Treatment of 3X3cm abscess in thigh
Reading File
Finding Sources
Searching PubMed
skin abscess incision drainage antibiotic treatment
Reading File
Finding Sources
Reading File
Reading File
Reading File
I now have comprehensive information. Here is a structured treatment guide for a 3×3 cm thigh abscess:
Treatment of a 3×3 cm Thigh Abscess
Overview
A 3×3 cm abscess is a moderate-sized, fluctuant collection. At this size, conservative measures (warm compresses, antibiotics alone) are insufficient — incision and drainage (I&D) is the treatment of choice. Antibiotics are usually unnecessary after adequate I&D unless there is surrounding cellulitis or the patient is immunocompromised.
— Pfenninger and Fowler's Procedures for Primary Care, 3rd ed.
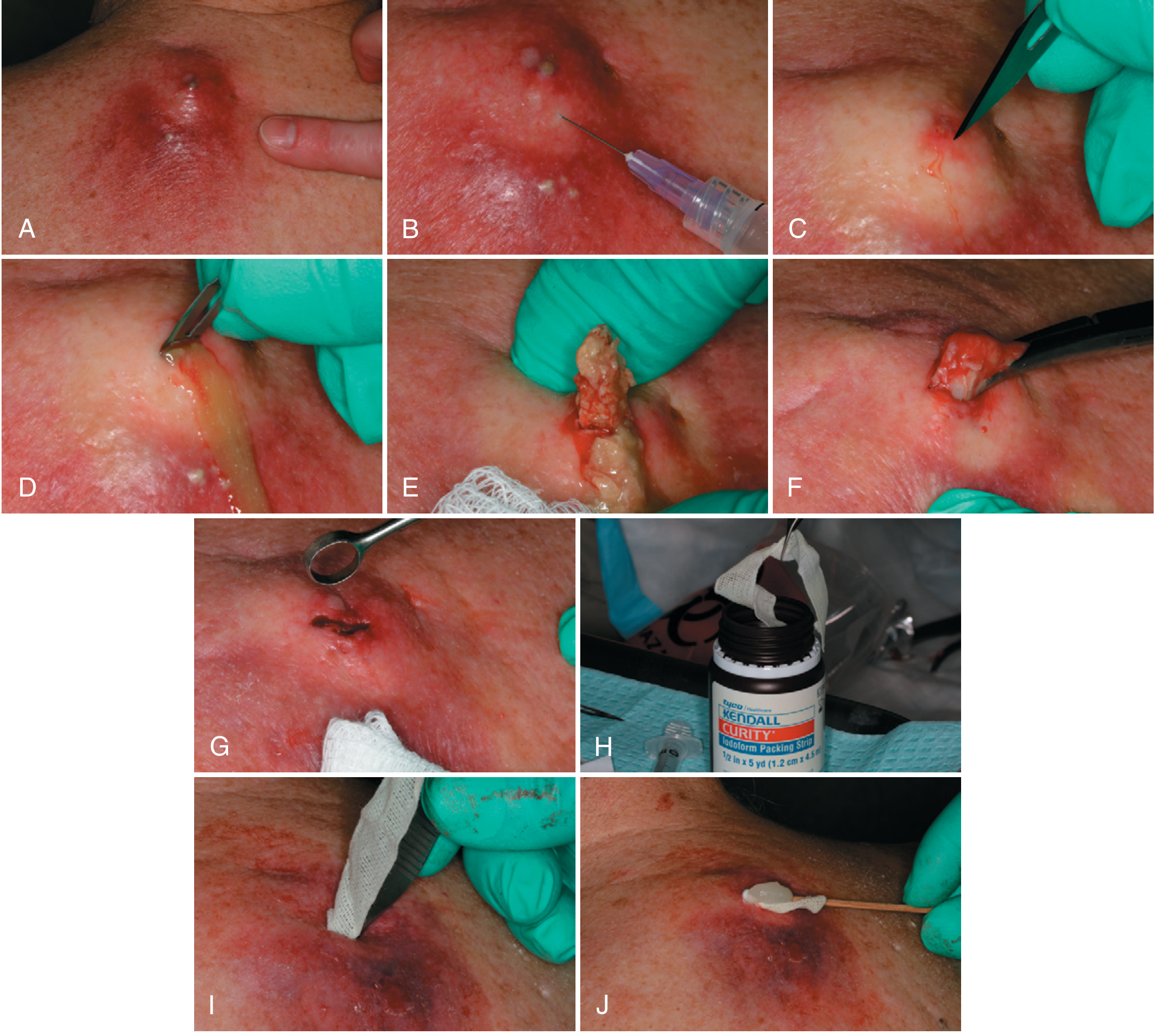
Step-by-Step I&D Procedure
Equipment needed:
- 1–2% lidocaine with sodium bicarbonate (to reduce sting), 25–30g needle
- Povidone-iodine or alcohol prep
- No. 11 scalpel blade
- Curved hemostats
- Iodoform gauze (¼–½ inch wide, up to 24 inches for this cavity size)
- 4×4 gauze, dressing, culture swab
Technique:
- Prepare the skin with povidone-iodine or alcohol.
- Field block anesthesia — infiltrate the perimeter of the abscess, not into the cavity. Local anesthetics work poorly in the acidic environment inside the abscess; more volume than usual may be needed.
- Incise with a no. 11 blade — make the incision wide enough (typically ~1 cm) to prevent premature closure. Follow skin lines where possible. Premature closure is the most common cause of recurrence.
- Culture — aspirate or swab from inside the cavity (not the surface skin) before expressing pus, especially if the patient is immunocompromised or the infection is recurrent.
- Express all pus with external digital pressure. Explore the cavity with hemostats and break down any internal septa or walled-off pockets.
- Pack the cavity with iodoform gauze — leave a small "tail" protruding for drainage. Apply antibiotic ointment over the gauze tail to prevent the outer dressing from sticking.
- Packing management:
- For a cavity this size, leave the wick in place for ~4 weeks, advancing it every few days (cut off ~2 inches at a time) to allow healing from the inside out.
- First packing change at 5–7 days to reduce purulence and check wound progress.
- Sterile dressing over the area; change several times daily.
Antibiotics
| Situation | Recommendation |
|---|---|
| Uncomplicated abscess, no cellulitis | Not needed after adequate I&D |
| Surrounding cellulitis | Add antibiotic covering S. aureus |
| Immunocompromised / diabetic | Consider antibiotics + send culture |
| Recurrence after I&D | Send culture/sensitivity; consider MRSA coverage |
MRSA coverage options (community-associated): trimethoprim-sulfamethoxazole, clindamycin, doxycycline, or rifampin — guided by local resistance patterns and culture results.
Pathogen Context
- Most common: Staphylococcus aureus (including community-MRSA, now the leading pathogen in ED presentations)
- Less common: Streptococcus spp., gram-negative organisms, anaerobes (particularly in perineal/groin abscesses)
Warning Signs Requiring Reassessment
Instruct the patient to return immediately for:
- Re-accumulation of pus
- Fever and chills
- Increasing pain, redness, or swelling
- Red streaks (lymphangitis) near the abscess
When to Escalate
- Failure to improve after I&D → suspect deep tissue extension; may need IV antibiotics, hospitalization, or surgical debridement
- Recurrence → culture for MRSA; adjust antibiotics accordingly
- Possible complications: cellulitis progression, septicemia, fistula formation, osteomyelitis (rare at thigh site)
— Pfenninger and Fowler's Procedures for Primary Care, 3rd ed., pp. 176–178
Its kind of painfull red hot firm swelling
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
This changes the picture. Here's the updated assessment:
Revised Assessment: Firm, Non-Fluctuant Swelling
What This Means Clinically
A firm (non-fluctuant) swelling — even with redness, heat, and pain — indicates that pus has not yet localized into a drainable collection. This is cellulitis / early pre-suppurative stage, not a mature abscess ready for I&D.
"An area of induration alone with no fluctuance indicates isolated cellulitis and is treated with antibiotics and warm compresses." — Textbook of Family Medicine, 9th ed.
Do NOT incise a firm, non-fluctuant swelling — there is no pus pocket to drain, and premature I&D yields nothing and risks unnecessary trauma/scarring.
Immediate Management
| Measure | Detail |
|---|---|
| Warm compresses | 15–20 min, 3–4× daily — promotes localization and may facilitate spontaneous pointing |
| Antibiotics | Required at this stage |
| Elevation of the limb | Reduces edema and inflammation |
| Analgesia | NSAIDs (also reduce inflammation) or paracetamol |
Antibiotic Choice
Target organism is S. aureus (MRSA must be considered):
Oral (mild–moderate):
- Clindamycin — good MRSA coverage
- TMP-SMX (co-trimoxazole) — effective for community MRSA
- Cephalexin / Dicloxacillin — if MRSA unlikely
IV (moderate–severe or systemic signs):
- Cefazolin or Ceftriaxone
- Vancomycin — if MRSA suspected or severe
Duration: Typically 5–7 days for uncomplicated cellulitis; reassess at 48–72 hours.
Monitoring — Reassess in 48–72 Hours
Watch for these changes:
| Sign | Meaning | Action |
|---|---|---|
| Swelling becomes soft/fluctuant | Pus has localized → now a mature abscess | Proceed with I&D |
| Spreading redness, fever, rigors | Progressing cellulitis / sepsis | Escalate to IV antibiotics / hospital |
| Red streaks proximally | Lymphangitis | Urgent IV antibiotics |
| No improvement at 48–72h | Consider deeper infection, MRSA, or necrotizing fasciitis | Imaging (USS/MRI) + surgical review |
Ultrasound — Useful Here
Bedside ultrasound is very helpful in this scenario:
- Abscess → hypoechoic fluid-filled cavity (confirms pus present, guides I&D)
- Cellulitis → "cobblestoning" pattern (no drainable collection)
This is especially useful when examination is equivocal — a firm swelling may still contain a small central pocket not palpable on exam.
Summary
| Stage | Exam Findings | Treatment |
|---|---|---|
| Pre-suppurative (now) | Firm, indurated, hot, red | Antibiotics + warm compresses |
| Mature abscess | Fluctuant, "pointing" | I&D + packing |
Monitor closely — if it softens and becomes fluctuant over the next 2–5 days, it is ready for I&D as described previously.
— Textbook of Family Medicine 9e; Rosen's Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.