Ligaments of uterus
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
I have comprehensive, well-illustrated content from Gray's Anatomy for Students, Color Atlas of Human Anatomy Vol. 2, and Campbell-Walsh-Wein Urology. Here is the full answer:
Ligaments of the Uterus
The uterus is held in position by a combination of peritoneal folds, fibromuscular condensations, and true ligaments. They are traditionally grouped as follows:
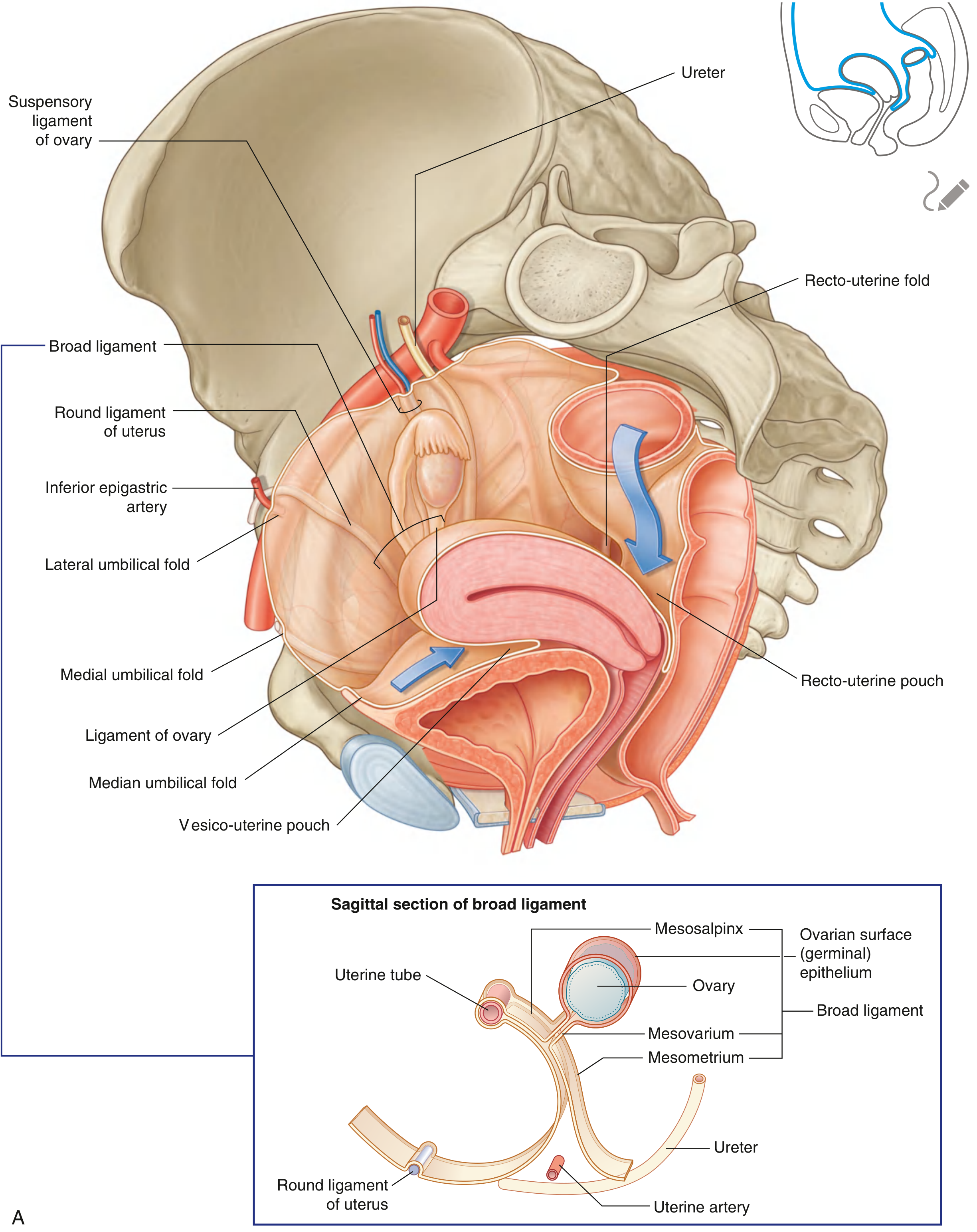
1. Broad Ligament
- A sheet-like, coronal fold of peritoneum extending from the lateral margins of the uterus to the lateral pelvic walls.
- Contains connective tissue, vessels, nerves, and encloses the uterine tube in its superior margin.
- The uterine arteries and ureters are closely related to its base - the uterine artery crosses above the ureter at this level ("water under the bridge").
- Has three named parts:
Part Location Contents Mesometrium Largest - from uterine body to lateral pelvic wall Uterine vessels, nerves Mesosalpinx Superior free margin Suspends the uterine (Fallopian) tube Mesovarium Posterior extension Attaches to and suspends the ovary
2. Round Ligament of the Uterus
- A fibromuscular cord arising from the uterine horn, just anterior and inferior to the fallopian tube.
- Runs anterolaterally through the inguinal canal (acquiring the same fascial coverings as the spermatic cord), exits through the superficial inguinal ring, and ends as fibrous strands in the connective tissue of the labium majus.
- Embryological origin: the long distal part of the gubernaculum (the structure that guides gonadal descent). The short proximal part of the gubernaculum becomes the ligament of the ovary (ovarian ligament).
- It does NOT provide significant uterine support; its main clinical relevance is as a landmark in inguinal/pelvic surgery.
3. Uterosacral Ligaments (Sacrouterine / Rectouterine Ligaments)
- Condensations of subperitoneal connective tissue and smooth muscle (rectouterinus muscle) that run from the posterolateral cervix and upper vagina to the posterolateral pelvic wall (sacrum/greater sciatic foramen, at S2-S4 level).
- They form the recto-uterine folds, which bound the recto-uterine pouch (pouch of Douglas) on each side.
- Composed of fibrous tissue, smooth muscle, and autonomic nerve fibers from the inferior hypogastric plexus.
- Clinically important: the ureter passes just lateral to the anterior portion of the uterosacral ligament near the cervix; they are used as anchoring structures in apical vaginal suspension surgeries (e.g. sacrospinous fixation, McCall culdoplasty).
4. Cardinal Ligament (Mackenrodt's / Transverse Cervical Ligament)
- A condensation of endopelvic/parametrial connective tissue at the base of the broad ligament, running from the cervix and upper vagina to the lateral pelvic wall.
- Often considered the most important structural support of the uterus - it anchors the cervix and resists downward displacement.
- Contains the major blood vessels from the internal iliac artery (uterine artery), lymphatics, and autonomic nerves.
- Fuses posteriorly with the uterosacral ligaments.
- Defects or weakness lead to uterine prolapse.
5. Ligament of the Ovary (Ovarian Ligament)
- A fibromuscular cord connecting the medial pole of the ovary to the uterine horn, just posterior and inferior to the uterine tube.
- Runs within the posterior margin of the mesovarium.
- Embryological origin: proximal part of the gubernaculum (same origin as round ligament - they are in continuity).
6. Suspensory Ligament of the Ovary (Infundibulopelvic Ligament / IP Ligament)
- A peritoneal fold covering the ovarian vessels (ovarian artery, vein, lymphatics, and nerves) as they travel from the lateral pelvic wall to the superior pole of the ovary.
- Lies posterior to the broad ligament.
- Surgically important: ligating it during oophorectomy risks the ovarian vessels and the nearby ureter (which passes beneath it).
7. Pubocervical Ligament (Anterior Ligament)
- Connects the cervix anteriorly to the posterior aspect of the pubic symphysis.
- Part of the endopelvic fascia; supports the bladder base and anterior vaginal wall.
Summary Table
| Ligament | Type | Attachment | Key Content/Note |
|---|---|---|---|
| Broad | Peritoneal fold | Uterus → lateral pelvic wall | Mesometrium, mesosalpinx, mesovarium |
| Round | Fibromuscular cord | Uterine horn → labium majus (via inguinal canal) | Gubernaculum remnant; not a true support |
| Uterosacral | Fascial condensation | Cervix → sacrum (S2-S4) | Bounds pouch of Douglas; apical support |
| Cardinal (Mackenrodt's) | Fascial condensation | Cervix → lateral pelvic wall | Main cervical support; contains uterine a. |
| Ligament of ovary | Fibromuscular cord | Ovary → uterine horn | Gubernaculum remnant |
| Suspensory (IP) | Peritoneal fold | Ovary → lateral pelvic wall | Contains ovarian vessels |
| Pubocervical | Fascial condensation | Cervix → pubis | Anterior support |
Important Clinical Points
- True uterine support comes mainly from the pelvic floor muscles (levator ani) and the cardinal + uterosacral ligament complex - not the broad or round ligaments.
- "Water under the bridge": Uterine artery crosses over the ureter at the base of the broad ligament. The ureter is at risk during hysterectomy when clamping these ligaments.
- Uterine prolapse results from weakening of the cardinal and uterosacral ligaments (often after childbirth or with aging).
- Endometriosis commonly involves the uterosacral ligaments, causing deep dyspareunia and cyclic pelvic pain.
- Ectopic pregnancy in the broad ligament (broad ligament/intraligamentous ectopic) can cause massive intraperitoneal hemorrhage.
- The round ligament can be a source of pain in pregnancy (round ligament pain) as it stretches with the growing uterus.
Sources: Gray's Anatomy for Students, pp. 355-356, 561; Color Atlas of Human Anatomy Vol. 2 (Internal Organs), pp. 460-461; Campbell-Walsh-Wein Urology, p. 3796-3800
This is a shared conversation. Sign in to Orris to start your own chat.