Pleural effusion
Reading File
Finding Sources
Searching PubMed
"pleural effusion"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
I now have comprehensive content to deliver a complete, well-illustrated answer on pleural effusion. Let me compile the full response.
Pleural Effusion
Pleural effusion is an abnormal collection of fluid in the pleural space - the potential space between the visceral and parietal pleura. Under normal conditions, approximately 1 L of fluid traverses the pleural space every 24 hours in a dynamic equilibrium, with only 0.1-0.2 mL/kg body weight present at any time. Effusions develop when fluid influx exceeds efflux.
Causes
Transudates
Caused by increased hydrostatic pressure or decreased oncotic pressure - no intrinsic pleural disease:
- Congestive heart failure (most common cause in the US)
- Cirrhosis with ascites
- Nephrotic syndrome
- Hypoalbuminemia / severe malnutrition
- Myxedema
- Peritoneal dialysis
- Glomerulonephritis
- Superior vena cava obstruction
- Pulmonary embolism (can be transudative or mixed)
Exudates
Caused by intrinsic pleural/pulmonary inflammation, altering permeability and lymphatic drainage:
Infections:
- Bacterial pneumonia - parapneumonic effusion (most common cause of exudate)
- Lung abscess / bronchiectasis
- Tuberculosis (leading cause in endemic areas)
- Viral illness
Neoplasms:
- Primary lung cancer
- Mesothelioma
- Pulmonary or pleural metastases
- Lymphoma
Connective Tissue Disease:
- Rheumatoid arthritis
- Systemic lupus erythematosus
Abdominal / GI Disorders:
- Pancreatitis
- Subphrenic abscess
- Esophageal rupture (rare but life-threatening)
- Abdominal surgery
Miscellaneous:
- Pulmonary infarction
- Uremia
- Drug reactions
- Chylothorax
- Postpartum state
Special note on PE: Pulmonary embolism produces a mixed picture - increased pulmonary vascular pressure creates a transudate component, while pleural ischemia and inflammation add an exudative component.
Pathophysiology
Pleural fluid is produced from systemic capillaries at the parietal pleural surface and absorbed into pulmonary capillaries at the visceral pleural surface, with lymphatics playing an essential supporting role. Net fluid accumulation is governed by differences in hydrostatic and oncotic pressures across the microvasculature.
- Transudates - ultrafiltrates of plasma with very little protein; result from imbalanced Starling forces (raised hydrostatic pressure or low oncotic pressure)
- Exudates - protein-rich; result from pleural inflammation, increased permeability, or impaired lymphatic drainage. As an exudative effusion is resorbed, residual fibrinous tissue can cause ongoing inflammation and adhesions.
Massive effusions (>1.5-2 L) - usually malignant; restrict respiratory movement, compress lung parenchyma, and cause intrapulmonary shunting. In extreme cases, tension hydrothorax can develop with mediastinal shift and circulatory compromise.
Hepatic hydrothorax - affects ~5-10% of cirrhotic patients; small diaphragmatic defects allow ascitic fluid into the pleural space. 85% are right-sided. Almost always transudative unless complicated by infection.
Clinical Features
- Small effusions - typically asymptomatic
- Dyspnea - generally does not develop until fluid reaches ≥500 mL
- Pleuritic chest pain - sharp, worse with deep breathing; suggests pleural inflammation
- Pain referred to ipsilateral shoulder - from diaphragmatic pleural irritation
Physical examination:
| Finding | Mechanism |
|---|---|
| Decreased/absent breath sounds | Fluid attenuating sound transmission |
| Dullness to percussion | Fluid replacing air |
| Decreased tactile fremitus | Fluid dampening vibration |
| Egophony at superior border | Underlying compressed (atelectatic) lung |
| Pleural friction rub | Early pleurisy before fluid accumulates |
Auscultatory percussion (percussing while listening with the stethoscope) may be more sensitive and specific than standard examination.
Diagnostic Imaging
Chest X-Ray
Erect PA view:
- Requires ~200 mL to be visible
- Classic sign: blunting of the costophrenic angle
- Larger effusions: hemidiaphragm obscured, concave upward meniscus (fluid layers higher laterally than medially)
- Massive effusion: complete opacification of hemithorax with contralateral mediastinal shift
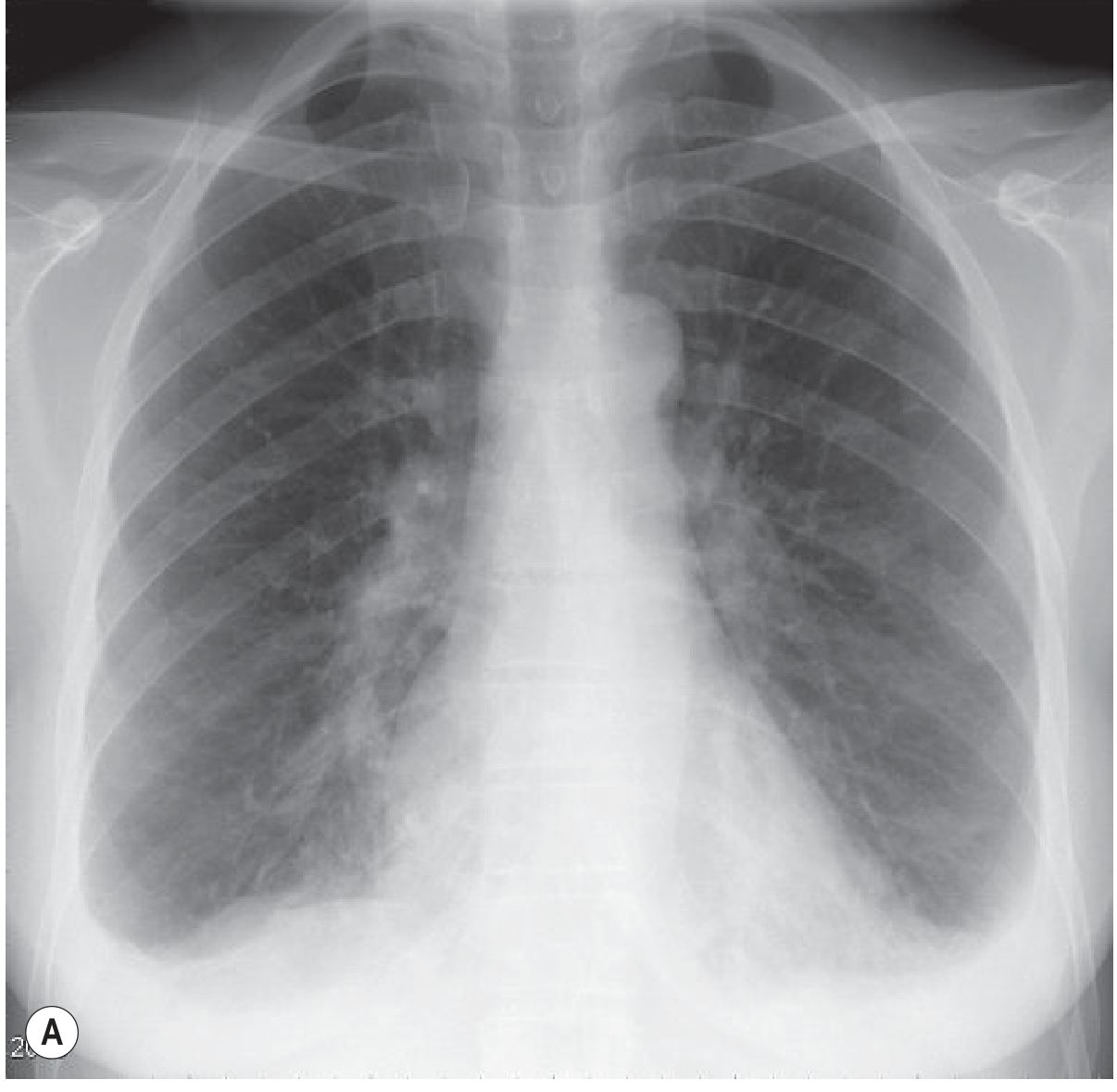
Bilateral pleural effusion on erect PA CXR. Note the concave upper margins, higher laterally than medially, blunting the costophrenic angles. - Grainger & Allison's Diagnostic Radiology
Supine view:
- Fluid gravitates posteriorly - effusion may not be visible
- Signs: diffuse haze over hemithorax, apical capping, obscured hemidiaphragm, widened minor fissure
- Costophrenic angles may NOT be blunted (a key pitfall)
Massive effusion with mediastinal shift:
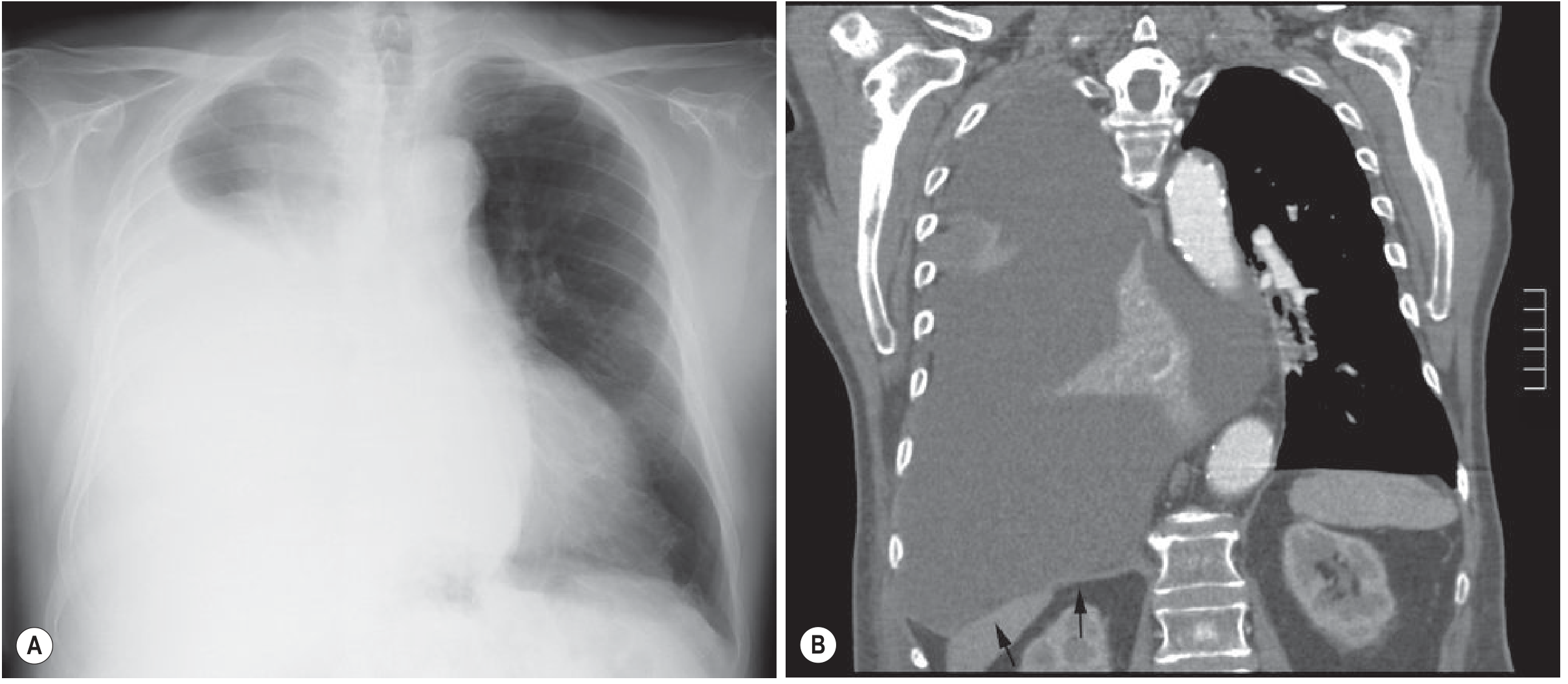
Massive pleural effusion displacing the mediastinum. CT shows compressed atelectatic lung within the effusion. Note depression of the right hemidiaphragm (arrows). - Grainger & Allison's Diagnostic Radiology
Subpulmonic effusion: appears as a "high hemidiaphragm" with peak more lateral than usual and rapid lateral fall to the costophrenic angle; left-sided: stomach bubble separation >2 cm.
Loculated effusions: fluid confined between pleural adhesions, often against the chest wall; transudates can loculate in interlobar fissures as "pseudotumors" or "vanishing tumors."
Ultrasound
- Detects as little as 50 mL of fluid
- More sensitive than CXR for diagnosis and size estimation
- Transudates: typically anechoic (echo-free)
- Exudates/hemorrhagic: echogenic, often with pleural thickening, septations, or fibrinous stranding
- Gold standard for guiding thoracentesis - significantly reduces risk of iatrogenic pneumothorax
CT
- Gold standard for detecting small effusions - detects as little as 3-5 mL
- Distinguishes pleural from parenchymal disease
- Identifies underlying cause (malignancy, PE, pneumonia)
- Helps quantify fluid and plan thoracentesis
Diagnostic Thoracentesis
Most pleural effusions should undergo diagnostic thoracentesis to classify the fluid and identify the underlying cause. Exceptions exist when the cause is obvious (e.g., bilateral effusions in decompensated heart failure responding to diuretics).
Light's Criteria (most widely accepted)
Fluid is classified as an exudate if any one of the following is met:
| Criterion | Threshold |
|---|---|
| Pleural fluid protein / serum protein | > 0.5 |
| Pleural fluid LDH / serum LDH | > 0.6 |
| Pleural fluid LDH | > 2/3 upper limit of normal serum LDH |
If none of the three criteria are met, the effusion is a transudate.
Additional Pleural Fluid Analysis
| Test | Significance |
|---|---|
| pH <7.3 | Parapneumonic effusion, malignancy, rheumatoid, TB, systemic acidosis |
| pH <7.0 | Strongly suggests empyema or esophageal rupture → indication for tube thoracostomy |
| Gram stain + culture | Rule out empyema / parapneumonic effusion |
| Cytology | Assess for malignant cells (sensitivity does not depend on volume collected) |
| Bloody fluid (hematocrit >50% of blood) | Hemothorax by definition |
| Atraumatic bloody fluid | Suggests trauma, neoplasm, or pulmonary infarction |
Management
General Approach
- Most effusions do not require emergent drainage
- Treat the underlying cause first (e.g., diuretics for CHF, antibiotics for parapneumonic)
Therapeutic Thoracentesis - Indications
- Massive effusion (>1.5-2 L) causing hemodynamic or respiratory compromise
- Empyema (urgent)
- Symptomatic relief (e.g., recurrent malignant effusion)
Volume limit: Remove no more than 1500 mL in a single procedure (BTS Grade C recommendation) to reduce risk of reexpansion pulmonary edema.
Relative contraindications: coagulopathy, history of pleurodesis, chest wall infection, pleural adhesions (latter risk reduced with ultrasound guidance)
Complications: iatrogenic pneumothorax (most common), hemothorax, lung laceration, infection, transient hypoxia, hypotension (large volume drainage in volume-depleted patients), reexpansion pulmonary edema
Empyema / Parapneumonic Effusion
- Empyema develops in 5-10% of parapneumonic effusions
- Requires chest tube drainage for source control
- Small-bore pigtail catheters (14 Fr) are now accepted as first-line over large-bore (28-40 Fr)
- Early surgical drainage (VATS) results in better outcomes than conservative management
Malignant Pleural Effusion
- Marker of significant morbidity and mortality
- Therapeutic thoracentesis provides short-term relief but malignant effusions recur rapidly
- Chemical pleurodesis (talc, doxycycline) creates permanent obliteration of the pleural space
- Indwelling pleural catheter - allows outpatient drainage; useful for palliation or bridging to definitive therapy
Hepatic Hydrothorax
- Sodium restriction + diuretics - first-line
- TIPS (transjugular intrahepatic portosystemic shunting) - initial response 70-80%; limited by shunt occlusion, worsening liver function, hepatic encephalopathy
- Indwelling pleural catheters - bridge to transplantation or palliation
- VATS pleurodesis / diaphragmatic defect repair - for refractory cases not eligible for TIPS
- Conventional chest tube drainage is NOT recommended (risk of protein/electrolyte loss, infection, renal failure)
Gas Exchange Effects
Pleural effusions cause generally mild hypoxemia. The primary mechanism is a mildly elevated intrapulmonary shunt (~7%). Importantly, large right-sided effusions can have hemodynamic effects similar to cardiac tamponade (impaired right ventricular filling), contributing to hypoxemia via low cardiac output and low mixed venous PO2. The effect of thoracentesis on arterial PO2 is inconsistent - it may increase, remain unchanged, or even decrease.
Disposition
| Effusion Type | Course |
|---|---|
| Post-surgical / postpartum (small) | Almost always resolve spontaneously within days |
| Viral pleuritis | Self-limited; symptomatic support only |
| CHF-related | Often respond to diuresis; may need admission for IV diuretics |
| Parapneumonic | Reason to hospitalize patients with CAP |
| Malignant | Significant morbidity; close outpatient follow-up after drainage |
| Unexplained | ~20% of all effusions; most resolve spontaneously without sequelae, but unexplained effusion must raise concern for malignancy |
Sources:
- Rosen's Emergency Medicine: Concepts and Clinical Practice - Pleural Effusion chapter, p. 988-991
- Murray & Nadel's Textbook of Respiratory Medicine - Hepatic Hydrothorax and Gas Exchange sections
- Grainger & Allison's Diagnostic Radiology - Pleural Effusion imaging
Recent evidence (2024-2026):
- A 2025 systematic review (PMID: 39708436) specifically addresses management of pleural effusion in mechanically ventilated critically ill patients - relevant for ICU settings.
- A 2025 meta-analysis (PMID: 40294877) found intrapleural fibrinolytic therapy has benefit for loculated malignant pleural effusions.
- A 2024 meta-analysis (PMID: 39182102) compared surgery vs. intrapleural fibrinolysis for complicated pleural infections - no significant survival difference found, but fibrinolysis may be preferred first-line in appropriate patients.
This is a shared conversation. Sign in to Orris to start your own chat.