Discuss recent WHO classification of Lung tumours. Describe clinical features, morphology and diagnostic approach in lung tumours
Reading File
Finding Sources
Finding Sources
Searching PubMed
WHO classification lung tumors 2021
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have comprehensive material from multiple authoritative textbooks. Let me compose the complete, detailed answer.
WHO Classification of Lung Tumours: Clinical Features, Morphology, and Diagnostic Approach
1. WHO Classification of Lung Tumours (2021, 5th Edition)
The WHO 2021 classification builds on the 2015 edition and places greater emphasis on molecular/genetic underpinning, integration of immunohistochemistry (IHC), and distinct treatment-relevant categories. The classification of malignant epithelial tumours (simplified) is as follows:
Malignant Epithelial Tumours (WHO 2021)
| Category | Subtypes |
|---|---|
| Adenocarcinoma | Acinar, papillary, micropapillary, solid, lepidic-predominant; invasive mucinous; colloid; fetal; enteric; adenocarcinoma in situ (AIS); minimally invasive adenocarcinoma (MIA) |
| Squamous cell carcinoma | Keratinizing; non-keratinizing; basaloid squamous cell carcinoma; squamous cell carcinoma in situ |
| Large cell carcinoma | Diagnosis of exclusion (no adenomatous, squamous or neuroendocrine differentiation) |
| Neuroendocrine tumours | Small cell carcinoma (combined SCLC); Large cell neuroendocrine carcinoma (LCNEC); Typical carcinoid; Atypical carcinoid; Diffuse idiopathic pulmonary neuroendocrine cell hyperplasia (DIPNECH) |
| Adenosquamous carcinoma | Mixed glandular + squamous differentiation |
| Sarcomatoid carcinoma | Pleomorphic, spindle cell, giant cell, carcinosarcoma, pulmonary blastoma |
| Salivary gland-type tumours | Mucoepidermoid carcinoma; adenoid cystic carcinoma; epithelial-myoepithelial carcinoma |
| Other | NUT carcinoma, thoracic SMARCA4-deficient undifferentiated tumour |
Benign Lung Neoplasms (WHO)
| Category | Examples |
|---|---|
| Papillomas | Squamous cell (exophytic, inverted), mixed squamous |
| Adenomas | Sclerosing pneumocytoma, alveolar adenoma, papillary adenoma, mucinous cystadenoma |
| Mesenchymal | Pulmonary hamartoma, chondroma, PEComa, teratoma |
Source: Mulholland & Greenfield's Surgery, 7e; Robbins & Kumar Basic Pathology
Key changes in 2021 vs 2015:
- Neuroendocrine tumours are now grouped as one family spanning low-grade (carcinoids) through high-grade (SCLC, LCNEC)
- The term "bronchioloalveolar carcinoma (BAC)" is abolished; replaced by AIS and MIA
- SMARCA4-deficient tumours and NUT carcinoma added as new entities
- Greater integration of molecular biomarkers into classification
2. Clinical Features of Lung Tumours
Epidemiology and Risk Factors
- Lung cancer accounts for ~45,000 new cases/year in the UK; 60% die within 1 year; only 15% survive 5 years
- Cigarette smoking is the dominant risk factor, accounting for 85-95% of all cases
- The risk is 60 times higher in heavy smokers (2 packs/day x 20 years) versus non-smokers
- Women are more susceptible to carcinogens in tobacco smoke than men
- Other risks: radon, asbestos, radioactive ore/chromium mining, atmospheric pollution
- About 10-15% of lung cancers occur in never-smokers, with EGFR mutations more common in this group (especially women, East Asian populations)
Intrathoracic Symptoms
Endobronchial/local disease:
- Cough (most common), which may be chronic and changing in character
- Haemoptysis - occurs in central tumours (squamous most common)
- Wheeze or stridor - from airway compression
- Dyspnoea - from atelectasis, effusion, or lymphangitic spread
- Post-obstructive pneumonia - recurrent or non-resolving pneumonia
Regional intrathoracic spread:
- Hoarseness - recurrent laryngeal nerve palsy (left nerve more often, long intrathoracic course)
- Dysphagia - oesophageal compression
- Superior vena cava (SVC) syndrome - facial/arm oedema, venous distension, plethora; more common with SCLC and right-sided lesions
- Horner's syndrome - enophthalmos, ptosis, miosis, anhidrosis from cervical sympathetic plexus invasion
- Pancoast (superior sulcus) syndrome - apical tumour invading C8/T1/T2 nerves causing shoulder pain radiating in ulnar distribution + Horner's syndrome + rib destruction
- Phrenic nerve palsy - elevated hemidiaphragm
- Malignant pleural effusion - pain, dyspnoea
- Pericardial involvement - tamponade, arrhythmias
Constitutional symptoms:
- Anorexia, weight loss (>10 lbs is a red-flag feature)
- Weakness, fever, night sweats
Extrathoracic Metastatic Disease
At autopsy, extrathoracic spread is found in:
-
50% of squamous cell carcinoma
- 80% of adenocarcinoma and large cell carcinoma
-
95% of SCLC
Common metastatic sites and their manifestations:
| Site | Symptoms |
|---|---|
| Brain | Headache, nausea/vomiting, seizures, focal neurologic deficits |
| Bone | Pain, pathologic fractures, spinal cord compression |
| Liver | Hepatomegaly, right upper quadrant pain, jaundice |
| Adrenal | Usually asymptomatic |
| Bone marrow | Cytopenias, leukoerythroblastic picture |
Paraneoplastic Syndromes
These may antedate diagnosis and are clinically important:
| Hormone/Mediator | Syndrome | Associated Tumour Type |
|---|---|---|
| ADH | SIADH - hyponatraemia | SCLC (predominantly) |
| ACTH | Cushing syndrome | SCLC (predominantly) |
| PTHrP, PGE2 | Hypercalcaemia | Squamous cell carcinoma (predominantly) |
| Calcitonin | Hypocalcaemia | Various |
| Gonadotropins | Gynaecomastia | Various |
| Serotonin/bradykinin | Carcinoid syndrome | Carcinoid tumours |
Other paraneoplastic manifestations:
- Lambert-Eaton myasthenic syndrome (LEMS) - autoantibodies against presynaptic voltage-gated calcium channels; proximal muscle weakness; associated with SCLC
- Hypertrophic pulmonary osteoarthropathy - periosteal new bone formation + clubbing of fingers; common with adenocarcinoma
- Peripheral neuropathy - purely sensory
- Acanthosis nigricans (dermatologic)
- Trousseau syndrome - hypercoagulable state with DVT/PE
Source: Robbins, Cotran & Kumar Pathologic Basis of Disease; Harrison's Principles of Internal Medicine, 22e
3. Morphology of Individual Lung Tumour Types
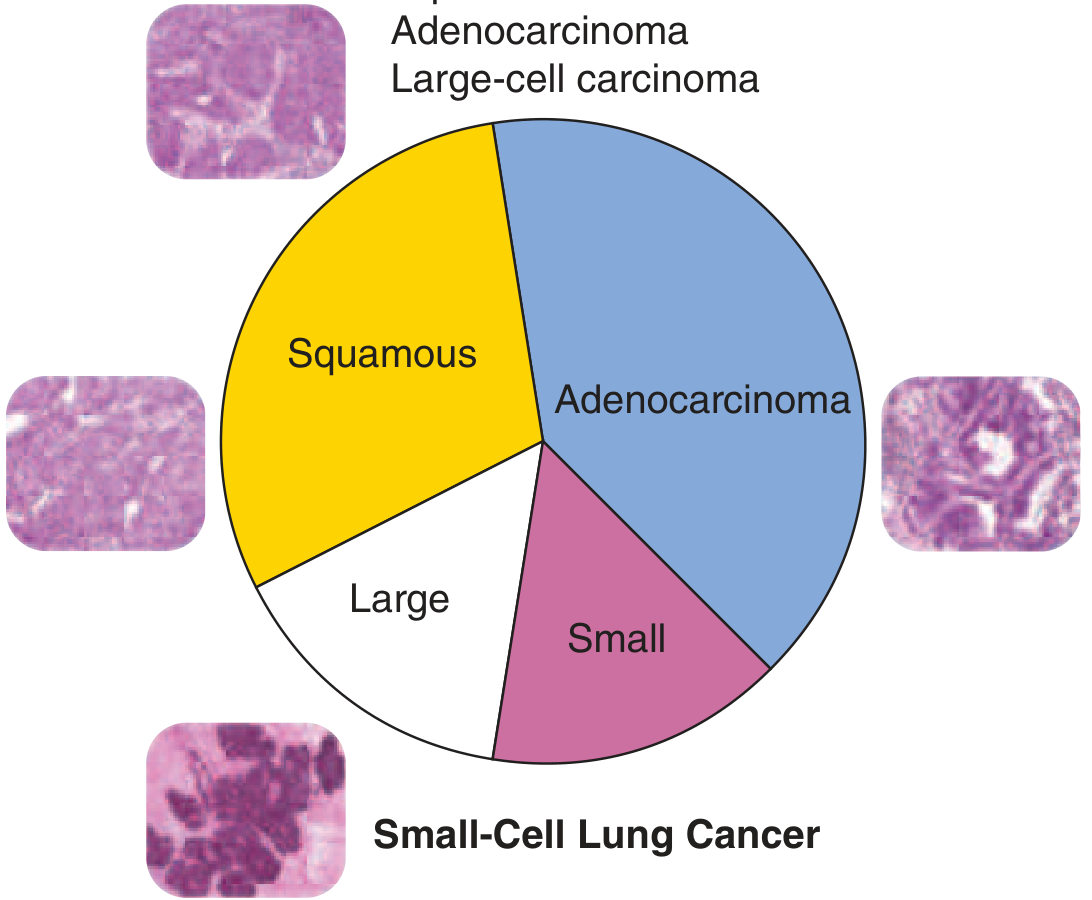
3.1 Adenocarcinoma (Most Common Overall; ~40%)
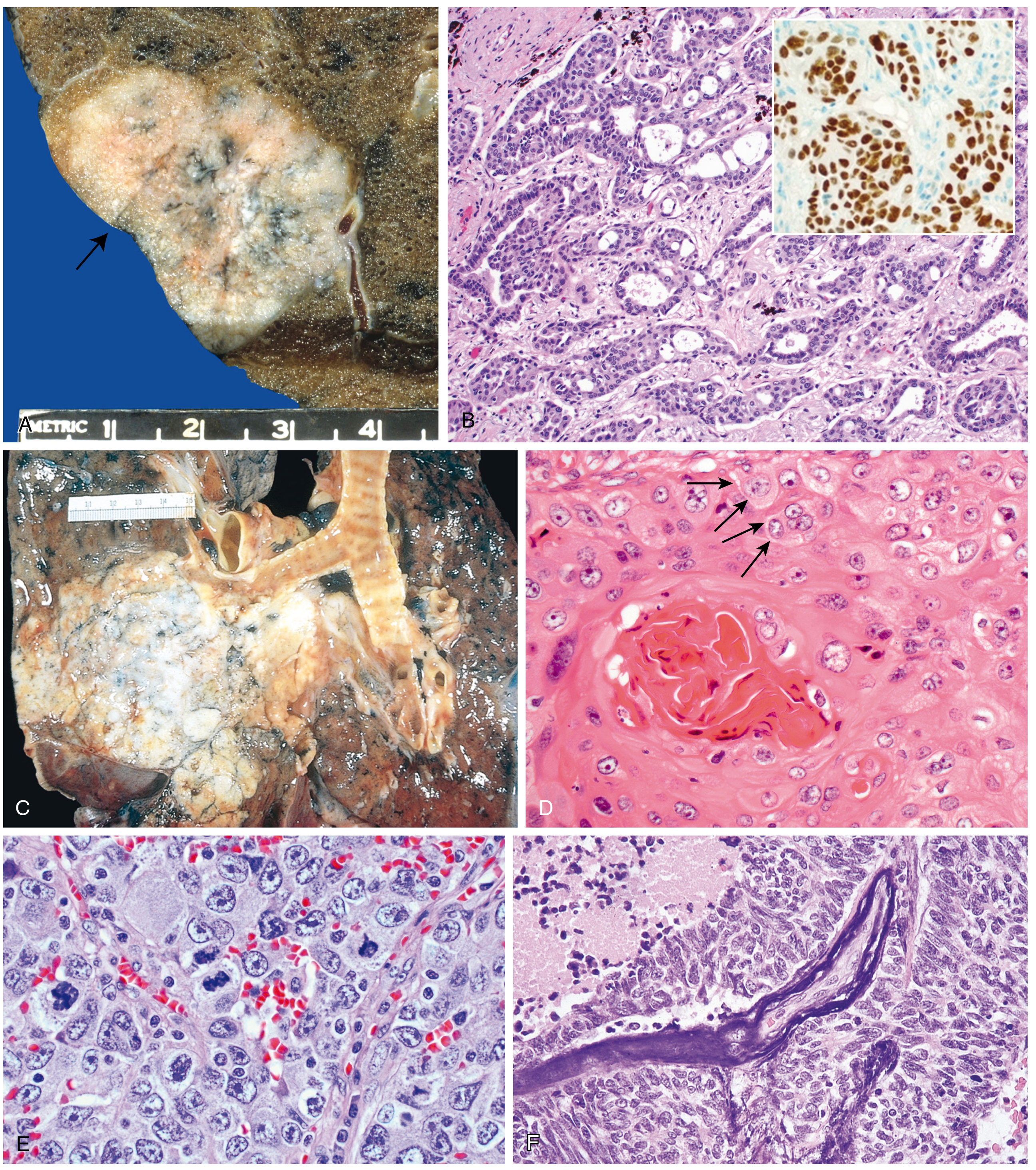
Location: Predominantly peripheral/subpleural; may be central
Gross: Often associated with central scarring (desmoplastic reaction), pleural puckering/retraction; may appear as a grey-white mass. Mucinous subtypes can show gelatinous, mucoid consistency.
Histological patterns (WHO 2021):
| Pattern | Description |
|---|---|
| Lepidic | Tumour cells grow along pre-existing alveolar walls without invasion; "spread-eagle" growth; best prognosis |
| Acinar | Gland/tubule formation with central lumina |
| Papillary | Tumour cells line fibrovascular cores |
| Micropapillary | Small papillary tufts lacking fibrovascular cores; worst prognosis among non-mucinous |
| Solid | Sheets of polygonal cells with mucin production (confirmed by histochemistry) |
| Invasive mucinous | Columnar goblet cells with abundant cytoplasmic mucin along alveoli; formerly mucinous BAC |
Pre-invasive lesions:
- Adenocarcinoma in situ (AIS): ≤3 cm, pure lepidic growth, no stromal/vascular/pleural invasion. Formerly called bronchioloalveolar carcinoma (BAC)
- Minimally invasive adenocarcinoma (MIA): ≤3 cm lepidic-predominant tumour with ≤5 mm stromal invasion
Immunohistochemistry: TTF-1 positive (nuclear), Napsin-A positive; CK7+, CK20-
Molecular markers: EGFR mutations (common in women, non-smokers, East Asians), KRAS mutations (~30%; usually smokers), ALK rearrangements (~5%), ROS1, MET, BRAF, HER2
3.2 Squamous Cell Carcinoma (~25-30%)
Location: Central/hilar, arising from bronchial epithelium (lobar/segmental bronchi)
Gross: Presents as a white-grey hilar mass invading contiguous parenchyma; cavitation is common (necrotic core); may obstruct a bronchus
Histology:
- Keratinizing subtype: Keratin pearls (concentric whorls of keratinised cells), intercellular bridges (desmosomes), individual cell keratinisation - easily recognised
- Non-keratinizing subtype: No obvious keratinization; may have only subtle IHC evidence of squamous differentiation
- Basaloid subtype: Peripheral palisading of basal-type cells; high-grade; poor prognosis
Precursor lesion: Squamous dysplasia and squamous cell carcinoma in situ (SCIS) of the bronchial mucosa
IHC: p40 and p63 positive (nuclear), CK5/6 positive; TTF-1 negative
3.3 Small Cell Carcinoma (SCLC; ~15-20%)
Location: Central, perihilar - typically a large hilar mass with extensive mediastinal involvement
Gross: Soft, pale, grey-white mass; extensive necrosis is characteristic; early mediastinal infiltration
Histology:
- Small cells (~2-3x the size of a lymphocyte) with very scant cytoplasm
- Round-to-oval nuclei with finely granular "salt-and-pepper" chromatin
- Absent or inconspicuous nucleoli
- Nuclear moulding (cells mould around each other)
- Very high mitotic rate; extensive necrosis
- Azzopardi effect: Basophilic encrustation of vascular walls by DNA from necrotic tumour cells - characteristic
- Crushed cell artefact common in biopsies
IHC (neuroendocrine markers): CD56 (NCAM), synaptophysin, chromogranin-A, INSM1 (insulinoma-associated protein 1) - all positive; TTF-1 often positive; very high Ki-67 (>60-80%)
Behaviour: Almost always metastatic at diagnosis; very chemosensitive initially but relapses; median survival in months
3.4 Large Cell Carcinoma (~10%)
Location: Usually peripheral
Gross: Large, bulky tumours with areas of necrosis and haemorrhage
Histology:
- Sheets of large, polygonal, undifferentiated cells
- No gland formation, no squamous pearls, no neuroendocrine pattern on H&E
- Large nuclei with prominent nucleoli
- Diagnosis of exclusion after IHC work-up
Note: With modern IHC, many previously called "large cell carcinoma" are now reclassified as adenocarcinoma, squamous cell carcinoma, or LCNEC
3.5 Large Cell Neuroendocrine Carcinoma (LCNEC)
- Organoid/trabecular/rosette architecture (neuroendocrine growth pattern) + large cell cytology
- IHC positive for neuroendocrine markers (CD56, synaptophysin, chromogranin)
- High mitotic rate (≥11/10 HPF); necrosis present
- Classified with high-grade neuroendocrine carcinomas alongside SCLC in WHO 2021
3.6 Typical and Atypical Carcinoids
Typical Carcinoid (TC):
- Well-circumscribed, vascularised, reddish-brown intrabronchial polypoid mass
- Histology: uniform round-to-spindle cells, organoid/trabecular pattern, abundant granular cytoplasm, "salt-and-pepper" chromatin; <2 mitoses/2mm²; no necrosis
- Low-grade; 5-year survival >90% with resection
Atypical Carcinoid (AC):
- 2-10 mitoses/2mm² OR punctate necrosis
- More aggressive than TC; intermediate prognosis
IHC: CD56, synaptophysin, chromogranin positive; low Ki-67 (<20% in TC; up to 20% in AC)
3.7 Sarcomatoid Carcinoma
Poorly differentiated NSCLC containing spindle cells, giant cells, or a sarcomatous component. Subtypes: pleomorphic carcinoma, spindle cell carcinoma, giant cell carcinoma, carcinosarcoma (carcinoma + sarcomatous differentiation), pulmonary blastoma. High grade; poor prognosis.
4. Diagnostic Approach
Step 1: Clinical Suspicion and Imaging
History and Examination:
- Smoking history (pack-years), haemoptysis, weight loss, chronic cough, Horner's syndrome, SVC syndrome
Chest X-Ray:
- First line; hilar mass, peripheral opacity, pleural effusion, mediastinal widening, cavitating lesion
CT Thorax (with contrast):
- Mandatory for all suspected cases
- Characterises mass, lymph node status, chest wall/vascular invasion, pleural involvement
- Guides biopsy approach
PET-CT (18F-FDG):
- SUV >2.5 is highly suspicious for malignancy
- Best for mediastinal lymph node and extrathoracic staging
- False negatives in lesions <8mm, carcinoids, diabetes
- False positives in TB and sarcoidosis
MRI Brain: For SCLC staging and suspected brain metastases; also for superior sulcus tumours (brachial plexus assessment)
Step 2: Tissue Diagnosis
The goal is histological + molecular characterisation of the tumour.
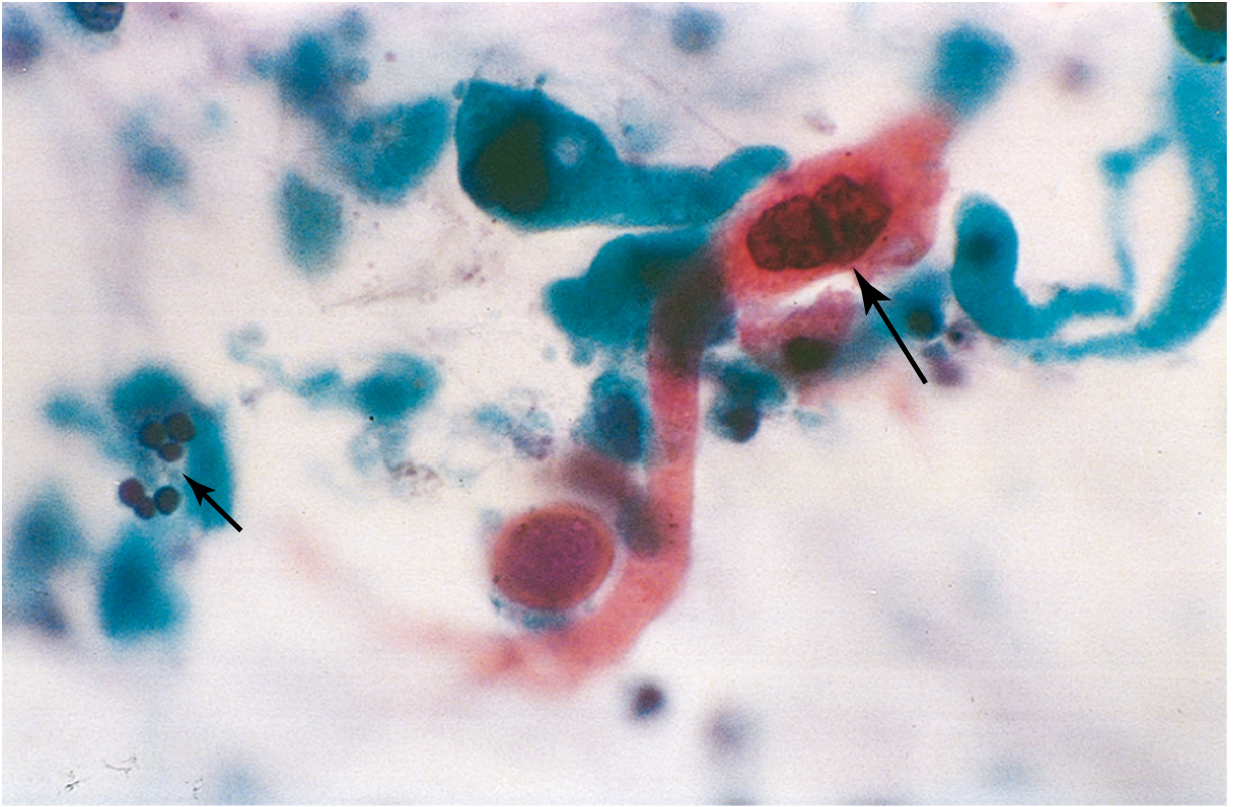
Sputum Cytology:
- Non-invasive; sensitivity ~40-60% for central tumours; lower for peripheral
- Positive findings: keratinised squamous cells with hyperchromatic nuclei (squamous carcinoma), adenocarcinoma cells with intracytoplasmic mucin vacuoles
Bronchoscopy:
- Flexible bronchoscopy with direct visualisation, brushings, washings, and transbronchial biopsy for central lesions
- Bronchoscopic biopsy: sensitivity ~70-80% for central endobronchial tumours
Endobronchial Ultrasound (EBUS):
- EBUS-guided transbronchial needle aspiration (TBNA) of mediastinal/hilar lymph nodes
- Key tool for mediastinal staging AND diagnosis concurrently
- Rapid on-site evaluation (ROSE) improves diagnostic yield
CT-guided Percutaneous Needle Biopsy:
- For peripheral lesions not accessible by bronchoscopy
- Core biopsy preferred over fine needle aspiration for molecular testing
- Pneumothorax is the main complication (~20-25%)
Video-Assisted Thoracoscopic Surgery (VATS) / Thoracoscopy:
- For pleural-based lesions, evaluation of pleural effusion
- Pleuroscopy + biopsy for malignant effusion
Surgical Resection:
- Provides definitive histological diagnosis AND curative treatment for resectable NSCLC
- Preferred margin assessment, lymph node staging
Step 3: Pathological Evaluation (Histology + IHC)
H&E morphology remains the cornerstone. IHC panel is applied when morphology alone is insufficient:
| IHC Marker | Adenocarcinoma | Squamous | SCLC | Carcinoid |
|---|---|---|---|---|
| TTF-1 | + | - | + | +/- |
| Napsin-A | + | - | - | - |
| p40/p63 | - | + | - | - |
| CK5/6 | - | + | - | - |
| CD56/Synaptophysin/Chromogranin | - | - | + | + |
| Ki-67 | Variable | Variable | >60% | <20% (TC) |
Step 4: Molecular/Biomarker Testing (Mandatory for NSCLC)
With modern targeted therapies, molecular profiling is essential for all advanced NSCLCs (especially adenocarcinoma):
| Biomarker | Frequency | Targeted Drug |
|---|---|---|
| EGFR mutation | ~15% (Western); up to 50% in Asian non-smokers | Osimertinib, erlotinib, gefitinib |
| ALK rearrangement | ~5% | Alectinib, crizotinib |
| ROS1 rearrangement | ~1-2% | Crizotinib, entrectinib |
| KRAS G12C | ~13% | Sotorasib, adagrasib |
| BRAF V600E | ~2-3% | Dabrafenib + trametinib |
| MET exon 14 skip | ~3-4% | Tepotinib, capmatinib |
| HER2 mutation | ~2-4% | Trastuzumab deruxtecan |
| PD-L1 expression | Variable | Pembrolizumab, atezolizumab |
Testing methods: Next-generation sequencing (NGS, liquid or tissue biopsy) is preferred over single-gene PCR. Liquid biopsy (circulating tumour DNA from plasma) is increasingly used when tissue is insufficient.
Step 5: Staging (TNM - IASLC 8th Edition)
- T: Tumour size and local invasion
- N: Regional lymph node involvement (N0-N3)
- M: Distant metastases
Practical staging workup:
- CT thorax/abdomen/pelvis
- PET-CT (preferred over CT alone for nodal and extrathoracic staging)
- MRI brain for SCLC (and NSCLC stage III/IV)
- EBUS ± mediastinoscopy for lymph node sampling when CT/PET show suspicious nodes
SCLC staging (simplified):
- Limited stage: confined to one hemithorax + ipsilateral nodes (within a radiotherapy portal)
- Extensive stage: beyond the above; ~two-thirds of patients at presentation
Summary Points
- Adenocarcinoma is now the most common lung cancer overall, including in women and non-smokers.
- The WHO 2021 classification groups neuroendocrine tumours as a spectrum (carcinoids → LCNEC → SCLC) and abolishes the term "bronchioloalveolar carcinoma."
- SCLC and NSCLC are the primary clinical divide because they differ in treatment strategy, prognosis, and biology.
- Paraneoplastic syndromes (SIADH, Cushing, hypercalcaemia, LEMS) may be the presenting feature.
- Pancoast syndrome and SVC syndrome are important patterns of regional spread.
- The diagnostic approach integrates imaging, tissue biopsy, IHC, and mandatory molecular testing for NSCLC.
- NGS-based molecular profiling now drives treatment selection in metastatic NSCLC.
Sources:
- Robbins, Cotran & Kumar Pathologic Basis of Disease (pp. 671-768)
- Robbins & Kumar Basic Pathology - Table 11.5, WHO classification 2021
- Harrison's Principles of Internal Medicine, 22e (pp. 659-670)
- Murray & Nadel's Textbook of Respiratory Medicine - Chapter 22 (WHO 2015 classification)
- Bailey & Love's Short Practice of Surgery, 28e (pp. 1006-1010)
- Mulholland & Greenfield's Surgery, 7e - Tables 79.1, 79.2
- Nicholson AG et al. The 2021 WHO Classification of Lung Tumors - J Thorac Oncol 2022 (PMID: 34808341)
This is a shared conversation. Sign in to Orris to start your own chat.