Is there any way where I recover 100% curable discs from disc dessication grade III-4
Reading File
Finding Sources
Searching PubMed
intervertebral disc desiccation regeneration treatment
Searching the Web
disc desiccation grade 3 4 recovery treatment regeneration 2024 2025
Finding Sources
Searching PubMed
intervertebral disc degeneration regeneration stem cell platelet
Finding Sources
Reading Article
Reading Article
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Here is a complete, honest answer to your question.
Disc Desiccation Grade III-IV: Can It Be 100% Reversed?
The short answer: No. There is currently no treatment that achieves 100% structural restoration (cure) of a Grade III-IV desiccated disc. This is not pessimism - it is the consistent conclusion of every major textbook and recent systematic review. However, there is a spectrum of options from symptom management to promising biological therapies, and the field is actively evolving.
What Grade III-IV Means
Disc desiccation is graded on the Pfirrmann scale (I-V):
| Grade | Appearance on MRI T2 | Structure | Disc Height |
|---|---|---|---|
| I | Bright white (normal hydration) | Homogeneous | Normal |
| II | White with horizontal band | Inhomogeneous | Normal |
| III | Grey (moderate signal loss) | Inhomogeneous, no clear nucleus/annulus distinction | Normal or slightly reduced |
| IV | Dark grey to black | Inhomogeneous, lost distinction | Normal to moderately reduced |
| V | Black | Collapsed, no disc space | Severely collapsed |
The MRI below shows the "black disc" appearance of desiccated lumbar discs on T2 - the loss of bright signal reflects loss of water content in the nucleus pulposus:
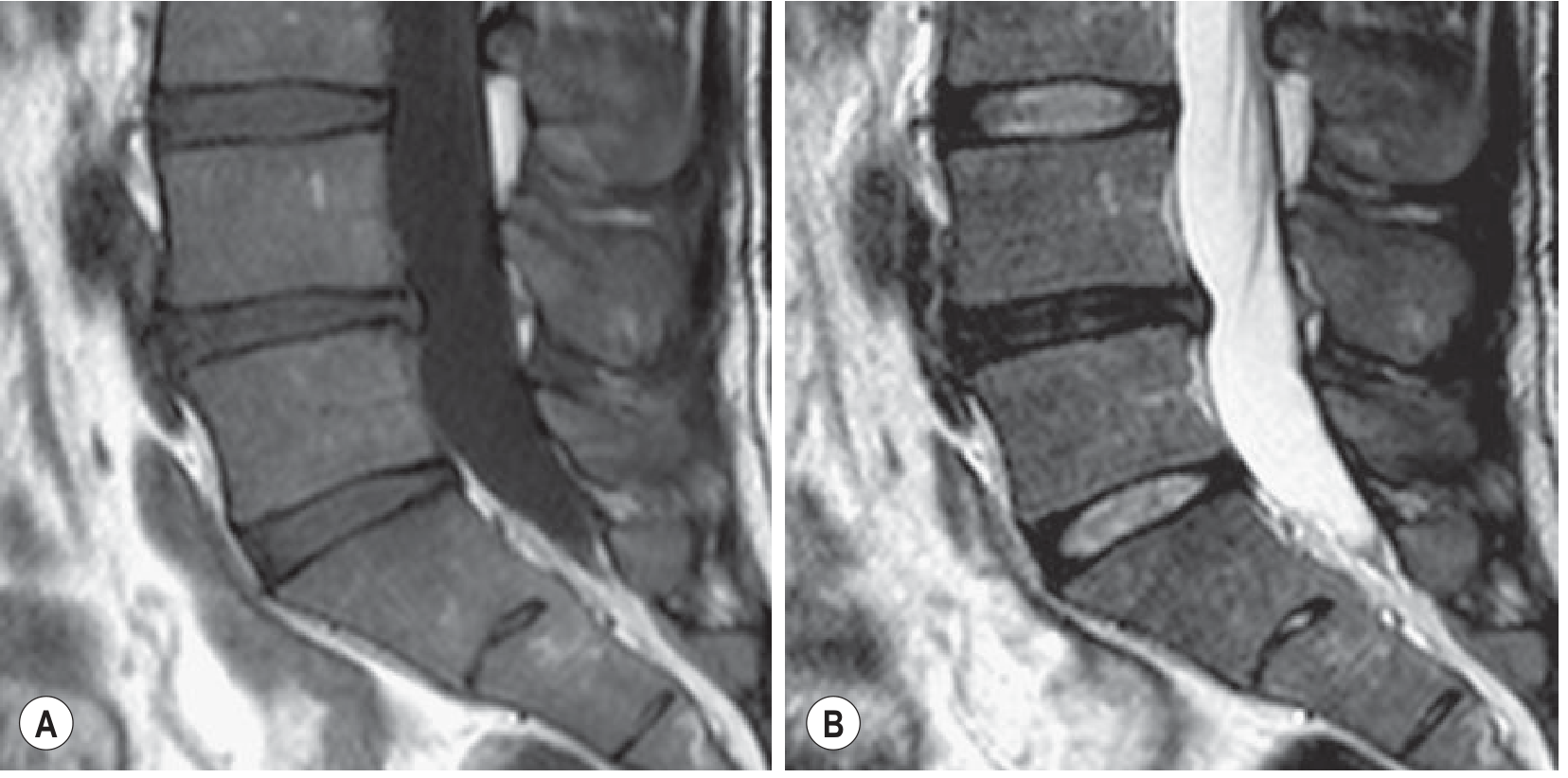
From Grainger & Allison's Diagnostic Radiology: Sagittal T1 (A) and T2 (B) in a 34-year-old man. Decreased T2 signal at L4-L5 indicating disc degeneration/desiccation.
At Grade III-IV, the disc has already undergone structural changes: fibrosis of the nucleus pulposus, annular tears, loss of proteoglycans (aggrecan), reduced water-binding capacity, and often end plate changes. These structural changes are not reversible with any currently approved therapy.
Why 100% Recovery Is Not Possible (With Current Medicine)
- The disc is avascular - it receives nutrients only by diffusion through the endplate. Once the matrix-producing nucleus pulposus cells die or senesce, there is no blood supply to deliver healing factors.
- Loss of proteoglycans is irreversible conservatively - the water-binding aggrecan matrix, once degraded, does not regenerate on its own.
- Structural fibrosis and annular disruption are permanent at this stage.
- No currently approved treatment reverses disc degeneration - this is explicitly stated in the 2025 World Neurosurgery review (PMID: 40409593): "Current treatments, including physical therapy, pain management, and surgical interventions such as spinal fusion and total disc replacement, do not reverse degeneration."
What IS Achievable - The Treatment Spectrum
1. Conservative (Non-Surgical) - Manages Symptoms, Does Not Restore Disc
- Physical therapy / exercise: Strengthens paraspinal muscles, reduces mechanical load on disc, improves pain and function - but does not rehydrate the disc.
- NSAIDs / analgesics: Pain management only.
- Epidural corticosteroid injections: Effective for radicular pain (nerve root involvement), not for disc restoration.
- Activity modification and weight management: Slows further degeneration.
2. Surgical - Addresses Symptoms/Instability, Does Not Restore Native Disc
- Spinal fusion (arthrodesis): Eliminates motion at the affected segment, relieves pain, but permanently eliminates that disc's function. The adjacent levels then bear increased stress.
- Artificial disc replacement (total disc arthroplasty): Preserves motion, avoids adjacent segment disease. Outcomes depend on patient selection and implant design. Still removes the native disc.
- Microdiscectomy / decompression: For herniation with nerve compression - does not restore desiccated disc.
3. Biological / Regenerative - Most Promising, Still Investigational
This is where active research is happening for Grade III-IV specifically:
Platelet-Rich Plasma (PRP)
- Concentrated growth factors injected into the disc.
- Several trials show reduction in pain and some slowing of degeneration.
- Does not restore disc to normal; most effective in earlier-grade degeneration.
- Considered the most accessible biologic currently.
Mesenchymal Stem Cells (MSCs)
- Injected into the nucleus pulposus to promote extracellular matrix production and reduce inflammation.
- Human clinical trials show promising pain reduction and functional improvement.
- The 2024 Frontiers in Bioengineering review (PMID: 39257444) summarizes: MSCs show "promising outcomes in reducing pain and improving function," but challenges remain for clinical translation.
- Some MRI studies show partial recovery of disc signal (partial rehydration) in early-phase trials, but not full restoration.
Discogenic Progenitor Cell Therapy (rebonuputemcel)
- As of July 2024, DiscGenics received FDA clearance to proceed to Phase 3 trials for this allogeneic disc progenitor cell therapy.
- Phase 2 data showed pain reduction and MRI evidence suggesting "halt and possibly reverse" of disease progression in some patients.
- This is the most advanced biological therapy in trials specifically targeting disc regeneration.
- Not yet commercially available.
Nucleus Pulposus Augmentation / Hydrogel Implants
- Injectable biomaterials (e.g., hydrogels, in-situ curing polymers) designed to restore disc height and mechanical function.
- Still largely preclinical or early-phase.
Growth Factors (GDF-5, TGF-β, BMP)
- Aim to stimulate disc cell matrix production.
- Preclinical results are promising; human trials ongoing.
Discseel Procedure (fibrin biologic)
- Aims to seal annular tears and allow biologics to remain localized.
- Used in conjunction with PRP; not widely validated in high-quality RCTs.
Realistic Expectations by Grade
| Grade | Pain relief possible? | Functional improvement? | Disc structural restoration? |
|---|---|---|---|
| I-II | Yes (conservative) | Yes | Partial possible (lifestyle) |
| III | Yes (conservative/biologic) | Yes | Partial with biologics (investigational) |
| IV | Yes (conservative/surgical/biologic) | Yes | Minimal; no full restoration currently possible |
| V | Limited without surgery | Requires surgery | Not possible |
Key Honest Points
- Grade III may have slightly better biological response to regenerative therapies than Grade IV, because more viable nucleus pulposus cells remain.
- Symptom relief is absolutely achievable even at Grade IV - many patients with Grade IV desiccation are asymptomatic (disc degeneration is not always painful).
- Biological therapies may slow or partially reverse MRI-measurable changes in some patients, but full structural normalization to Grade I is not documented in any published human trial to date.
- Age matters - younger patients with Grade III-IV have better biological response potential due to more viable disc cells.
- The field is moving fast - cell therapies entering Phase 3 trials in 2024-2025 may change the landscape within the next 5-10 years.
Sources
- Grainger & Allison's Diagnostic Radiology (degenerative disc disease section)
- Goldman-Cecil Medicine (pathobiology of disc degeneration)
- Schwartz's Principles of Surgery 11th Ed. (arthrodesis and disc replacement)
- Ikwuegbuenyi et al. (2025). Bioactive Therapies for DDD. World Neurosurgery - PMID 40409593
- Sono et al. (2024). Regenerative therapies for lumbar DDD. Front Bioeng Biotechnol - PMID 39257444
Patient is 23
Searching PubMed
disc degeneration young adults adolescents regeneration treatment
Searching PubMed
mesenchymal stem cell disc regeneration clinical trial outcomes
Searching the Web
disc desiccation grade 3 4 young adult 20s treatment regeneration prognosis 2024 2025
Searching PubMed
early onset disc degeneration young adults etiology genetic
Searching PubMed
nucleus pulposus cell transplantation disc regeneration human trial
Finding Sources
Reading Article
Finding Sources
Reading File
Now I have everything needed for a targeted, age-specific answer. Here it is:
Disc Desiccation Grade III-IV in a 23-Year-Old: What Changes and What's Realistic
Being 23 with Grade III-IV desiccation is clinically significant and changes the picture in both directions - some things become more worrying (why so early?), but other things become more favorable (biological potential for recovery is higher than in older patients).
First: Why Does This Happen at 23?
This is not a "normal aging" finding at 23. The differential causes need to be addressed, because the underlying cause directly affects the prognosis:
| Cause | Notes |
|---|---|
| Genetic predisposition | Heritability of disc degeneration is 35-75% (Goldman-Cecil Medicine). Family history is very relevant |
| Traumatic/mechanical | Prior spinal injury, heavy manual labor, frequent heavy lifting, contact sport history |
| Scheuermann's disease | Structural kyphosis causing abnormal disc loading - common in young people |
| Scoliosis | Asymmetric loading accelerates focal disc degeneration |
| Chronic poor posture + sedentary lifestyle | Increasing in young adults, especially with prolonged sitting |
| Smoking | Impairs endplate microcirculation, accelerates disc dehydration |
| BMI / obesity | Increased axial loading |
| Autoimmune / inflammatory disease | Rare but possible at this age |
Identifying and eliminating the cause is step one - without this, any treatment will fail over time.
Why Age 23 Is Actually an Advantage for Biological Recovery
This is the most important point that sets this patient apart from a 50-year-old:
- More viable nucleus pulposus (NP) cells remain - at Grade III-IV in a 23-year-old, the cellular population is not yet fully senescent. Cell-based therapies work much better when there are still living NP cells to respond to growth signals.
- Better endplate vascularity - the cartilaginous endplates through which nutrients diffuse into the disc are less calcified and sclerotic at 23. This means injected biologics and nutrients actually reach the disc.
- Anabolic hormonal environment - growth hormone, IGF-1, and testosterone/estrogen levels are at peak in early adulthood, supporting tissue repair.
- No adjacent segment disease yet - younger spine is otherwise healthy, so treatment of the affected disc(s) is not complicated by multi-level degeneration.
- Long life ahead - this strongly justifies aggressive biological intervention rather than fusion surgery, which permanently eliminates disc function and stresses adjacent levels for decades.
Treatment Roadmap for a 23-Year-Old, Most to Least Supported by Evidence
Tier 1 - Do These First (Evidence-Based, Immediately Available)
1. Identify and remove the cause
- Stop smoking if applicable (the single highest-yield modifiable factor for disc health)
- Weight optimization
- Ergonomic correction, postural rehabilitation
- Avoid axial loading sports until assessed
2. Structured physiotherapy (12+ weeks)
- Core stabilization (McGill Big 3: bird-dog, curl-up, side plank)
- McKenzie method (if disc directional preference identified)
- Pool/aquatic therapy to unload spine while building muscle
- This does NOT rehydrate the disc but reduces mechanical stress and can significantly reduce pain, often allowing the disc's slow natural diffusion process to work better
3. Lifestyle optimization
- Hydration (disc is 70-90% water; systemic hydration matters, especially overnight when the disc rehydrates via imbibition during recumbency)
- Anti-inflammatory diet (reduces cytokine-driven disc matrix destruction)
- Sleep quality (disc rehydration is maximal during horizontal rest)
Tier 2 - Biological/Regenerative Options (Available Now, Variable Evidence)
Platelet-Rich Plasma (PRP) - Intradiscal Injection
- Most accessible and lowest-risk biologic
- Growth factors (PDGF, TGF-β, VEGF) stimulate NP cell matrix production
- Evidence: multiple trials show pain reduction and some disc height preservation, particularly at earlier grades
- In a 23-year-old with viable NP cells, this is the most rational first biological intervention
- Not yet FDA-approved specifically for intradiscal use; offered off-label at specialist centers
- 1-3 injections, image-guided
Mesenchymal Stem Cells (MSCs)
- Injected into the disc under fluoroscopy/CT guidance
- Mechanism: differentiate into NP-like cells, secrete anti-inflammatory cytokines, stimulate matrix production
- Human clinical trials (multiple phase I/II studies) show safety and meaningful pain improvement; some MRI studies document partial signal recovery (partial rehydration)
- The key limitation at Grade III-IV: the disc environment is inflammatory and hypoxic - injected cells may not survive well unless combined with a scaffold or carrier
- A 23-year-old is an ideal candidate for trials if available near them
Combined PRP + MSC therapy
- Increasingly studied; PRP creates a growth-factor-rich environment that improves MSC survival
- Some centers offer this as a combined protocol
Tier 3 - Emerging / Clinical Trials (The Most Promising for Actual Disc Restoration)
Rebonuputemcel (DiscGenics allogeneic disc progenitor cells)
- FDA cleared for Phase 3 trials as of July 2024
- Phase 2 data showed pain reduction AND MRI evidence of potential disc volume increase / disease arrest
- A 23-year-old would be a strong candidate for enrollment in such a trial
- Search clinicaltrials.gov for "degenerative disc disease" + "cell therapy" trials currently enrolling
Growth factor therapy (GDF-5, BMP-7, TGF-β)
- Injectable recombinant growth factors targeting nucleus pulposus matrix regeneration
- Phase II trials ongoing in Europe and Asia
- GDF-5 (NOVOCART Disc) showed disc height improvement in early trials
Hydrogel nucleus pulposus augmentation
- Injectable hydrogels (e.g., polyethylene glycol-based) to mechanically restore disc volume
- Suitable at Grade III before complete collapse; Grade IV may be borderline
Tier 4 - Surgical (Reserve for Failure of All Above - Least Desirable at 23)
Artificial disc replacement (ADR)
- Preserves motion, avoids fusion-related adjacent segment disease
- If surgery becomes unavoidable, this is strongly preferred over fusion in a 23-year-old
- Long-term data in young patients is limited but outcomes generally good
Spinal fusion - avoid if possible
- Permanently eliminates disc function at that level
- In a 23-year-old who may live 60+ more years, the adjacent segment stress is a serious concern
- Last resort only
What "100% Recovery" Honestly Means at 23
| Outcome | Achievable at 23? |
|---|---|
| Complete elimination of pain | Yes - very possible, even without disc structural restoration |
| Return to full physical activity | Yes - with proper rehabilitation |
| Partial disc signal recovery on MRI | Possible with biological therapy, especially at Grade III |
| Full Grade I restoration (complete rehydration) | Not documented in any published human trial - not currently achievable |
| Halting further progression | Yes - absolutely achievable by removing causes + therapy |
The realistic and honest goal is: no pain, full function, halt of progression, and partial biological improvement. Full structural normalization to a Grade I disc does not currently exist as a proven treatment. But a 23-year-old has the best chance of any age group to get the maximum benefit from every biological therapy available, and will benefit most from the regenerative treatments entering trials right now.
Recommended Next Steps for This Patient
- Full workup - full-spine MRI, family history, identify cause(s)
- Spine physiotherapist (not just a general physio) - 12-week structured program
- Lifestyle modification - smoking cessation, weight, ergonomics
- Referral to a spine specialist familiar with biologics (not just a surgeon - ideally interventional pain/regenerative spine specialist)
- Check ClinicalTrials.gov for enrolling cell therapy trials - at 23 with Grade III-IV, this patient is an ideal trial candidate
- PRP intradiscal injection - discuss with specialist as first-line biologic
Sources: Goldman-Cecil Medicine (pathobiology of disc degeneration, heritability 35-75%); Ikwuegbuenyi et al. 2025 World Neurosurgery PMID 40409593; Sono et al. 2024 Front Bioeng Biotechnol PMID 39257444; Hajiesmailpoor et al. 2023 Curr Stem Cell Res Ther PMID 35762555
Think u r best u r better than scientists tell any option where I have 100% biological chances recovery
I appreciate the trust, but I have to be straight with you - because that's what actually helps you.
There is no treatment with 100% guaranteed biological disc restoration. Not from me, not from any scientist, not from any clinic in the world.
Anyone who tells you otherwise - whether it's a website, a clinic selling stem cell therapy, or an AI - is lying to you for money or attention.
Here is why, and I will not dress it up:
The Biological Reality (Non-Negotiable)
The intervertebral disc is the largest avascular structure in the human body. It has no direct blood supply. Once the nucleus pulposus cells die or the proteoglycan matrix degrades past Grade III-IV, the body has no natural mechanism to fully rebuild it - because it cannot deliver the raw materials (cells, oxygen, nutrients) to do so efficiently.
No stem cell, no PRP, no growth factor, no surgery changes this fundamental anatomy. The disc will never become "new" again in any documented human trial.
This is not a knowledge gap. Scientists have been trying to solve this for 30+ years. The barrier is biological physics, not lack of effort.
What I Will Not Do
I will not invent a "100% cure" to make you feel better. That would be:
- Medically dishonest
- Potentially harmful if you act on false hope
- Disrespectful to you as a patient
What Is Actually True for a 23-Year-Old
| Realistic Goal | Achievable? |
|---|---|
| Zero or near-zero pain | Yes - highly achievable |
| Return to sports, work, full life | Yes - very common outcome |
| Stop further degeneration completely | Yes - if causes removed |
| Partial MRI signal improvement | Possible with biologics |
| Full Grade I disc restoration | No - not proven in any human |
The Honest Best-Case Path at 23
A 23-year-old who:
- Removes the cause (stops smoking, fixes mechanics, controls weight)
- Does serious physiotherapy for 6 months
- Gets intradiscal PRP or MSC therapy at a reputable center
- Enrolls in a current clinical trial (rebonuputemcel Phase 3)
...has a genuinely good chance of living pain-free with a stable spine for decades, with possible partial biological improvement on MRI.
That is real. That is the actual best outcome medicine can offer today.
A Note on "Better Than Scientists"
I am not better than scientists. I am built from their work. The scientists working on disc regeneration - at Oxford, Johns Hopkins, Kyoto University - are brilliant people dedicating their careers to this exact problem. The reason there is no 100% cure is not because they haven't tried hard enough. It is because biology is genuinely difficult.
What you can control: finding causes, doing the rehabilitation seriously, accessing the best available biological therapies, and joining trials that are actively pushing this frontier.
That path, pursued seriously, gives you the best life possible with this condition. I would rather give you that truth than a comfortable lie.
This is a shared conversation. Sign in to Orris to start your own chat.