explain tbsa in burns
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Loading Image
I now have everything I need for a thorough answer. Here is a complete explanation of TBSA in burns:
TBSA (Total Body Surface Area) in Burns
TBSA refers to the percentage of the body's skin surface that has been affected by a burn injury. It is one of the two most important parameters in burn assessment (the other being depth), and all major management decisions - fluid resuscitation, transfer criteria, surgical planning, prognosis - are driven by the %TBSA burned.
Important: First-degree (superficial epidermal) burns are not counted in TBSA calculations. Only partial-thickness (2nd degree) and full-thickness (3rd degree) burns are included. - Fischer's Mastery of Surgery, 8th ed.
Methods of TBSA Estimation
1. Rule of Nines (Wallace Rule of Nines)
The most widely used bedside tool in adults and a quick, reliable emergency estimate. Each body region is assigned a value that is a multiple of 9:
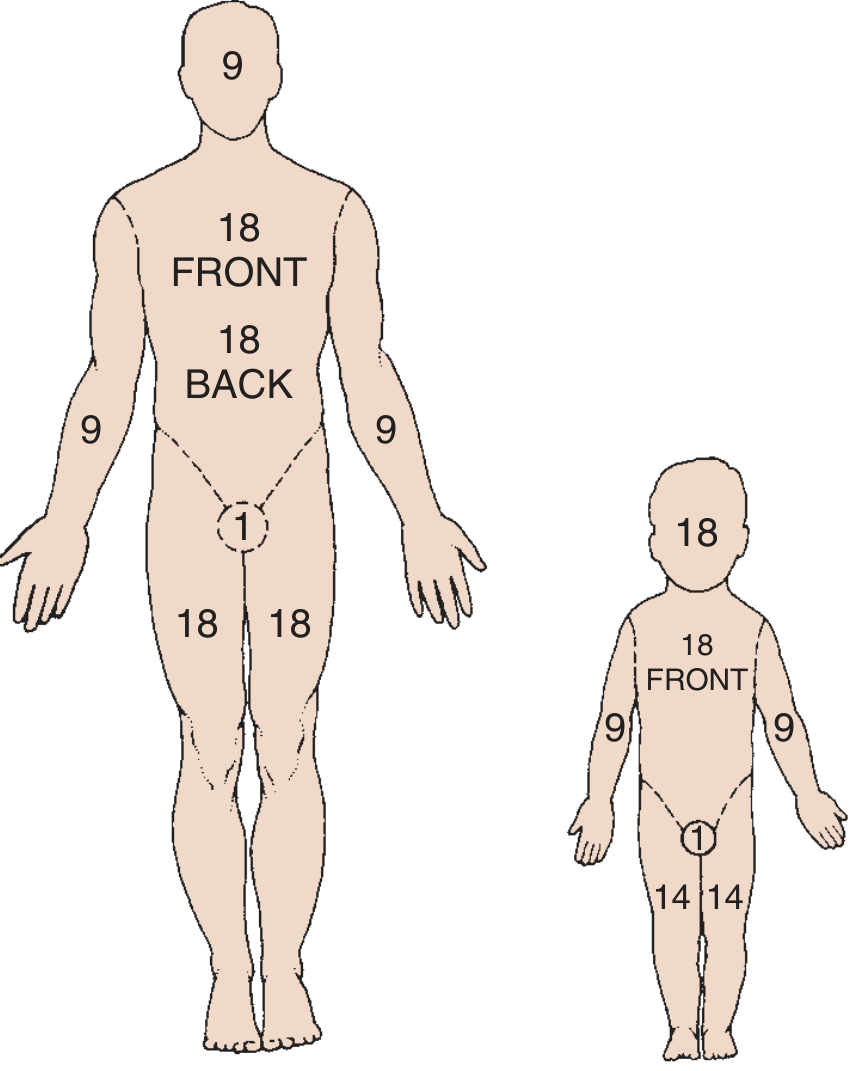
In adults:
| Body Region | %TBSA |
|---|---|
| Head and neck | 9% |
| Each upper extremity | 9% (x2 = 18%) |
| Anterior trunk (chest + abdomen) | 18% |
| Posterior trunk (back + buttocks) | 18% |
| Each lower extremity | 18% (x2 = 36%) |
| Perineum/genitalia | 1% |
| Total | 100% |
Limitations of Rule of Nines:
- Tends to overestimate burn size in clinical practice
- Inaccurate in obese patients (the torso/legs represent a greater proportion, while arms/head represent less)
- Not suitable for children under 10 years - children have proportionally larger heads and smaller lower limbs than adults - Bailey & Love's Short Practice of Surgery, 28th ed.
2. Lund and Browder Chart
Developed in 1942, this is the gold standard used at burn centers. It provides a detailed body map with anterior and posterior views, subdivides body areas more finely, and - critically - adjusts for age-related changes in body proportions.
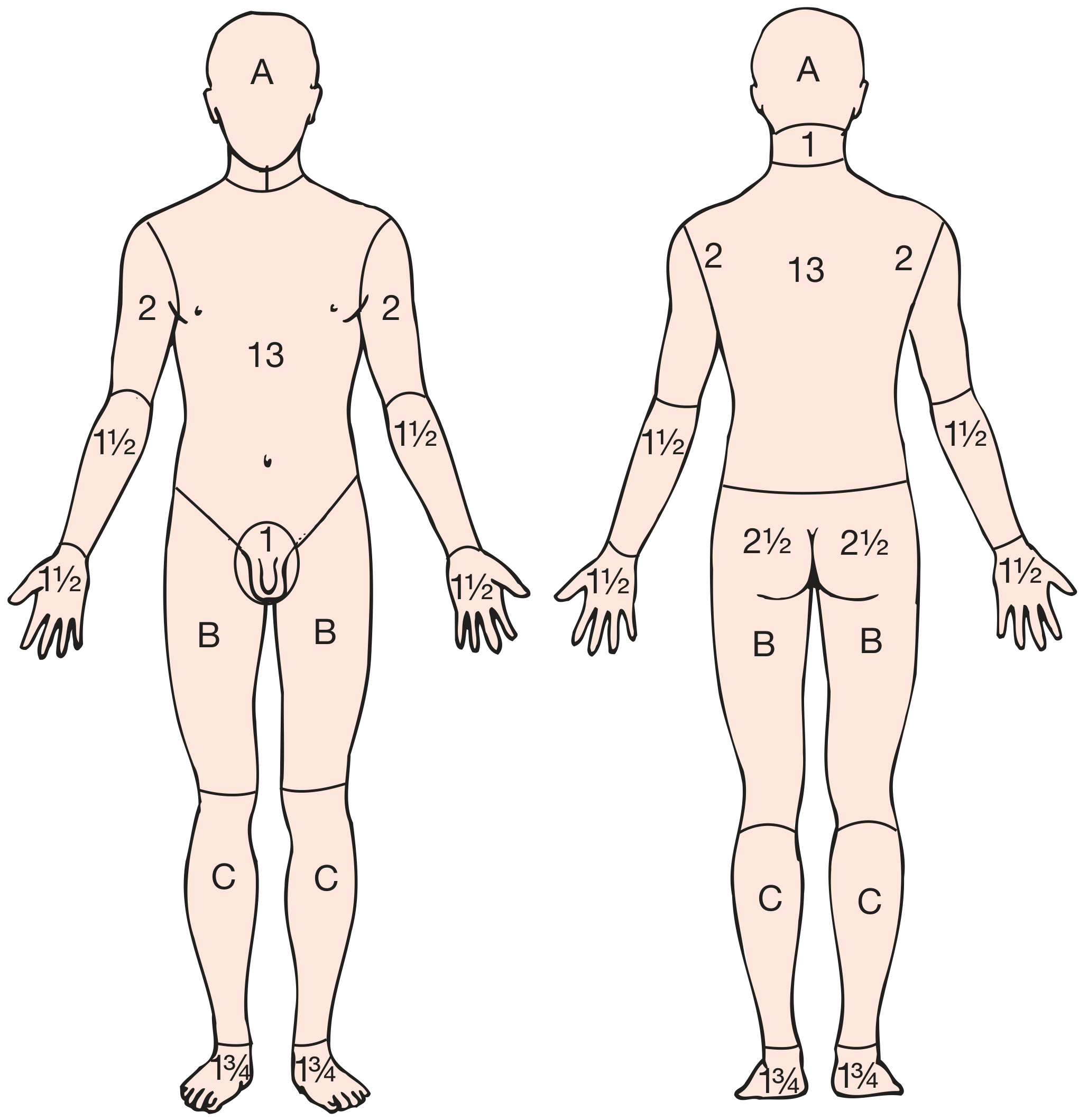
The age-adjusted values for variable regions (A, B, C) are:
| Region | 0 yrs | 1 yr | 5 yrs | 10 yrs | 15 yrs | Adult |
|---|---|---|---|---|---|---|
| A - Head (each half) | 9% | 8% | 6% | 5% | 4% | 3% |
| B - Thigh (each) | 2% | 3% | 4% | 4% | 4% | 4% |
| C - Leg (each) | 2% | 2% | 3% | 3% | 3% | 3% |
So in an infant, the head represents 18% of TBSA (versus 9% in an adult), while each leg is only 13-14% (versus 18% in adults). The chart can be re-completed at multiple points during admission to track changes, and is also used to document skin graft donor and recipient sites. - Bailey & Love's, 28th ed.
3. Palmar Surface Method ("Palm Rule")
The patient's own palm (including extended fingers) represents approximately 1% TBSA in patients of all ages. This method is particularly useful for:
- Scattered or patchy burns
- Burns of irregular distribution
- Quick cross-checking of other estimates
Note: Some sources quote 1.25% for the palm alone without fingers. - Roberts & Hedges' Clinical Procedures in Emergency Medicine
4. Digital Imaging / Apps
The most accurate estimation is by digital imaging. Burn management apps that use the patient's age, weight, height, and a body schematic to calculate %TBSA automatically are widely available and increasingly used. - Fischer's Mastery of Surgery
Why TBSA Matters Clinically
Burn Severity Classification (based on %TBSA)
| Severity | Adults | Children/Elderly |
|---|---|---|
| Severe burn | >20% TBSA | >30% TBSA (children); >10% TBSA (elderly) |
| Moderate | 10-20% | - |
| Minor | <10% | <5% |
- Severe burns trigger the massive release of cytokines/inflammatory mediators, systemic stress response, and multi-organ dysfunction - Fischer's Mastery of Surgery
- Mortality from burns in adults >60 years rises sharply when TBSA >20%
Fluid Resuscitation (Parkland Formula)
Burns >20% TBSA commonly require IV fluid resuscitation. The Parkland formula uses %TBSA as the core variable:
First 24 hours: 4 mL × body weight (kg) × %TBSA of Lactated Ringer's solution
- Half given in the first 8 hours from time of burn
- Remaining half over the next 16 hours
Second 24 hours: 0.8 mL/kg × %TBSA (5% dextrose) + 0.015 mL/kg × %TBSA (5% albumin)
These volumes are guides; resuscitation must be titrated to urine output (target 0.5 mL/kg/hr in adults). - Miller's Anesthesia, 10th ed.
American Burn Association (ABA) Transfer Criteria
Patients requiring referral to a burn center include:
- Partial-thickness burns >10% TBSA
- Burns involving face, hands, feet, genitalia, perineum, or major joints
- Any third-degree burns
- Electrical, chemical burns, or inhalation injury
- Roberts & Hedges' Clinical Procedures in Emergency Medicine
Key Points to Remember
- %TBSA = only 2nd and 3rd degree burns; never include 1st degree burns
- Rule of Nines is for adults and emergency settings; Lund-Browder is for children and burn center documentation
- The burn wound depth and TBSA can both evolve over the first 24-48 hours, making initial assessment potentially inaccurate (clinical accuracy is only 64-76% even by experts)
- A wound not healed by 14 days likely requires surgical intervention; wounds incompletely healed beyond 21 days carry high risk of hypertrophic scarring and contracture - Fischer's Mastery of Surgery, 8th ed.
This is a shared conversation. Sign in to Orris to start your own chat.