Bimalleolar fracture treatment
Reading File
Searching the Web
bimalleolar fracture treatment ORIF guidelines 2024
Searching PubMed
"bimalleolar fracture" AND treatment
Finding Sources
Searching PubMed
"ankle fracture" AND "bimalleolar" AND fixation
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive information from Campbell's Operative Orthopaedics (2026 edition). Let me compile a thorough response.
Bimalleolar Fracture - Treatment
Source: Campbell's Operative Orthopaedics, 15th Ed., 2026 - Chapter 59
Overview
Bimalleolar ankle fractures disrupt both the medial and lateral stabilizing structures of the ankle, making the joint mechanically unstable. Displacement reduces tibiotalar contact area and alters joint kinematics. Closed reduction can often be achieved but rarely maintained as swelling subsides. Key facts that drive management:
- ~10% nonunion rate with closed (conservative) treatment
- 20% of bimalleolar fractures have intraarticular injuries to the talus and tibia - these go untreated when closed methods are used
- Randomized, prospective, and long-term follow-up studies demonstrate superior results with operative over nonoperative treatment, including for supination-external rotation (SER) Stage IV fractures
Classification (Danis-Weber)
| Type | Level of Fibular Fracture | Syndesmosis |
|---|---|---|
| A | Below the plafond | Intact |
| B | At the level of the plafond | Partially disrupted |
| C | Above the plafond | Disrupted |
Treatment Decision
Non-operative (rare)
Reserved for:
- Truly non-displaced, stable fractures
- Patients with significant surgical contraindications (poor soft-tissue condition, severe medical comorbidities, very elderly/frail patients)
- Management: below-knee cast, non-weight-bearing x 6 weeks
Operative - ORIF (recommended for most displaced fractures)
ORIF of both malleoli is recommended for most displaced bimalleolar fractures.
Lateral Malleolus Fixation
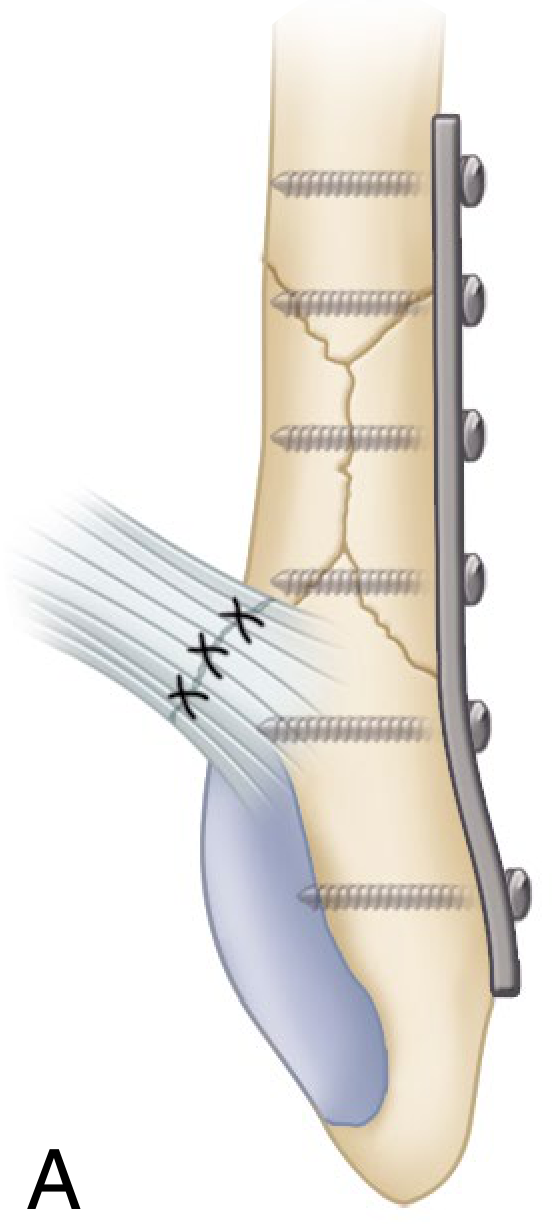
Fig. 59.3A - Standard fixation: 1/3 semitubular 3.5 mm plate with screws (most common)
Options for lateral malleolus fixation:
- Plate and screw fixation (Weber B & C) - standard lateral plate with 3.5 mm screws
- Posterior antiglide plating - avoids intraarticular screws, decreases palpable implants, stronger construct; risk of peroneal tendinitis (~30% peroneal tendon injury after implant removal)
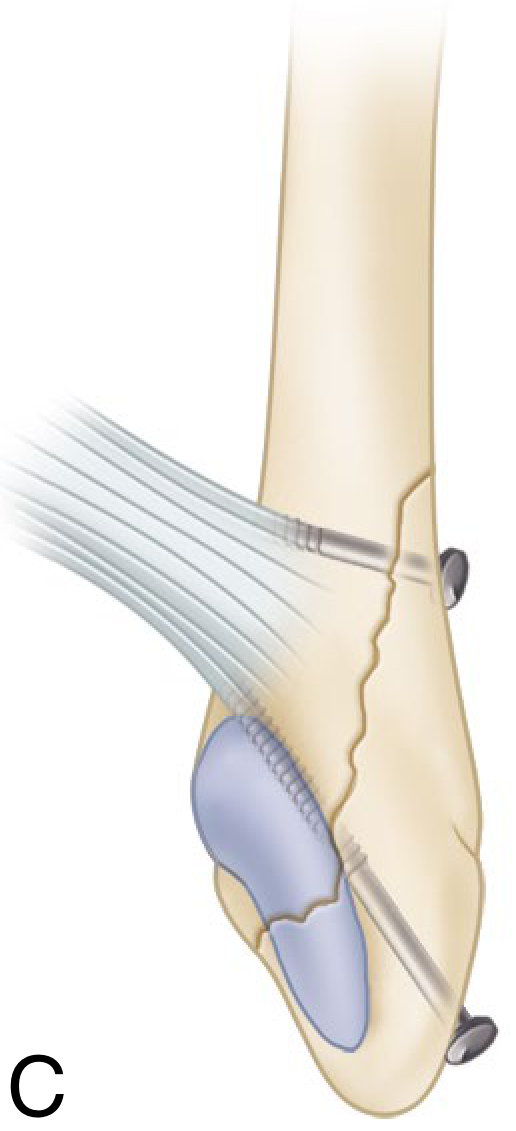
- Lag screw-only technique - for simpler oblique fractures; less implant prominence and pain; ideal candidates are patients <50 years with simple oblique fracture, minimal comminution, allowing 2 lag screws at least 1 cm apart
- Intramedullary screw - 3.5 mm IM screw for select fracture patterns (Fig. 59.3F)
- Tension band wiring with 4 mm lag screw - used in some configurations (Fig. 59.3E)
In osteopenic bone, Kirschner wires augmenting plate fixation improve resistance to bending.
Medial Malleolus Fixation
- Two partially threaded cancellous lag screws - standard technique
- Tension band wiring with K-wires - often preferred for small fragments or comminuted fractures
- 4 mm malleolar screw - for small or low fractures
Timing of Surgery
Surgery is ideally performed in two time windows:
- Within 12 hours of injury (before significant swelling)
- 2-3 weeks after injury (after swelling has resolved)
In between, surgery may be technically hazardous (soft tissue envelope at risk). Equally good functional results have been shown with immediate vs. delayed ORIF, though:
- Hospitalization is briefer with immediate surgery
- Pain scores are lower with immediate surgery
- Delayed surgery is justified for severe soft-tissue injury or fracture blisters
If open reduction must be delayed, immediate closed reduction + splinting is mandatory to prevent skin necrosis over a fracture-dislocation.
Syndesmotic Injury Assessment & Fixation
Syndesmosis disruption is common with Weber C fractures and some Weber B fractures.
Intraoperative assessment:
- Cotton Test - bone hook distraction of fibula from tibia; >3-4 mm lateral displacement = syndesmotic fixation needed
- External rotation stress test under fluoroscopy after lateral malleolar fixation
Syndesmotic fixation is indicated for:
- Syndesmotic injuries associated with proximal fibular fractures where fixation is not planned, plus an unstabilizable medial injury
- Syndesmotic injuries extending >5 cm proximal to the plafond
- Injuries extending >3-4.5 cm from the plafond with medial injury
Fixation options:
- Trans-syndesmotic screws (traditional 3.5 or 4.5 mm cortical screw)
- Suture-button (TightRope) devices - allow physiologic micro-motion and eliminate the need for screw removal
- Similar functional outcomes have been shown with deltoid ligament repair + posteroinferior tibiofibular ligament repair vs. trans-syndesmotic fixation
Postoperative Rehabilitation (General Timeline)
| Phase | Timeframe | Key Focus |
|---|---|---|
| Phase I | Weeks 0-6 | NWB or toe-touch WB in boot/cast; edema control; ankle ROM exercises |
| Phase II | Weeks 6-12 | Progressive WB to full WB; strengthening begins; balance/proprioception |
| Phase III | Weeks 13-16 | Full WB; bilateral then unilateral heel raises; balance on uneven surfaces |
| Phase IV | Weeks 17-20 | Plyometrics; sport-specific movement patterns; return to activity |
If syndesmotic repair was performed: strict NWB for 6 weeks minimum.
Complications
- Wound complications / infection - especially with delayed or early surgery in swollen tissue
- Nonunion / malunion - reduced significantly vs. closed treatment
- Posttraumatic arthritis - risk increased with intraarticular injuries (present in 20% of bimalleolar fractures)
- Implant prominence / irritation - common, especially with lateral plates; only ~50% get relief after implant removal
- Peroneal tendon injury - reported in 30% after removal of posterior antiglide plate due to screw tract
- Syndesmotic malreduction - associated with poor long-term outcomes
Key Evidence
-
Operative vs nonoperative medial malleolus RCT (JAMA, 2024) - RCT comparing operative vs. nonoperative management of unstable medial malleolus fractures [PMID: 38236603]
-
Posterior malleolus ORIF systematic review (Foot Ankle Int, 2023) - systematic review showing improved patient-rated outcomes when posterior malleolus fragment is fixed [PMID: 37125766]
-
Campbell's Operative Orthopaedics, 15th Ed., 2026, Chapter 59, pp. 3323-3325
This is a shared conversation. Sign in to Orris to start your own chat.