EXPLAIN THYROID ITS TYPE IN DETAIL AND THERE SYPMTOM WITH TREATMENT AND INVESTIGATION
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Searching Images
thyroid gland anatomy diagram
Reading File
Reading File
Reading File
Reading File
Finding Sources
Searching Images
Graves disease exophthalmos hyperthyroidism clinical signs
I now have comprehensive information from multiple authoritative textbooks. Let me compile a thorough, well-organized response.
🦋 THYROID GLAND — COMPREHENSIVE CLINICAL GUIDE
ANATOMY & OVERVIEW
The thyroid gland is a butterfly-shaped endocrine gland located in the anterior neck, inferior to the larynx, consisting of two lobes connected by an isthmus. It sits anterior to the trachea, closely related to the recurrent laryngeal nerves and parathyroid glands.
The gland produces T3 (triiodothyronine) and T4 (thyroxine), regulated by the hypothalamic–pituitary–thyroid (HPT) axis:
- Hypothalamus → releases TRH → stimulates pituitary
- Pituitary → releases TSH → stimulates thyroid
- Thyroid → T3/T4 feedback inhibits both
Thyroid disorders affect 60–80 per 1,000 adults worldwide and up to 8.9% of the US adult population. They exist in three functional states: euthyroid, hypothyroid, or hyperthyroid.
— Textbook of Family Medicine 9e
CLASSIFICATION OF THYROID DISORDERS
| Level | Type | Cause |
|---|---|---|
| Primary | Abnormal thyroid gland itself | Autoimmune, iodine deficiency, nodules |
| Secondary | Pituitary dysfunction | TSH deficiency from pituitary tumor |
| Tertiary | Hypothalamic dysfunction | Impaired TRH production |
1. HYPOTHYROIDISM
Definition
Insufficient production of thyroid hormone by the thyroid gland. Ranges from subclinical (elevated TSH, normal T4) to overt.
Causes
- Hashimoto's thyroiditis — most common cause in developed countries; autoimmune destruction with antithyroid peroxidase (anti-TPO) and antithyroglobulin antibodies
- Iodine deficiency — most common cause globally; presents with goiter
- Post-radioactive iodine treatment or post-thyroidectomy
- Drugs: Amiodarone (most common drug cause), lithium, phenytoin, rifampin, carbamazepine
- Infiltrative diseases: Riedel thyroiditis, hemochromatosis, amyloidosis
- Secondary: Pituitary tumors impairing TSH production (accompanied by hypogonadism and adrenal insufficiency)
- Subclinical hypothyroidism: TSH 4.5–20 mU/L with normal free T4
Symptoms & Signs
| System | Symptoms/Signs |
|---|---|
| General | Fatigue, lethargy, weight gain, cold intolerance |
| Skin/Hair | Dry cool skin, hair loss/thinning, loss of outer eyebrows, brittle nails, nonpitting edema |
| Neurologic | Decreased mental acuity, depression, delayed deep tendon reflexes (most sensitive sign — ankle jerk) |
| Cardiovascular | Bradycardia, diastolic hypertension, pericardial effusion (muffled heart sounds in severe cases) |
| GI | Constipation |
| Musculoskeletal | Proximal myopathy, elevated CK, carpal tunnel syndrome, Raynaud phenomenon, myxedematous arthropathy of large joints |
| Metabolic | Hypercholesterolemia (elevated LDL), hyponatremia, macrocytic anemia |
| Reproductive | Menstrual irregularities (heavy, prolonged menses) |
Myxedema Coma — life-threatening extreme: severe hypothermia, hypotension, bradycardia, altered mental status/coma. Medical emergency requiring immediate treatment.
— Goldman-Cecil Medicine
Investigations
| Test | Finding |
|---|---|
| TSH | ↑ (>4.5 mU/L) — most sensitive, first-line test |
| Free T4 | ↓ (confirms overt hypothyroidism) |
| Anti-TPO antibodies | Positive in Hashimoto thyroiditis |
| Antithyroglobulin antibodies | Positive in Hashimoto |
| Serum cholesterol (LDL) | ↑ (very sensitive indirect marker) |
| CK, AST | ↑ in muscle dysfunction |
| CBC | Macrocytic anemia (elevated MCV) |
| Serum sodium | Hyponatremia |
| Pituitary MRI | If secondary hypothyroidism suspected (low/normal TSH with low free T4) |
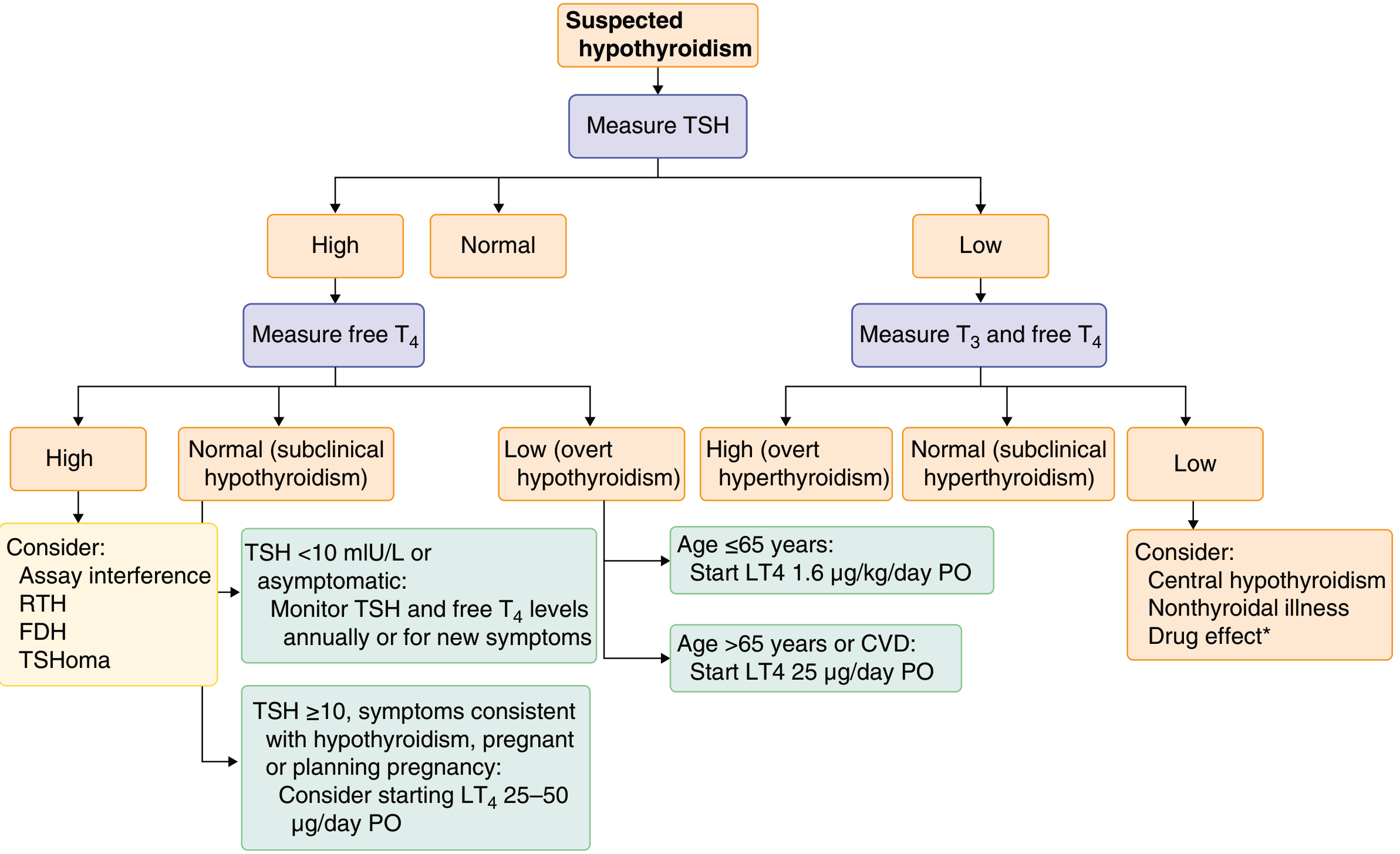
Diagnosis algorithm: TSH first → if elevated, check free T4 → if T4 low = overt hypothyroidism; if T4 normal = subclinical hypothyroidism
— Goldman-Cecil Medicine
Treatment
- Drug of choice: Levothyroxine (L-T4) — preferred over T3 or combination T3/T4 products
- Available in doses from 25 μg to 300 μg tablets
- Average dose: 1.6 µg/kg/day
- Take on empty stomach (absorption impaired by food, iron, calcium carbonate, aluminum hydroxide, sucralfate, cholestyramine, soy)
- Steady state achieved in 6–8 weeks; check TSH 5–6 weeks after initiating or changing dose
- Goal: Normalize TSH to the normal range
- Myxedema coma: IV thyroid hormone + supportive ICU care
- Drugs increasing metabolism of thyroxine (reduce effectiveness): Phenytoin, phenobarbital, carbamazepine, rifampin
- Pregnancy: Levothyroxine 1.6 µg/kg/day; PTU preferred for hyperthyroidism in first trimester — Lippincott Pharmacology; Goldman-Cecil Medicine
2. HYPERTHYROIDISM (THYROTOXICOSIS)
Definition
Overproduction and increased circulation of thyroid hormone. Spectrum: subclinical → overt thyrotoxicosis → thyroid storm (life-threatening).
Causes
- Graves' disease — most common cause; autoimmune, TSH-receptor stimulating antibodies (TRAb)
- Toxic multinodular goiter
- Toxic adenoma (solitary hot nodule)
- Subacute thyroiditis (de Quervain's) — transient
- Postpartum thyroiditis
- hCG-mediated (gestational, hydatidiform mole)
- Amiodarone-induced thyrotoxicosis
- Exogenous thyroid hormone excess
Symptoms & Signs
| System | Symptoms/Signs |
|---|---|
| General | Weight loss, heat intolerance, increased sweating |
| Cardiovascular | Palpitations, tachycardia (>100 bpm), atrial fibrillation |
| Neurologic/Psych | Nervousness, anxiety, tremor, insomnia |
| Musculoskeletal | Proximal myopathy (70%), adhesive capsulitis of shoulder (10%), osteoporosis |
| Eyes (Graves') | Exophthalmos/proptosis, lid retraction, Dalrymple sign (staring look), periorbital edema |
| Skin (Graves') | Pretibial myxedema (brawny induration of lower legs) |
| Extremities (Graves') | Thyroid acropachy (<1%): digital clubbing, soft tissue hand swelling, periosteal reaction |

Thyroid Storm — extreme hyperthyroid crisis with fever, extreme tachycardia, and altered mental status. Administration order is critical: Beta-blocker → PTU/methimazole → Iodine (iodine must be given ≥1 hour after thionamide to prevent worsening).
Investigations
| Test | Finding |
|---|---|
| TSH | ↓↓ (suppressed <0.1 mU/L) — first-line, most sensitive |
| Free T3 and T4 | ↑ |
| Thyroid-stimulating antibodies (TRAb/TSI) | Positive in Graves' disease |
| Radioactive iodine uptake (RAIU) scan | Diffuse uptake (Graves'), focal hot nodule (toxic adenoma), low uptake (thyroiditis) |
| Thyroid ultrasound | Diffuse enlargement, vascularity (Graves'), nodule characteristics |
| CBC | May show leukopenia (if on thionamides — check for agranulocytosis) |
Treatment
1. Antithyroid drugs (Thionamides)
- Methimazole — preferred (once-daily dosing, longer half-life, fewer adverse effects)
- PTU (propylthiouracil) — preferred in first trimester of pregnancy; also blocks peripheral T4→T3 conversion
- Both inhibit thyroid hormone synthesis; clinical effect delayed until stored thyroglobulin is depleted
- Adverse effects: rash, pruritus, arthralgia; agranulocytosis and hepatotoxicity (PTU has higher risk of fatal liver failure)
2. Radioactive Iodine (¹³¹I)
- Selectively taken up by follicular cells → destroys gland
- Most patients subsequently develop hypothyroidism and require lifelong levothyroxine
3. Surgery (Thyroidectomy)
- Preferred for large goiters, compressive symptoms, malignancy concern, or patient preference
- Preoperative iodide given to reduce vascularity
4. Beta-blockers (Propranolol, Metoprolol, Atenolol)
- Blunt widespread sympathetic stimulation (palpitations, tremor, anxiety)
- Essential in thyroid storm
5. Iodide (Wolff-Chaikoff effect)
- High-dose iodide briefly inhibits thyroid hormone synthesis and release
- Used for thyroid storm and pre-surgery
- Not useful long-term; adverse effects: metallic taste, mucosal ulceration — Lippincott Pharmacology; Goldman-Cecil Medicine; Rosen's Emergency Medicine
3. THYROIDITIS
Types
| Type | Features |
|---|---|
| Hashimoto's thyroiditis | Most common autoimmune thyroid disease; anti-TPO antibodies; leads to hypothyroidism |
| Subacute (de Quervain's) thyroiditis | Painful, viral; transient thyrotoxicosis then hypothyroidism |
| Painless (silent) thyroiditis | Can be postpartum; transient hyper then hypothyroidism; ~25% → permanent hypothyroidism |
| Riedel thyroiditis | Fibrous infiltration; may compress recurrent laryngeal nerve or parathyroids |
4. THYROID CANCER
Types & Frequency
| Type | % of Cases | Origin | Key Features |
|---|---|---|---|
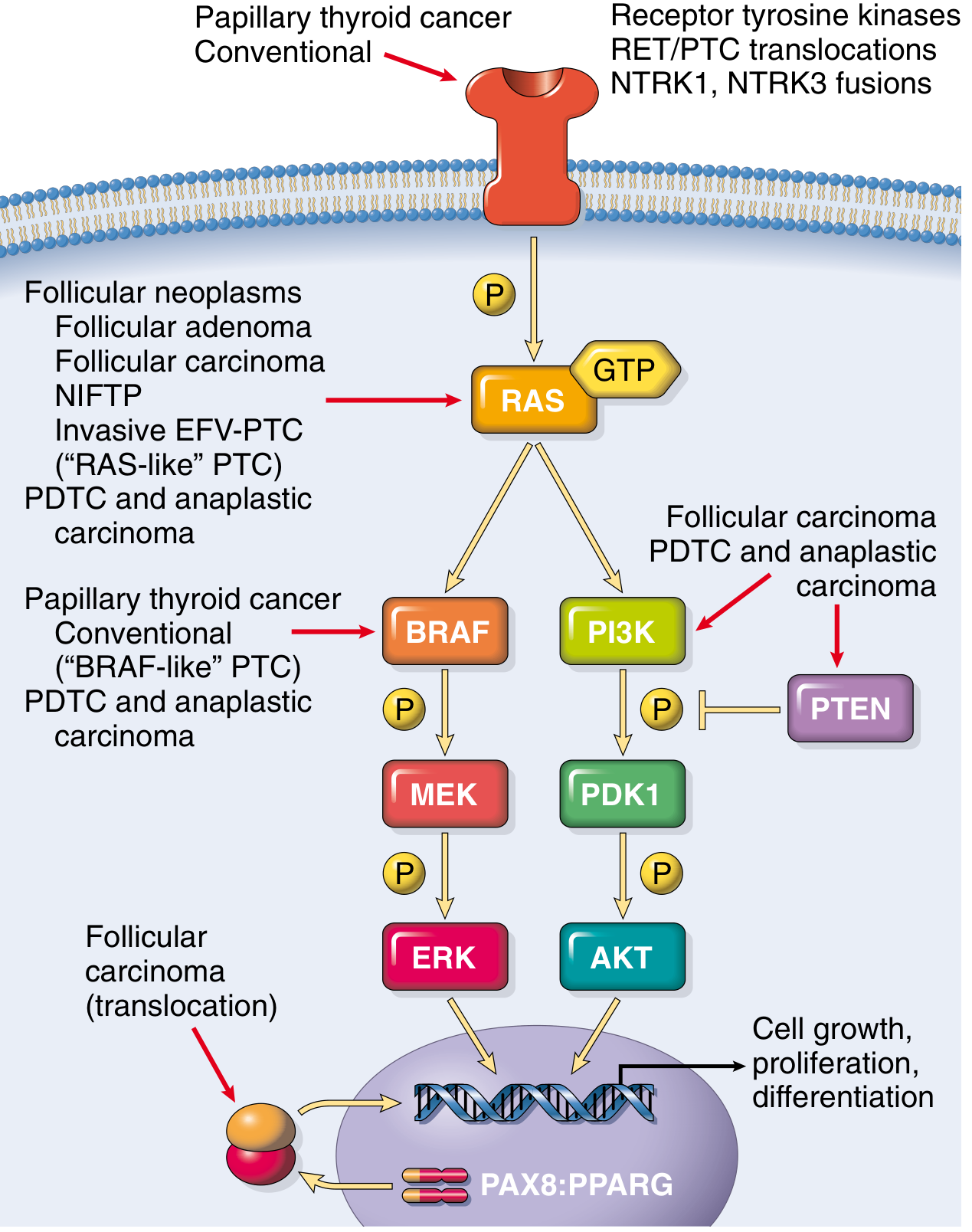
| Papillary carcinoma | ~70–80% | Follicular epithelium | Most common; BRAF V600E mutation; best prognosis; spreads via lymphatics |
| Follicular carcinoma | ~10–15% | Follicular epithelium | RAS or PAX8-PPARγ mutation; spreads hematogenously to lung/bone |
| Hürthle cell carcinoma | Variant of follicular | Oncocytic follicular cells | Refractory to radioactive iodine |
| Medullary thyroid cancer (MTC) | <5% | C cells (parafollicular) | Produces calcitonin; RET mutations; associated with MEN 2A/2B |
| Anaplastic (undifferentiated) | ~1% | Follicular epithelium | Most aggressive; poor prognosis |
| Lymphoma | Rare | Lymphoid tissue | Often in background of Hashimoto's |
Presentation
- Most present as an asymptomatic thyroid nodule (palpation or incidental imaging)
- Rarely: symptoms of metastatic disease
- Risk factors: Childhood radiation exposure, family history, MEN syndromes
Investigation
- Thyroid ultrasound — first-line for nodule evaluation
- Fine-needle aspiration (FNA) cytology — diagnostic standard
- TSH — if suppressed, radionuclide scan to rule out functioning nodule
- Serum calcitonin — elevated in medullary cancer
- Molecular markers: BRAF, RAS, RET/PTC, NTRK
- Staging CT/PET — for metastatic disease evaluation
Treatment
- Surgery (thyroidectomy) — primary treatment; lobectomy vs. total thyroidectomy based on size and risk
- Radioactive iodine (¹³¹I) — post-thyroidectomy for intermediate/high-risk differentiated cancer
- TSH suppression with levothyroxine — reduces stimulation of residual cancer cells
- External beam radiation — for unresectable or locally invasive disease
- Targeted therapy (RET inhibitors, BRAF inhibitors): Used for advanced/metastatic disease when surgery + RAI inadequate
- Active surveillance — for low-risk papillary microcarcinoma (<1 cm, no high-risk features) — Goldman-Cecil Medicine; Robbins Pathology; Goodman & Gilman's Pharmacology
5. GOITER & THYROID NODULES
- Goiter = enlarged thyroid gland; may be diffuse or nodular; can be associated with any functional state
- Simple/non-toxic goiter: Often iodine deficiency; managed with iodine supplementation or thyroidectomy if compressive
- Thyroid nodule: Common; evaluated by ultrasound + FNA; >90% are benign
- Multinodular goiter: Multiple nodules; may become autonomously functioning (toxic MNG) causing hyperthyroidism
SUMMARY TABLE: KEY DIAGNOSTIC TESTS
| Condition | TSH | Free T4 | Free T3 | Antibodies |
|---|---|---|---|---|
| Primary hypothyroidism | ↑↑ | ↓ | ↓ | Anti-TPO/TgAb (Hashimoto) |
| Subclinical hypothyroidism | ↑ mild | Normal | Normal | May be positive |
| Hyperthyroidism (Graves) | ↓↓ | ↑ | ↑ | TRAb/TSI positive |
| Subclinical hyperthyroidism | ↓ | Normal | Normal | Variable |
| Secondary hypothyroidism | Low/normal | ↓ | ↓ | Negative |
| Thyroid storm | Undetectable | ↑↑ | ↑↑ | — |
SOURCES
- Goldman-Cecil Medicine, International Edition (2-Volume Set)
- Textbook of Family Medicine, 9th Edition
- Lippincott Illustrated Reviews: Pharmacology
- Goodman & Gilman's The Pharmacological Basis of Therapeutics
- Rosen's Emergency Medicine: Concepts and Clinical Practice
- Robbins, Cotran & Kumar Pathologic Basis of Disease
This is a shared conversation. Sign in to Orris to start your own chat.