst, dermoid cyst, milia
- Key point: Has a WALL (cyst capsule) - distinguishes it from a simple vesicle/bulla
12. Comedone
- Definition: A plug of keratinous material and skin oils retained in a hair follicle
- Open comedone (blackhead): Open to the air; black colour from oxidised melanin (not dirt)
- Closed comedone (whitehead): Covered by thin layer of skin; flesh-coloured or pinkish
- Pathology: Sebaceous duct obstruction; precursor of acne vulgaris
- Symptom to Diagnosis, 4e
13. Telangiectasia
- Definition: Dilated, superficial blood vessel visible on the skin surface; does not blanch with pressure (unlike erythema)
- Examples: Rosacea, hereditary haemorrhagic telangiectasia (HHT/Osler-Weber-Rendu), CREST syndrome, spider naevi, ataxia-telangiectasia
SECONDARY SKIN LESIONS
These develop from primary lesions due to scratching, infection, healing, or time.
| Lesion | Definition | Key Features |
|---|---|---|
| Scale | Excessive accumulation / shedding of stratum corneum cells | Seen in psoriasis (silvery), tinea (fine), pityriasis rosea, ichthyosis |
| Crust | Dried exudate (serum, pus, blood) on the skin surface | Yellow = serous/infected; red = haemorrhagic; "honey-coloured" = impetigo |
| Erosion | Superficial loss of epidermis ONLY; does NOT reach the dermis | Heals WITHOUT scarring; moist, shallow |
| Ulcer | Full-thickness loss of epidermis AND at least part of the dermis | Heals WITH scarring; may show necrosis, base exposed |
| Fissure | Linear or wedge-shaped epidermal crack/tear extending into the dermis | Painful; at sites of repeated movement - heels, fingers, lips |
| Excoriation | Linear, angular erosion caused by scratching; may be crusted | Sign of pruritus; seen in atopic dermatitis, scabies, neurotic excoriation |
| Lichenification | Thickened, leathery epidermis with accentuated skin markings | Chronic scratching/rubbing; typical of chronic atopic dermatitis |
| Scar | New connective tissue replacing damaged dermis after full-thickness injury | May be hypo/hyperpigmented; hypertrophic scar = stays within wound; keloid = grows beyond wound |
| Atrophy | Loss of skin substance | Epidermal atrophy = shiny, thin, wrinkled; dermal atrophy = depression; caused by topical steroids, lichen sclerosus |
SPECIAL / VASCULAR LESIONS
| Lesion | Definition | Examples |
|---|---|---|
| Petechiae | Pinpoint (< 2 mm) red/purple non-blanching spots from RBC extravasation | Thrombocytopenia, vasculitis, meningococcaemia |
| Purpura | Larger red-purple non-blanching areas from RBC extravasation | Palpable = leukocytoclastic vasculitis; non-palpable = coagulopathy |
| Ecchymosis | Large area of purpura ("bruise") from haemorrhage into skin | Trauma, coagulopathy |
| Retiform purpura | Net/lace-like purpura with concave borders | Occlusive vasculopathy (thrombosis, emboli); potentially life-threatening |
Purpura is caused by extravasation of red blood cells into the skin, resulting in a reddish to dark purple to black colour. Palpable purpura suggests small vessel leukocytoclastic vasculitis. Retiform purpura - with concave, net-like, scalloped borders - can signal a life-threatening disorder. - Goldman-Cecil Medicine
CONFIGURATION PATTERNS (Arrangement of Lesions)
The arrangement of lesions is a key diagnostic clue:
| Pattern | Description | Example |
|---|---|---|
| Linear | Along a line | Contact dermatitis (linear), lichen striatus |
| Dermatomal | Following a dermatome | Herpes zoster |
| Annular | Ring-like configuration | Tinea corporis (ringworm), erythema migrans (Lyme) |
| Serpiginous | Wavy/coiled/snake-like | Cutaneous larva migrans |
| Targetoid | Bull's-eye (central dark zone, pale ring, outer red ring) | Erythema multiforme |
| Nummular/Discoid | Coin-shaped | Nummular eczema |
| Grouped/Herpetiform | Clustered on an erythematous base | Herpes simplex, herpes zoster |
| Filiform | Thread-like | Filiform warts |
QUICK REFERENCE SUMMARY TABLE
| Lesion | Flat/Raised | Fluid? | Size | Key Example |
|---|---|---|---|---|
| Macule | Flat | No | < 1-2 cm | Freckle, vitiligo |
| Patch | Flat | No | > 1-2 cm | Port-wine stain |
| Papule | Raised | No (solid) | < 1 cm | Wart, comedone |
| Plaque | Raised (flat-top) | No (solid) | > 1 cm | Psoriasis |
| Nodule | Raised (deep) | No (solid) | 0.5-5 cm | Lipoma, rheumatoid nodule |
| Tumor | Raised (deep) | No (solid) | > 5 cm | Large malignancy |
| Vesicle | Raised | Yes (clear) | < 1 cm | Herpes, contact derm |
| Bulla | Raised | Yes (clear) | > 1 cm | Pemphigoid, burns |
| Pustule | Raised | Yes (pus) | Any size | Folliculitis, pustular psoriasis |
| Wheal | Raised (transient) | Oedema | Variable | Urticaria |
| Cyst | Raised | Semi-solid | Variable | Epidermal cyst |
Sources:
- Harrison's Principles of Internal Medicine, 22e (2025) - Tables 39-1 and 39-2
- Goldman-Cecil Medicine, International Edition - Chapter 403: Morphology, Configuration, Palpation
- The Harriet Lane Handbook, 23e (Johns Hopkins) - Evaluation and Clinical Descriptions of Skin Findings
- Symptom to Diagnosis: An Evidence-Based Guide, 4e - Constructing a Differential Diagnosis
This is a shared conversation. Sign in to Orris to start your own chat.