A 40-year-old man on treatment for diabetes and hypertension presents to the casualty with a progressive redness over the right thigh with pain over the last 3 days. The complaints started after a minor fall from the stairs where the patient sustained an abrasion over the right thigh. Examination reveals temperature of 40°C; PR=140/min; BP=80 mmHg systolic and RR=30/min. Local examination shows tenderness, erythema, patchy purplish discoloration, and crepitus over the anterior right thigh. Discuss the differential diagnosis, pathogenesis, investigations, treatment, and complications of the patient’s condition.
Reading File
Finding Sources
Finding Sources
Searching PubMed
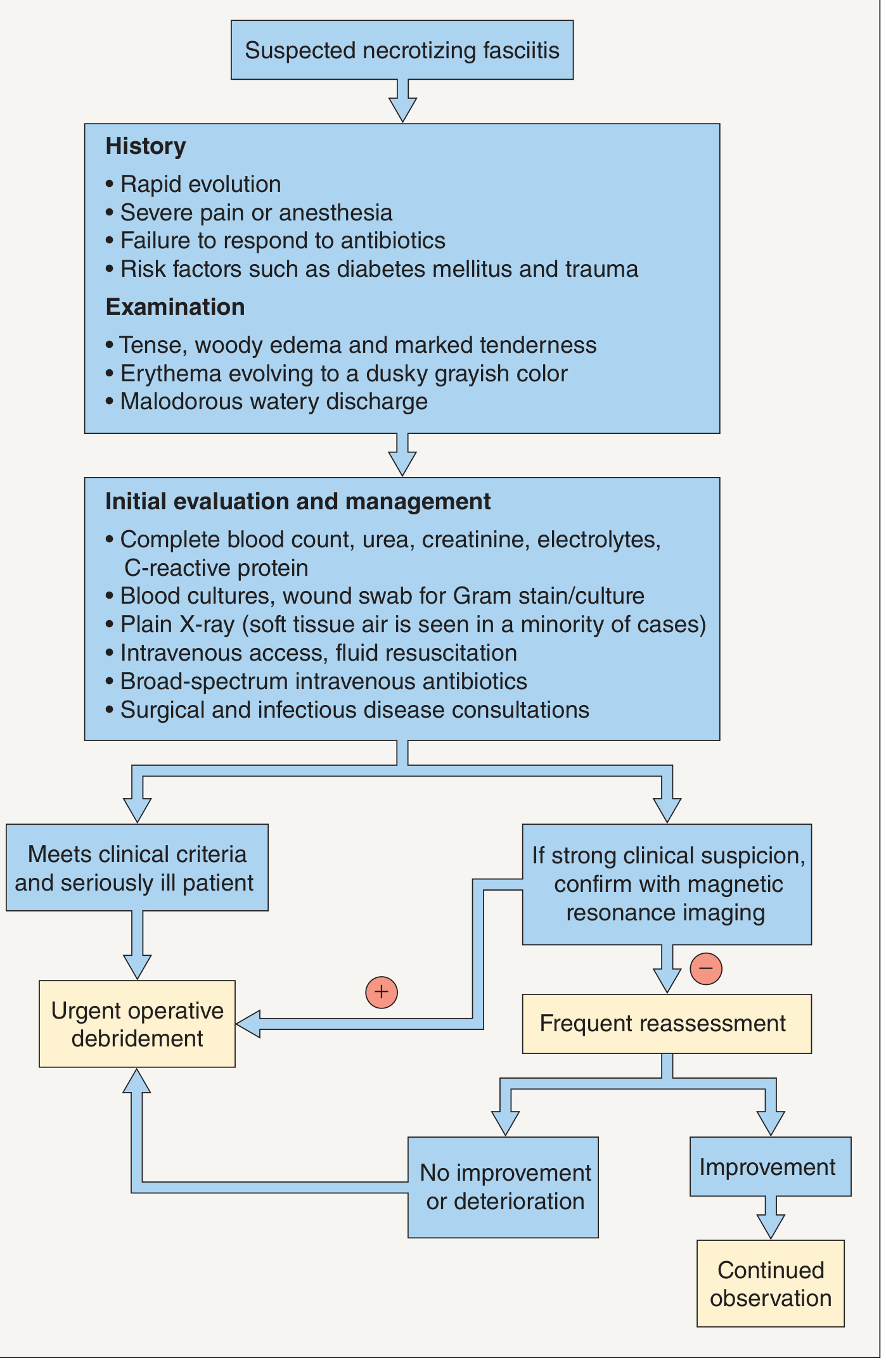
"necrotizing fasciitis" management treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
I now have all the information needed for a comprehensive, well-structured answer. Let me compile the full response.
Necrotizing Fasciitis - Comprehensive Discussion
This presentation is a surgical emergency. The combination of a portal of entry (abrasion after minor trauma), a 3-day rapidly progressive soft tissue infection, systemic sepsis (temp 40°C, HR 140, BP 80 systolic, RR 30), and the classic local triad of erythema → purplish discoloration + crepitus in an immunocompromised host (diabetes + hypertension) is necrotizing fasciitis (NF) until proven otherwise.
Clinical photo of necrotizing fasciitis showing erythema, blistering, and tissue necrosis:

1. Differential Diagnosis
Primary Diagnosis: Necrotizing Fasciitis (Type I - Polymicrobial)
The combination of rapid progression, systemic toxicity, crepitus (subcutaneous gas), purplish discoloration, and a diabetic patient strongly favors NF.
Differential Diagnoses to Consider
| Condition | Key Distinguishing Features |
|---|---|
| Severe cellulitis | No crepitus, no fascial plane involvement, less systemic toxicity; responds to antibiotics |
| Gas gangrene (Clostridial myonecrosis) | Caused by C. perfringens; involves muscle rather than fascia; extreme pain, bronze discoloration, sweet/mousy odor; X-ray shows feathery gas in muscle planes |
| Pyomyositis | Muscle involvement with abscess formation; common in tropics; no fascial spread; MRI distinguishes |
| Suppurative fasciitis (non-necrotizing) | Pus in fascial plane without necrosis; less systemic toxicity |
| Deep vein thrombosis (DVT) | Unilateral limb swelling/erythema, no fever or crepitus, Doppler positive |
| Phlegmasia cerulea dolens | Severe DVT with purplish discoloration, no gas, venous occlusion on imaging |
| Traumatic hematoma with secondary infection | History of trauma, imaging shows hematoma, no gas or fascial spread |
| Neutrophilic dermatoses (Sweet's, pyoderma gangrenosum) | Rapid skin necrosis but typically no gas, no systemic sepsis of this severity |
| Clostridial cellulitis | Crepitus present, but superficial - fascia and muscle spared |
Key differentiator: Crepitus + purplish discoloration + septic shock + diabetic host = necrotizing fasciitis until the operating room proves otherwise.
- Dermatology 2-Volume Set 5e, p. 1529
- Fitzpatrick's Dermatology, p. 2800
2. Pathogenesis
Entry and Bacterial Invasion
NF is most often community-acquired via bacterial introduction through a break in the skin - in this case, the traumatic abrasion on the right thigh. S. aureus, streptococci, Gram-negative enteric rods, and anaerobes enter the subcutaneous tissue simultaneously. Diabetes mellitus impairs neutrophil chemotaxis, reduces opsonization, and promotes microvascular ischemia, making the local defenses markedly inadequate.
Spread Along Fascial Planes
Once bacteria reach the superficial fascia, they encounter a relatively avascular space with limited immune surveillance. The infection spreads rapidly along fascial planes because:
- Enzymatic destruction - Streptococcal toxins (streptokinase, hyaluronidase, M-protein), staphylococcal toxins (hemolysins), and bacterial collagenases digest fascial connective tissue
- Anaerobic metabolism - Mixed aerobes and anaerobes create a microenvironment of low O₂ tension and low pH; anaerobes produce hydrogen and carbon dioxide gas (explaining crepitus) via fermentation
- Vascular thrombosis - Endotoxins and exotoxins trigger fibrin thrombi in dermal and subcutaneous vessels → ischemia → nutrient supply is cut off from host immune cells while bacteria continue to proliferate in necrotic tissue
- Progressive necrosis - Ischemia leads to coagulation necrosis of subcutaneous fat, fascia, and overlying dermis → the characteristic gray-blue/purplish discoloration
Histopathology
Biopsy shows:
- Gangrene of subcutaneous tissue with spread along fascial planes
- Fibrinoid necrosis in the media of vessels passing through destroyed fascia
- Fibrin thrombi in dermal vessels
- Coagulation necrosis of epidermis, dermis, and appendages
- Dense neutrophil and mononuclear infiltration in upper dermis
- Numerous bacteria visible on Gram stain
Systemic Sepsis
Bacterial toxins (especially streptococcal superantigens) activate a massive cytokine cascade → SIRS → septic shock. This patient already has septic physiology (BP 80 systolic, HR 140, RR 30, temp 40°C).
- Dermatology 2-Volume Set 5e, p. 1529
- Fitzpatrick's Dermatology, p. 2800-2801
3. Microbiology - Classification
Type I (Polymicrobial) - Most Likely Here
At least one anaerobe (Bacteroides, Peptostreptococcus, Clostridium) plus facultative anaerobes (streptococci, E. coli, Enterobacteriaceae). Accounts for ~60% of cases. Common in diabetics, post-trauma.
Type II (Monomicrobial)
Most often Group A Streptococcus (S. pyogenes) alone or with S. aureus. More aggressive; associated with streptococcal toxic shock syndrome.
Type III
Gram-negative marine organisms: Vibrio vulnificus (seawater injuries), Aeromonas hydrophila (freshwater). High mortality and amputation rates.
Type IV
Fungal (zygomycosis/mucormycosis) in immunocompromised patients.
- Dermatology 2-Volume Set 5e, p. 5176
4. Investigations
Bedside / Immediate
| Investigation | Rationale |
|---|---|
| Vital signs + oxygen saturation | Confirm sepsis/septic shock severity |
| Blood glucose | Diabetic control; hyperglycemia worsens prognosis |
| Capillary refill, limb perfusion | Assess vascular compromise |
Laboratory (Send Immediately)
| Test | Findings in NF |
|---|---|
| CBC | Leukocytosis (WBC >15,000) or leukopenia; left shift with bands |
| CRP | Markedly elevated (>150 mg/L) |
| Serum sodium | Hyponatremia (<135 mEq/L) - seen in NF |
| Serum creatinine/urea | Elevated (renal impairment from sepsis/DM) |
| Serum glucose | Hyperglycemia |
| Serum lactate | Elevated (>2 mmol/L indicates tissue hypoperfusion) |
| Coagulation screen (PT/aPTT/D-dimer) | DIC screening |
| Creatine phosphokinase (CPK) | Elevated in NF (distinguishes from cellulitis) |
| Blood cultures (×2) | Before antibiotics - identify causative organisms |
| LFTs, albumin | Baseline organ function and nutritional status |
| ABG | Metabolic acidosis, respiratory status |
The LRINEC Score (Laboratory Risk Indicator for Necrotizing Fasciitis)
A scoring tool based on routinely available labs. High specificity but lower sensitivity - do NOT use to exclude NF.
| Variable | Criteria | Points |
|---|---|---|
| CRP (mg/L) | ≥150 | +4 |
| WBC (×10³/µL) | 15-25 | +1; >25 |
| Hemoglobin (g/dL) | 11-13.5 | +1; <11 |
| Sodium (mmol/L) | <135 | +2 |
| Creatinine (µmol/L) | >141 | +2 |
| Glucose (mmol/L) | >10 | +1 |
Score ≥6 = high risk; ≥8 = strong predictor. This patient likely scores very high.
Imaging
| Modality | Findings |
|---|---|
| Plain X-ray (right thigh) | Gas in soft tissues (present in minority of cases; 57% sensitivity); rules out fracture/foreign body |
| CT scan (with contrast) | Best for demonstrating extent of gas, fascial plane involvement, and guiding surgical planning; shows "dirty fascia sign" |
| MRI | Gold standard for tissue involvement depth; shows high signal intensity along fascial planes on T2/STIR; helps differentiate from cellulitis - but do NOT delay surgery for MRI in a septic patient |
| Point-of-care ultrasound | Can show thickened fascia and subcutaneous gas (cobblestone sign) - rapid bedside tool |
Intraoperative "Gold Standard" Diagnosis
Surgical exploration remains the definitive diagnostic step. Findings specific to NF:
- Easy dissection ("finger sweep test") along fascial planes with no resistance
- Gray-dusky edematous necrotic fascia
- Thin, stringy brown ("dishwater") exudate
- Lack of bleeding at fascial level
- Gram stain of necrotic tissue - polymicrobial organisms
Wound/Tissue Specimens
-
Wound swab for Gram stain and culture + sensitivity
-
Tissue biopsy from operative specimens for histopathology and culture
-
Anaerobic cultures
-
Dermatology 2-Volume Set 5e, p. 5208
-
Fitzpatrick's Dermatology, p. 2801-2802
-
Rosen's Emergency Medicine, p. 2402
5. Management
This is a TIME-CRITICAL emergency. The patient has septic shock + NF = immediate surgical and ICU intervention.
A. Resuscitation (Simultaneous with Surgery Prep)
- IV access - large-bore ×2, central line
- Fluid resuscitation - IV crystalloids (0.9% NS or Ringer's lactate); target MAP ≥65 mmHg
- Vasopressors - Norepinephrine if fluid-unresponsive (septic shock)
- Oxygen - high-flow O₂; intubation if needed
- Foley catheter - monitor urine output (target ≥0.5 mL/kg/hr)
- Glycemic control - insulin infusion; target glucose 140-180 mg/dL in ICU
- Blood products - FFP, platelets if DIC develops
B. Antibiotics - Broad-Spectrum Empiric (Start Immediately, Before OR)
The empirical regimen must cover streptococci, staphylococci (including MRSA), Gram-negative bacilli, and anaerobes:
| Regimen | Components |
|---|---|
| First-line | Vancomycin (MRSA coverage) + Piperacillin-tazobactam (broad Gram-negative + anaerobe) |
| Alternative | Vancomycin + Carbapenem (meropenem/imipenem) |
| Alternative | Vancomycin + Ceftriaxone + Metronidazole |
| Penicillin allergy | Ciprofloxacin + Metronidazole or Clindamycin |
Add Clindamycin to any regimen when Group A Streptococcus is suspected - it inhibits toxin production by blocking ribosomal protein synthesis (even when penicillin has reduced efficacy in the stationary growth phase).
Antibiotics are adjunctive to surgery - they do not penetrate the avascular necrotic tissue. Narrow therapy once culture and sensitivity results return.
C. Surgical Debridement - The Definitive Treatment
Urgent operative debridement is the mainstay of treatment and must not be delayed.
Steps:
- Wide surgical exploration of the involved fascial plane
- Excision of all necrotic tissue until healthy, bleeding tissue is encountered at wound margins
- "Finger sweep test" - probe fascial planes; NF shows easy blunt dissection
- Multiple tissue samples for culture/histopathology
- Wound left open (do not close a contaminated wound)
- Re-exploration at 24-48 hours - mandatory "second-look" operation; further debridement almost always required
- Amputation of the limb may be necessary to control the source if fascial spread is uncontrollable or limb viability is lost
D. Adjunctive Therapies
| Therapy | Role |
|---|---|
| Hyperbaric oxygen (HBO) | Controversial; may benefit a subset with anaerobic Gram-negative NF; increases tissue O₂ tension, enhances neutrophil killing. Never delay surgery for HBO |
| Intravenous immunoglobulin (IVIg) | May be useful in severe Group A Streptococcal NF with toxic shock; however, a randomized placebo-controlled trial failed to show benefit in ICU patients with necrotizing soft tissue infections |
| Nutritional support | Enteral feeding started early; critical for post-op wound healing |
| Wound care | Negative pressure wound therapy (VAC) after debridement accelerates healing |
| Reconstructive surgery | Split-thickness skin grafting and/or flap coverage once wound is clean and patient is stable |
E. Wound Closure and Reconstruction
After serial debridements and clean wound bed confirmed, reconstruction options include:
-
Split-thickness skin grafts (STSG)
-
Local or free muscle flaps for deep defects
-
Dermatology 2-Volume Set 5e, p. 5211-5213
-
Fitzpatrick's Dermatology, p. 2802-2803
-
Rosen's Emergency Medicine, p. 2402
6. Complications
Early Complications
| Complication | Mechanism |
|---|---|
| Septic shock | Massive bacteremia + cytokine storm → refractory hypotension |
| Disseminated Intravascular Coagulation (DIC) | Endotoxins activate coagulation cascade → consumption coagulopathy |
| Multi-organ dysfunction syndrome (MODS) | Hypoperfusion + direct toxin effects → acute kidney injury, hepatic failure, ARDS |
| Acute Respiratory Distress Syndrome (ARDS) | Cytokine-mediated lung injury |
| Limb loss / Amputation | Required in ~26-50% of cases with extensive limb involvement |
| Wound dehiscence | Large fasciotomy wounds left open |
| Streptococcal Toxic Shock Syndrome (STSS) | Streptococcal superantigens → massive T-cell activation → cytokine storm |
Late Complications
| Complication | Details |
|---|---|
| Extensive scarring and disfigurement | Large surgical defects after debridement |
| Contracture | Over joints if skin grafts placed near flexion surfaces |
| Functional disability | Loss of muscle/fascia function |
| Recurrence | Rare if adequately debrided |
| Psychological complications | PTSD, depression following prolonged ICU stay and disfigurement |
| Chronic wound / osteomyelitis | If bone involved |
Mortality
Mortality rates range 20-60%. In this patient, prognostic risk factors include:
-
Diabetes mellitus with likely vascular compromise
-
Septic shock at presentation (BP 80 systolic, HR 140)
-
Delay in diagnosis (3 days)
-
Elevated creatinine/lactate (anticipated)
-
Dermatology 2-Volume Set 5e, p. 5183
-
Fitzpatrick's Dermatology, p. 2800, 2803
Summary Table
| Domain | Key Points |
|---|---|
| Diagnosis | Type I polymicrobial NF; clinical diagnosis confirmed intraoperatively |
| Pathogenesis | Fascial plane spread, vascular thrombosis, anaerobic gas production, systemic toxin release |
| Microbiology | Mixed: streptococci, S. aureus, E. coli, Bacteroides, Clostridium |
| Investigations | LRINEC labs, blood cultures, CT/MRI, intraoperative tissue cultures |
| Treatment | Immediate surgical debridement + broad-spectrum antibiotics + ICU resuscitation |
| Complications | Septic shock, DIC, MODS, limb loss; mortality 20-60% |
Clinical Pearl: "When in doubt, cut it out." Any suspicion of NF in a septic diabetic patient after trauma mandates immediate surgical exploration. A negative exploratory incision is far safer than a delayed diagnosis. The LRINEC score can risk-stratify but must never be used to exclude NF.
Sources:
- Dermatology 2-Volume Set 5e (Griffiths et al.), pp. 1528-1530
- Fitzpatrick's Dermatology (McGraw-Hill), pp. 2799-2804
- Rosen's Emergency Medicine, p. 2402
- Goldman-Cecil Medicine, Streptococcal NF chapter
This is a shared conversation. Sign in to Orris to start your own chat.