Stoma Examination and viva for practical examination PG general surgery
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive material from multiple authoritative surgical textbooks. Let me compile the complete PG surgery examination guide on stoma.
Stoma - Examination & Viva Guide for PG General Surgery
Definition
A stoma (Greek: "mouth") is a surgically created opening in the abdominal wall that brings a portion of the bowel (or urinary tract) to the surface to divert the contents of the gut (feces/urine) - Bailey & Love's Short Practice of Surgery, 28th Ed.
A stoma may serve as:
- A definitive procedure (permanent stoma)
- A temporary diversion to protect a distal anastomosis or allow healing
- A salvage from a failed/complicated prior surgical intervention
Classification
By Duration
| Type | Characteristics |
|---|---|
| Temporary | Protects anastomosis, diverts fecal stream; intended for reversal |
| Permanent | Required when continuity cannot be restored (e.g., APR, total colectomy with incontinence) |
By Bowel Used
| Stoma | Bowel segment | Output character |
|---|---|---|
| Ileostomy | Ileum | Liquid/semi-liquid, caustic, high volume |
| Colostomy | Colon | Varies - ascending = liquid; descending/sigmoid = formed, less irritant |
| Urostomy/Ileal conduit | Ileum (urinary diversion) | Urine |
By Configuration
| Type | Description | Common use |
|---|---|---|
| End stoma | Single barrel; bowel divided, proximal end brought out | APR (end colostomy), Hartmann's procedure |
| Loop stoma | Loop of bowel with supporting rod; two openings (afferent/efferent) | Temporary diversion; easier to close |
| Double-barrel | Both limbs brought out as separate stomas | Emergency; significant inflammation/sepsis |
| End-loop | Loop mobilized, distal limb stapled/oversewn | Alternative to loop; useful with limited mesentery |
| Ghost ileostomy | Loop marked but not opened, sutured subfascially | "Safety net" if anastomotic leak occurs post-op |
Viva point: A transverse loop colostomy should be avoided - it is large, prone to prolapse, placed in the belt line (mid-upper abdomen), making pouching difficult. - Sabiston Textbook of Surgery
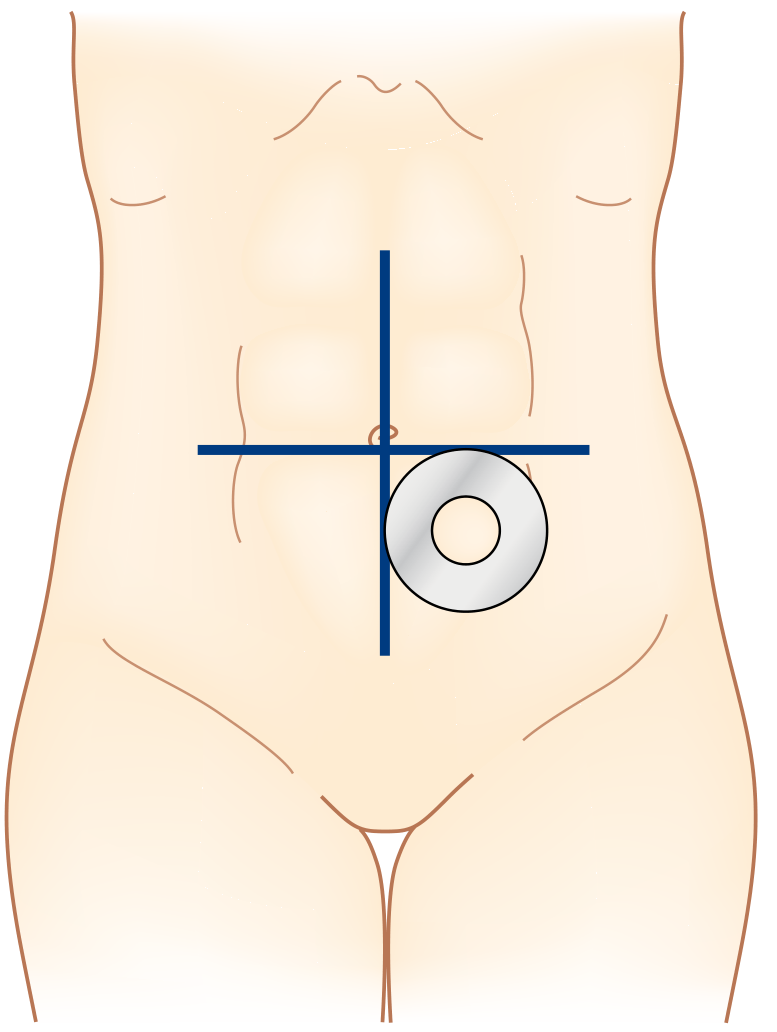
Sites and Siting
Ideal Stoma Site Criteria (must know for viva)
- Within the rectus abdominis muscle (reduces hernia and prolapse risk)
- At the infraumbilical fat mound - ideally where patient can see it
- Away from bony prominences (ASIS, costal margin), umbilicus, scars, skin folds, belt line
- Assessed in three positions - lying, sitting, standing - to avoid creases that appear only in certain postures
- Right iliac fossa (RIF) - ileostomy site
- Left iliac fossa (LIF) - sigmoid colostomy site
- Should be marked preoperatively by the stoma nurse (enterostomal therapist)
Stoma Aperture Construction
- Disk of skin 1.5-2 cm diameter excised at marked site
- Subcutaneous fat incised to anterior rectus fascia
- Rectus muscle split (not cut) with a curved clamp
- Posterior fascia opened sharply into peritoneum
- Final aperture = two fingerbreadths (adequate for bowel + mesentery to pass without tension)
- Larger aperture needed in obese patients or obstructed mesentery
Viva Q: Why is the stoma brought through the rectus muscle? - To reduce risk of parastomal hernia and prolapse by the muscular support it provides. - Fischer's Mastery of Surgery, 8th Ed.
Types in Detail
Ileostomy
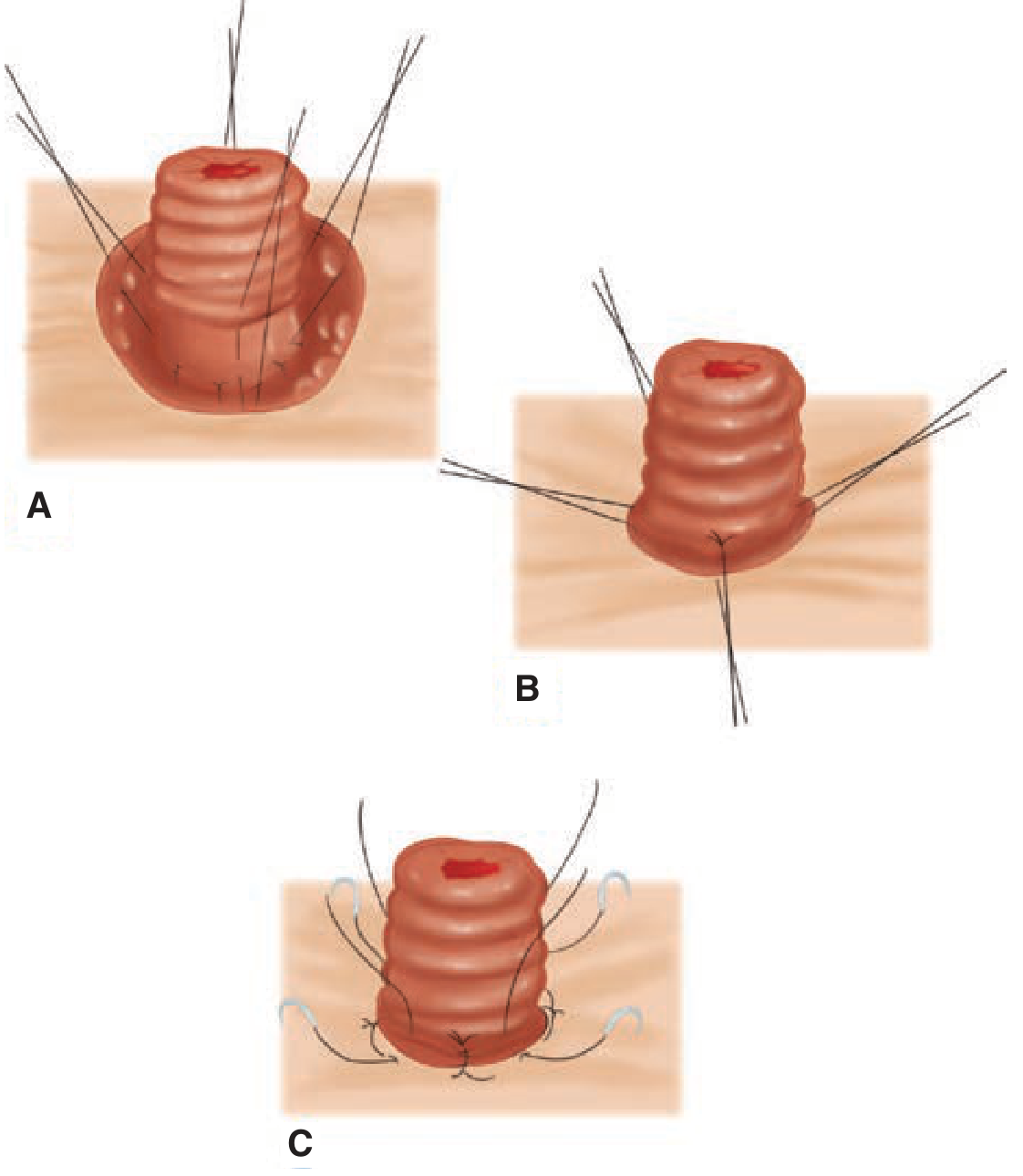
Brooke Ileostomy (standard end ileostomy technique):
- Stump brought 4-5 cm above skin level
- Four sutures placed at 90° to each other incorporating: cut end of ileum + seromuscular layer at level of anterior rectus fascia + subcuticular skin edge
- Sutures tied to produce stomal eversion (the "spout" or "rose bud" appearance)
- Additional simple sutures complete the maturation
- Purpose of spout (2-3 cm protrusion): caustic ileostomy effluent is delivered directly into the pouch, away from skin, reducing excoriation
Loop Ileostomy:
- Segment of distal ileum brought through abdominal wall defect as a loop
- Rod/bridge may be placed to prevent retraction
- Enterotomy created, stoma matured
- Can also be divided loop - linear cutting stapler across distal limb flush with skin, then proximal limb matured - prevents incomplete diversion
Indications for ileostomy:
- Protection of low rectal or ileal anastomosis
- Total colectomy for UC (before IPAA or as permanent in cases of incontinence)
- Crohn's disease (temporary/permanent)
- Familial adenomatous polyposis (FAP) - after colectomy
- Ileostomy output guide for colectomy decision (high output = avoid)
Output: 500-1500 mL/day (liquid); contains active digestive enzymes → high risk of peristomal skin excoriation
Colostomy
End Colostomy (Hartmann-type / permanent after APR):
- Protrudes only 0.5-1 cm above skin level (effluent is formed, not caustic)
- No spout needed
- Matured with interrupted absorbable sutures
Loop Colostomy (transverse or sigmoid):
- Descending/sigmoid preferred over transverse
- Transverse loop colostomy: avoid - high prolapse rate, poor bag adhesion (belt line)
Double-barrel Colostomy (Paul-Mikulicz):
- Both proximal and distal limbs brought out
- Used in emergency situations with significant contamination or fistula
Ascending colostomy → high liquid output (like ileostomy)
Descending/sigmoid colostomy → formed stool, less skin irritation
Indications for colostomy:
- Obstructing or perforated left colon cancer (Hartmann's procedure)
- Anorectal trauma (fecal diversion)
- Recto-vaginal or recto-urethral fistulas
- Hirschsprung's disease (leveling colostomy)
- Radiation proctitis
- Perineal sepsis / Fournier's gangrene
Difference Between Ileostomy and Colostomy
| Feature | Ileostomy | Colostomy |
|---|---|---|
| Site | RIF | LIF (sigmoid) |
| Protrusion | 2-3 cm spout (Brooke) | 0.5-1 cm flush |
| Output | Liquid, 500-1500 mL/day | Semi-formed to formed |
| Output enzymes | Active - caustic | Inactive |
| Skin excoriation risk | High | Low (sigmoid) |
| Bag change | Daily or more | Every 2-3 days |
| Mesentery | Mobile, no vascular ligation needed | May need central ligation in obese |
| Odor | Less | More |
| Closure | Without formal laparotomy usually | Similar |
Preoperative Preparation (Stoma Care)
- Preoperative marking by stoma nurse/enterostomal therapist is mandatory
- Assess abdomen in sitting, standing, bending positions
- Consider clothing habits (belt position, clothing type)
- Psychological preparation and counseling (permanent stoma has major psychosocial impact)
- Optimize nutrition (malnourished patients have higher complication rates)
- Bowel preparation: role is limited in emergency settings
Complications of Stoma
Up to 30% of patients require operative revision for stoma complications. - Fischer's Mastery of Surgery
Early Complications (within 30 days)
| Complication | Cause | Management |
|---|---|---|
| Necrosis / Ischemia | Tension on mesentery; inadequate blood supply; tight aperture; hypotension | Use transparent pouch for inspection; clear tube + flashlight to assess level; necrosis below fascia = re-exploration + new stoma; above fascia = expectant ± revision |
| Retraction | Tension, obesity, mesenteric edema | Convex skin barrier; stoma belt; local revision or relocation if persistent |
| Mucocutaneous separation | Tension, infection, poor technique, ischemia | Minor: allow to heal by secondary intention; Major: revision |
| High output (ileostomy) | Short bowel; Crohn's activity | Dietary modification; loperamide; codeine; IV fluids; octreotide in refractory cases |
| Peristomal skin excoriation | Effluent contact (especially ileostomy) | Correct appliance; barrier creams; convex skin barrier |
Late Complications (after 30 days)
| Complication | Features | Management |
|---|---|---|
| Parastomal hernia | Most common late complication; bowel through fascial defect beside stoma | Conservative (support belt); surgical - Sugarbaker repair or keyhole repair with mesh; laparoscopic/robotic preferred |
| Prolapse | Bowel telescopes outward; more common in loop stomas (efferent limb) and transverse colostomy | Manual reduction; surgical revision if recurrent/incarcerated |
| Stenosis | At skin or fascial level; from ischemia, Crohn's, scar, inadequate aperture | Gentle dilatation (short-term); surgical revision; assess for Crohn's/malignancy in late onset |
| Skin irritation / Dermatitis | Contact dermatitis, candidiasis, psoriasis | Correct appliance fitting; antifungals if candida; barrier creams |
| Bleeding | From mucosa (trauma), varices (portal hypertension - "caput medusae" around stoma) | Minor: conservative; variceal: local measures, TIPS |
| Fistulation | Crohn's disease; deep suture | Examination; Crohn's work-up; surgical revision |
Stoma Necrosis - Assessment Method
- Use clear tube (test tube) + flashlight inserted into stoma
- If mucosa viable = pink/red above fascia level → conservative
- If black/cyanotic extending below fascia → re-exploration required
Stoma Reversal (Closure)
Prerequisites for closure:
- Anastomosis healed - confirm with contrast enema (Gastrografin) and flexible endoscopy
- Patient nutritionally optimized
- No active sepsis or disease
- Cancer patients: defer until completion of adjuvant chemotherapy
- Generally performed 8-12 weeks after index surgery
Technical considerations:
- Elliptical incision around stoma
- Bowel dissected free of subcutaneous tissue and fascia
- Hand-sewn or stapled anastomosis; return bowel to peritoneal cavity
- Stoma site closure: purse-string leaving small opening, or skin closure over Penrose drain
- Mesh reinforcement of fascial defect at time of closure reduces risk of incisional/parastomal hernia
Complications of reversal:
- Anastomotic leak
- Wound infection (contaminated field)
- Incisional hernia at stoma site
Parastomal Hernia - Management (High-yield Viva)
Repair techniques:
- Sugarbaker repair - mesh placed without fenestration; intestine lateralized between mesh and abdominal wall; lower recurrence rate but requires bowel redundancy
- Keyhole repair - mesh fenestrated to allow stoma passage; more natural bowel course but higher recurrence (fenestration enlarges over time)
- Stoma relocation - move stoma to opposite side + mesh repair of original defect
Open vs. Laparoscopic/Robotic:
- Laparoscopic/robotic preferred: fewer wound complications (incisions remote from contaminated stoma site)
- Open: more wound morbidity but technically less demanding
High-Output Ileostomy
Definition: Output > 2000 mL/day
Causes: Short bowel syndrome, Crohn's, post-op ileus resolution, bacterial overgrowth, medications
Complications: Dehydration, hyponatremia, hypomagnesemia, metabolic acidosis, renal failure
Management:
- Restrict hypotonic fluids
- Oral rehydration solution (high sodium - >90 mEq/L)
- Loperamide (slows transit)
- Codeine phosphate
- Proton pump inhibitor (reduces GI secretions)
- Octreotide (severe/refractory)
- Nutritional support - parenteral if needed
Stoma Appliances
One-piece system: Skin barrier and pouch integrated - simpler, less bulky, for established stomas
Two-piece system: Separate skin wafer + pouch that clicks on - allows pouch change without disturbing skin
Closed-end pouch: For colostomy (formed stool) - disposed after single use
Open-end/drainable pouch: For ileostomy (liquid output) - drained periodically, changed every 1-3 days
Convex wafer: Used in retracted stoma to push skin in and direct effluent into pouch
Irrigation of Colostomy
- Used for sigmoid/descending colostomy only (formed stool, adequate length of colon)
- 500-1000 mL warm water instilled via cone irrigation set into stoma
- Promotes bowel evacuation at a predictable time; patient can go "bag-free" between irrigations
- Not suitable for ileostomy (liquid, unpredictable output) or transverse/ascending colostomy
Stoma and Quality of Life
- Permanent stoma has significant psychological, sexual, and social impact
- Stoma care nurse (enterostomal therapist) role: preoperative education, site marking, postoperative appliance training, complication management, emotional support
- Support groups, counseling, and regular follow-up mandatory
- Body image disturbance is a recognized complication - address proactively
Key Viva Questions & Model Answers
Q: What are the components of an ideal stoma?
A: Correct site (within rectus, visible, away from bony prominences and folds), adequate blood supply without tension, appropriate protrusion (ileostomy 2-3 cm spout; colostomy flush), proper aperture size (2 fingerbreadths), secure mucocutaneous union.
Q: Why does an ileostomy have a spout but a colostomy does not?
A: Ileal effluent is liquid and contains active proteolytic enzymes - highly caustic to skin. The spout delivers effluent directly into the pouch bag, protecting peristomal skin. Colonic effluent (especially sigmoid) is formed and less irritating, so flush maturation is adequate.
Q: What is the most common late complication of stoma?
A: Parastomal hernia. Incidence up to 30-50% at 5 years for end colostomy.
Q: How do you assess viability of a necrotic-appearing stoma?
A: Insert a transparent/clear test tube into the stoma lumen and inspect with a flashlight. Assess the level of ischemia relative to the fascia. Above fascia = conservative; below fascia = re-operation required.
Q: What is a Hartmann's procedure?
A: Resection of the rectosigmoid with end colostomy (LIF) and closure of the rectal stump as a blind pouch. Done in emergency setting (perforated sigmoid cancer, diverticular perforation with peritonitis) when primary anastomosis is unsafe.
Q: What is the 'ghost ileostomy'?
A: A loop of ileum is prepared and marked but not exteriorized - it is sutured beneath the anterior abdominal wall. Acts as a safety net. If anastomotic leak occurs postoperatively, the ghost ileostomy can be quickly converted to a functioning stoma without full re-laparotomy.
Q: What is Turnbull-Blowhole colostomy?
A: Decompressive loop colostomy (without formal laparotomy) used in toxic megacolon - particularly in pregnancy or in patients too unstable for major surgery. Skin is incised over the dilated loop, which is then opened and fashioned as a stoma.
Q: What is the difference between Sugarbaker and keyhole repair for parastomal hernia?
A: Sugarbaker repair - mesh without fenestration, intestine lateralized between mesh and abdominal wall; lower recurrence. Keyhole repair - mesh with central fenestration for stoma; higher recurrence because the fenestration tends to enlarge over time. Both carry risks of obstruction, mesh erosion, and bowel ischemia.
Summary Table: Ileostomy vs Colostomy
| End Ileostomy | Loop Ileostomy | End Colostomy | Loop Colostomy | |
|---|---|---|---|---|
| Common site | RIF | RIF | LIF | Transverse/sigmoid |
| Protrusion | 2-3 cm (spout) | 2-3 cm | 0.5-1 cm | Flush/minimal |
| Output | Liquid | Liquid | Formed | Semi-formed |
| Permanent/Temp | Both | Usually temp | Both | Usually temp |
| Reversal | Formal laparotomy usually | Often without laparotomy | Hartmann reversal | Without formal laparotomy |
| Prolapse risk | Low | Moderate (efferent limb) | Low | High (transverse) |
Sources: Bailey & Love's Short Practice of Surgery (28th Ed.) | Sabiston Textbook of Surgery | Schwartz's Principles of Surgery (11th Ed.) | Fischer's Mastery of Surgery (8th Ed.) | Maingot's Abdominal Operations
Indications
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Your credits are exhausted. You can purchase a top-up or subscribe to a plan to continue using Orris. If you're already subscribed, your daily credits will reset tomorrow.
Management of parastomal hernia PG level
Your credits are exhausted. You can purchase a top-up or subscribe to a plan to continue using Orris. If you're already subscribed, your daily credits will reset tomorrow.
This is a shared conversation. Sign in to Orris to start your own chat.