What is asd pda and vsd devices how they are deployed and how to measure septal wall hole size to deploy appropriate devise ???
Reading File
Finding Sources
Finding Sources
Searching the Web
ASD VSD PDA occluder devices deployment technique septal defect sizing 2024
Finding Sources
Finding Sources
Finding Sources
Searching Images
ASD VSD PDA device closure deployment echocardiography sizing
Reading File
Finding Sources
Loading Image
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information from Braunwald's Heart Disease and the Clinical Echocardiography textbook. Let me compile the full answer:
ASD, VSD, and PDA Device Closure: Devices, Deployment, and Defect Sizing
Overview
These are the three most common congenital heart defects (CHDs) amenable to transcatheter (percutaneous) device closure — avoiding open-heart surgery. All rely on a catheter introduced via the femoral vein/artery, guided by echocardiography (TEE/ICE) and fluoroscopy.
1. Atrial Septal Defect (ASD) Closure
What is an ASD?
An opening in the interatrial septum causing left-to-right shunting, leading to RV dilation and, if left unrepaired, pulmonary hypertension by the sixth decade. Incidence: 56–100 per 100,000 live births.
Types amenable to device closure:
- Secundum ASD — most common, located in the fossa ovalis region ✅ ideal for transcatheter
- Patent Foramen Ovale (PFO) — transcatheter closure FDA-approved for cryptogenic stroke ✅
- Superior sinus venosus ASD — now treated with covered stent in SVC-RA junction
- Primum ASD / Inlet ASD — not amenable; require surgical repair
ASD Closure Devices
| Device | Key Features |
|---|---|
| Amplatzer Septal Occluder (ASO) (Abbott) | Nitinol mesh, self-centering, dual discs with central waist filled with Dacron polyester. Sizes 4–40 mm waist diameter |
| Amplatzer Cribriform | No waist — not self-centering; ideal for multifenestrated defects and small central defects with satellite holes |
| Amplatzer PFO Occluder | Two nitinol discs, RA disc larger than LA disc, short fixed waist. FDA-approved for cryptogenic stroke |
| GORE Cardioform Septal Occluder (GSO) | 5-wire nitinol frame + ePTFE membrane. Non-self-centering. Closes defects up to 18 mm |
| GORE Cardioform ASD Occluder (GCA) | ePTFE-covered nitinol; "intra-disc occluder" expands to fit defect shape. Sizes 27–48 mm; treats defects 8–35 mm. No erosion risk — safe with deficient retro-aortic rim |
ASD Sizing — Critical Steps
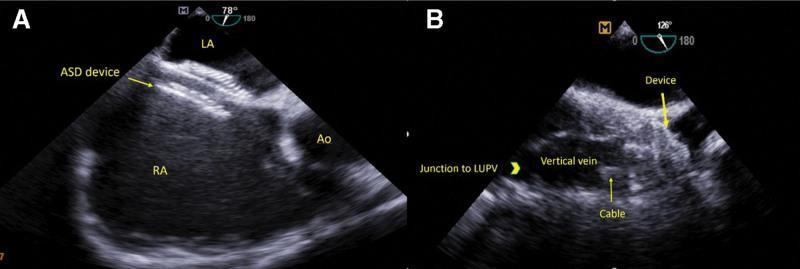
Step 1 — Echocardiographic (static) measurement:
- TEE or TTE measures the ASD diameter in multiple planes (bicaval view, short-axis view, 4-chamber view)
- 3D echocardiography provides the best spatial assessment of defect shape and rim adequacy
- Rim assessment is essential: a rim <5 mm ("deficient rim") — especially the retro-aortic rim — complicates device placement and increases erosion risk with the ASO
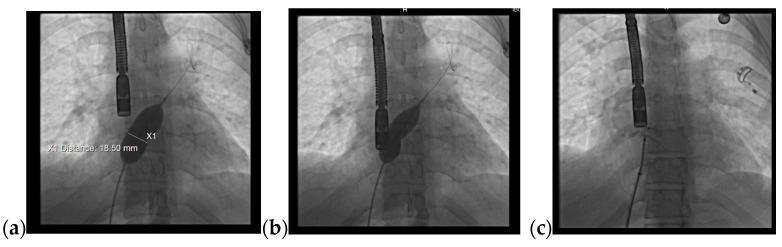
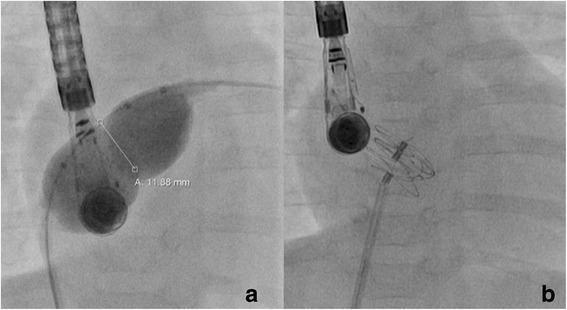
Step 2 — Balloon sizing (Stop-Flow Technique):
- A compliant sizing balloon (e.g., NuMed Sizing Balloon) is advanced across the ASD via the delivery sheath
- The balloon is inflated with dilute contrast under TEE/fluoroscopic guidance
- Inflation continues until the left-to-right shunt stops completely (stop-flow endpoint) — verified by color Doppler
- The stretched diameter of the balloon at this exact point is measured fluoroscopically
- ⚠️ Do NOT overinflate beyond cessation of shunt — overinflation overstates the true defect size and risks erosion
Step 3 — Device size selection:
- ASO: Choose device = same size as stop-flow diameter, or at most 1 size larger
- Maximum: Device ≤ 1.5× the echocardiographic (static) ASD diameter — never exceed this to avoid erosion
- Deficient retro-aortic rim (<5 mm): Higher erosion risk with ASO. Consider GORE Cardioform (no erosion reported) or specialized techniques
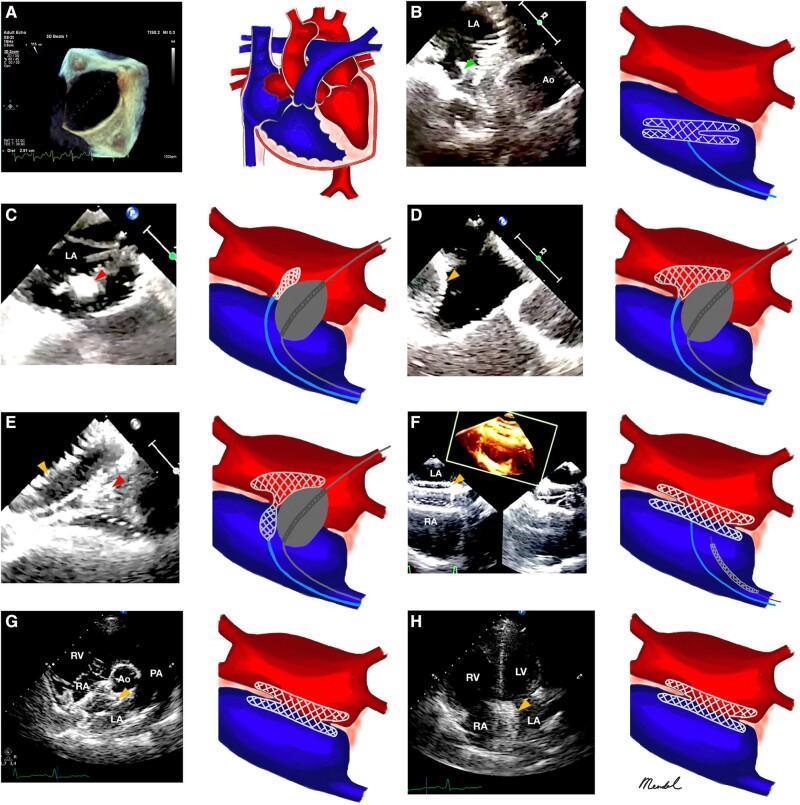
ASD Deployment Steps (Amplatzer ASO Technique)
- Venous access via right femoral vein
- Transseptal puncture (if not crossing through defect directly)
- Position TorqVue long sheath in left upper pulmonary vein (stable position)
- Size the defect (balloon stop-flow technique as above)
- Load the device into loader, connect to delivery cable (screwthread mechanism)
- Advance device through sheath into left atrium
- Open LA disc in left atrium, pull back to engage the septum
- Retract sheath to open RA disc in right atrium
- Perform "wiggle test" — push-pull maneuver under TEE/fluoroscopy to confirm stability
- Assess position: device must not impinge on SVC, pulmonary veins, mitral valve, or aorta
- If position stable → release device by counterclockwise rotation of delivery cable
- Confirm closure with color Doppler TEE
2. Ventricular Septal Defect (VSD) Closure
What is a VSD?
The most common congenital heart defect. Defects range from tiny pinholes to near-absence of the septum. Shunt magnitude depends on ventricular outflow resistance.
VSD locations:
| Type | Transcatheter Suitability |
|---|---|
| Muscular | ✅ Ideal for device closure |
| Perimembranous | ⚠️ Controversial — risk of complete AV block (2–6%) |
| Post-infarct | ✅ FDA-approved (Amplatzer Post-Infarct device) |
| Traumatic / Post-op residual | ✅ Device closure is reasonable alternative |
| Inlet | ❌ Not amenable — no circumferential tissue rim |
VSD Closure Devices
| Device | Key Features |
|---|---|
| Amplatzer Muscular VSD Occluder | Larger discs, short waist. For congenital muscular VSDs |
| Amplatzer Post-Infarct Muscular VSD Occluder | Larger discs + longer 10 mm waist to accommodate thicker adult interventricular septum. FDA-approved for post-MI VSD |
| Amplatzer Septal Occluder (off-label) | Sometimes used for post-infarct VSDs |
VSD Sizing and Deployment
Sizing:
- 2D/3D TEE in multiple views: RV inflow-outflow, parasternal short axis, apical 4-chamber
- Measure the defect diameter directly — balloon sizing not routinely needed for most VSDs (unlike ASD)
- Device size selected to be 1–2 mm larger than the measured defect
- Confirm adequate rim from aortic valve, TV, and MV
Deployment (Muscular VSD — Retrograde Approach):
- Femoral venous + arterial access
- Cross the VSD from the LV side (arterial, retrograde) with a wire
- Establish arteriovenous wire loop (snared from RV and exteriorized via femoral vein)
- Advance long delivery sheath from femoral vein, crossing VSD into LV
- Open LV disc in left ventricle
- Pull back to appose the septum
- Open RV disc in right ventricle
- Wiggle test, TEE confirmation of position
- Ensure no AV valve impingement, no aortic regurgitation
- Release device
Complications specific to VSD closure:
- Complete AV block (most feared — perimembranous VSDs)
- Aortic regurgitation (from device impinging on aortic valve)
- Tricuspid regurgitation
- Device embolization
3. Patent Ductus Arteriosus (PDA) Closure
What is a PDA?
Failure of the ductus arteriosus to close after birth. Causes left-to-right shunt (aorta → pulmonary artery), pulmonary overcirculation, LV dilation. Large PDAs → heart failure, atrial arrhythmias, pulmonary hypertension. Site for infective endarteritis.
PDA Closure Devices
| Device | PDA Type | Key Features |
|---|---|---|
| Amplatzer Duct Occluder I (ADO-I) | Conical/ampullary PDA | Nitinol mesh + Dacron polyester. Funnel-shaped with retention disc on aortic side. 6–9 Fr sheath. Sizes 3.5–14 mm |
| Amplatzer Duct Occluder II (ADO-II) | Any orientation | Symmetric retention skirts — can be placed antegrade or retrograde. No polyester fill (tighter nitinol weave) |
| Amplatzer Vascular Plug II (AVP-II) | Long tubular ducts | Low profile, sizes 3–22 mm. Works when duct is long enough to prevent LPA/aortic obstruction |
| Amplatzer Vascular Plug IV (AVP-IV) | Tortuous anatomy | Even lower profile, sizes 4–8 mm, slightly longer |
| Nit-Occlud (PFM Medical) | Small/moderate PDAs | Single nitinol wire coil in funnel shape. Delivered via 4 Fr catheter with controlled-release mechanism |
| Simple/detachable coils | Small PDAs | After crossing, simple or detachable coils reliably occlude small ducts |
PDA Sizing and Deployment
Sizing:
- Angiography (aortogram in lateral projection) is the gold standard: measures minimum PDA diameter, length, and shape (Type A–E Krichenko classification)
- TTE/TEE supplementary: measures minimum diameter, LPA/aortic end diameter
- Device size selected: ≥1–2 mm larger than the narrowest (minimum) PDA diameter
- For ADO-I: device diameter at pulmonary end should match the PDA minimum diameter +1–2 mm; the retention disc sits in the aortic ampulla
Deployment (Antegrade — ADO-I Standard Technique):
- Right femoral venous access; advance catheter across PDA from PA to descending aorta
- Establish guidewire in descending aorta
- Advance long delivery sheath into descending aorta
- Screw device onto delivery cable clockwise; load into sheath
- Advance device into descending aorta → retract sheath to open retention disc in aortic ampulla
- Pull sheath + cable back as one unit until retention disc is snug at aortic end of ampulla
- Retract sheath further into PA → tubular body and PA disc open within the duct
- Confirm position angiographically (no LPA or aortic obstruction) and by echocardiography
- Check for residual shunting with color Doppler
- Release device (counterclockwise rotation)
Overall PDA closure success rate: ~94%. Serious adverse events are rare.
Summary: Sizing Rules at a Glance
| Defect | Sizing Method | Device Size Selection |
|---|---|---|
| ASD | Balloon stop-flow (stretched diameter) + TEE static measurement | = Stop-flow diameter (max 1 size larger); never >1.5× static echo diameter |
| VSD | 2D/3D TEE direct measurement | 1–2 mm > measured defect diameter |
| PDA | Lateral aortogram minimum diameter | ≥1–2 mm > minimum (narrowest) PDA diameter |
Imaging Guidance During All Procedures
| Modality | Role |
|---|---|
| TEE | Primary real-time guidance — confirms device position, rules out impingement, checks residual shunt |
| ICE (Intracardiac Echo) | Alternative to TEE — avoids general anesthesia; growing use in adults |
| TTE | Pre/post procedure assessment; can be used in children |
| Fluoroscopy | Device delivery, balloon sizing measurement, angiography (especially for PDA) |
| 3D Echo | Best for defect morphology, rim assessment, device orientation |
Sources: Braunwald's Heart Disease, 12th Ed., Chapter 83 "Transcatheter Therapies for Congenital Heart Disease"; Textbook of Clinical Echocardiography, Chapter 17; Abbott/Amplatzer device instructions for use
This is a shared conversation. Sign in to Orris to start your own chat.